

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The association between androgens and cardiovascular diseases (CVDs) remains controversial. For many years, androgenic hormones have been associated with an increased risk of CVDs [1]. This has been largely based on the gender disparity in the incidences of CVDs, with a higher male predisposition [1]. Further, abuse of anabolic steroid by athletes has been linked to various adverse effects in the cardiovascular system including thrombosis, hypertension as well as heart failure [2]. However, recent evidence from various population-based and animal studies demonstrates beneficial effects of physiological levels of androgens on the cardiovascular system.
These beneficial effects are consistent with the higher incidence of atherosclerosis [34], aneurysms [5], heart failure and coronary artery disease [6] among hypogonadal males. The hypogonadism may be due to age-related decline in endogenous androgen levels [78], androgen deprivation therapies [9], and disorders that either damage the testis or reduce gonadotropin stimulation [1011]. The basis for higher prevalence of CVD among hypogonadal men has been explored in biochemical and physiological models and has been attributed to adverse effects of androgen insufficiency on lipid profiles [3]. Low androgen levels are associated with increased concentrations of atherogenic low density lipoproteins, cholesterol, and triglycerides and decreased concentrations of high density lipoproteins [121314]. It has however been demonstrated that the higher incidences of CVD in hypogonadism are only partly mediated through a lipid-mediated effect [12]. Although it is known that androgen insufficiency as seen in hypogonadism is associated with endothelial dysfunction [915], structural changes in the vascular wall that may constitute an anatomical basis for the higher prevalence of CVD among hypogonadal men are largely unexplored. This study therefore aims to describe structural changes in the common carotid artery (CCA) of male rat following orchiectomyinduced hypogonadism.
Materials and Methods
This was a non-randomized trial (quasi-experimental) using the rat model. A total of 22 male rats aged 2 months were used in this study. Rats were used as the study model because of their ease of handling, low maintenance cost and close physiological resemblance to man. Further, the structure of the rat CCA is similar to that in man. Two-month-old rats were used because this is the age at which they attain sexual maturity. Rats with visible neck or scrotal pathology were excluded. The animals were housed in cages floored with wood shavings that were changed regularly. They were kept in their cages for 2 weeks prior to commencement of the study for acclimatization. The animals were placed under a normal 12 hours' light/dark diurnal cycle and provided with standard rat pellets and water ad libitum. Ethical approval to conduct the study was granted by the Biosafety, Animal Care and Use committee of Nairobi University, Nairobi, Kenya (Ethical approval number: FVMBAUEC/2016/96).
Four rats were chosen using simple random sampling technique to demonstrate the baseline (day 0) histomorphology of the CCA. The remaining rats were divided randomly into two groups (11 experimental, 11 controls). Hypogonadism was induced in the experimental via bilateral orchiectomy under local anesthesia. The animals were placed in the dorsal recumbent position and under physical restrain. The scrotal skin disinfected using iodine solution. Two milliliters of 1% lignocaine was injected in the around the scrotal sac to provide local anesthesia. A 1.5-cm incision was made at the base of the hemi-scrotal sacs. Subcutaneous tissue was bluntly dissected to reveal the vaginal processes. This was then excised to access the testis and the spermatic cord which were then gently exteriorized. The spermatic cord was then clamped, ligated and removed together with the testis and epididymis. A 4-0 suture was then used to close the processus vaginalis. This procedure was repeated on the contralateral hemi-scrotal sac. The skin was thereafter closed with a 2-0 non-absorbable interrupted sutures. The wound was then covered with a cotton wool soaked in iodine and secured with a bandage.
On experimental week 3, 6, and 9, three animals from both groups were picked randomly, euthanized and perfused with normal and formal saline solutions. Their CCA were harvested and processed for paraffin embedding and sectioning. The rats' CCA were fixed in 10% formalin for twelve hours. This was followed by dehydration in increasing grades of alcohol (70% up to absolute alcohol) at one hour intervals, and clearing in toluene. Thereafter, the vessels were placed in the memmert oven for wax infiltration. The CCA were embedded in paraffin wax and oriented for transverse sectioning. After cooling, the embedded tissues were blocked using wooden blocks and then serially cut into 7-µm sections using a microtome. Fifteen 7-µm sections were randomly obtained from the ten ribbons, floated on a 60℃ water bath and picked on a glass slide, then dried in an oven for 12 hours. Masson's Trichrome was used to display smooth muscle cells and collagen fibers while Wiegerts stain was used to display elastic fiber profile. Hematoxylin and eosin was used to display the smooth muscle cell nuclei in the CCA.
Photomicrographs of the sections were taken using a digital camera (Canon Powershot A640, 12 mp, Beijing, China) mounted on a photomicroscope (Carl Zeiss, Axiostar Plus Microimaging, Jena, Germany) for stereological analysis using the Fiji-ImageJ. This is an open source software developed by the United States National Institute of Health for processing and analyzing images. The variables obtained include volumetric densities of collagen fibers, elastic fibers, and smooth muscle cells (in %). Histomorphological changes of the vessel wall were also described. The collected were entered into the SPSS software version 21 (IBM Corp., Armonk, NY, USA) for coding, tabulation and statistical analysis. Volumetric densities are expressed in frequencies (%). The data were groupd: control group (non-castrated) and experimental (castrated) group. After confirming that the data was not normally distributed (using box plots and histograms), non-parametric tests were used for univariate analysis. Kruskal-Wallis H-test was used to compare the medians of the volumetric densities of collagen fibers, elastic fibers, and smooth muscle cell nuclei along the various harvesting periods within each group while Man-Whitney U test was used to compare the medians of the above variables between control and experimental groups. A P-value <0.05 was considered significant at 95% confidence interval. Data are presented in tables and photomicrographs.
Results
The CCA displayed features of an elastic artery with three conventional tunics; tunica intima (TI), media (TM), and adventitia (TA). TI consisted of a single layer of endothelial cells lying on a thin sub-endothelial connective tissue. TM was the most prominent layer, being made up of 3–5 thick continuous elastic lamellae with smooth muscle cells and collagen fibers interspersed between them. TA comprised of thick collagen fiber bundles running circumferentially around the vessel wall. Elastic fibers were also identified in this layer.
Intima hyperplasia
Androgen deprivation resulted in the development of focal intimal thickenings in the CCA of castrated animals. These thickenings were composed of collagen fibers and smooth muscle cells (Fig. 1D, F).
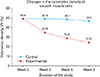
Decreased smooth muscle cell density
There was a progressive decrease in the smooth muscle cells count in the CCA of the castrated animals from 48.84% at baseline to 34.38%, 28.35%, and 24.25% in week 3, 6, and 9, respectively (P<0.001) (Fig. 2), with that in the control animals remaining fairly constant, being 48.79%, 48.1%, and 46.3% in week 3, 6, and 9, respectively (P=0.414). Moreover, castration resulted in reduced thickness of the smooth muscle bundles, coupled with a decrease in medial smooth muscle cell nuclei as demonstrated with hematoxylin and eosin stain (Fig. 1A–D).
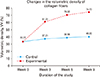
Increased deposition of collagen fibers
Castration resulted in vascular fibrosis with a progressive increase in the CCA collagen fiber density (Fig. 1C, D), from 33.22% at baseline to 61%, 70.52%, and 74.23% at week 3, 6, and 9 after castration respectively (P<0.001) (Fig. 3). There were however no statistically significant changes in the collagen fiber density in control rats across the study period (P=0.216). Further, there was disruption of the lamellae organization of collagen fiber bundles in the TA of castrated rats as evidenced by wider spaces between the collagen fibers.
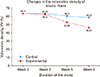
Disruption of elastic lamellae organization
Androgen deprivation resulted in the disruption of the lamella organization of medial elastic lamellae in the CCA of castrated rats (Fig. 1E, F). While the CCA of control rats had thick continuous medial elastic lamellae running circumferentially around the vessel wall, there was a reduction in the thickness coupled with fragmentation of these elastic lamellae in the TM of castrated. Further, there was a significant decrease in the elastic fiber density in the CCA of castrated rats (Fig. 1E, F), from 63.4% at baseline to 62.4%, 52.89%, and 46.34% at week 3, 6, and 9, respectively (P=0.014) (Fig. 4). There were however no statistically significant changes in the elastic fiber densities in control animals across the study period (P=0.074).
Discussion
Higher incidences of CVD have been reported among hypogonadal males compared to their normogonadic counterparts. The structural basis for this predisposition however remains relatively underexplored.
In the current study, orchidectomy resulted in the development of intimal hyperplasia (IH). Non-induced IH in hypogonadal states remains hitherto undescribed to the best of our knowledge. Previous studies focused mainly on effects of exogenous testosterone on the size of mechanically-induced carotid atherosclerotic plaque, reporting a reduction in the plaque area following treatment of the animals with exogenous testosterone [1216]. Similarly, population-based studies have reported an inverse correlation between the levels of endogenous androgens and the presence of carotid and aortic atherosclerotic plaques [1718]. Since IH normally precedes the formation of an atherosclerotic plaque, all are therefore in agreement that that low levels of androgens are associated with IH.
The IH observed in the current study could be attributed to the increased production of pro-inflammatory cytokines [19] and urotensin II [20] that normally occurs in hypogonadal states. The former is known to cause endothelial damage [19], while the latter is involved in the stimulation of vascular smooth muscle cell proliferation and migration [21] as well as the recruitment of macrophages into the vascular wall [22]. Both processes are crucial in the pathogenesis of IH. Since the rate of development of the IH in the current study was proportional to the duration of exposure of the animals to hypogonadism; and that IH normally precedes atheroma formation, it is plausible to postulate the IH would have developed into an atherosclerotic plaque had the animals been followed up for a longer duration of time. The progressive occlusion of the vessel lumen in atherosclerosis is known to compromise vascular supply to vital organs such as the brain and heart. The observations of the current study may therefore partly explain the higher incidences of myocardial ischemia [6] as well as stroke [23] among hypogonadal men.
The present study reports a decrease in vascular smooth muscle composition following orchidectomy-induced hypogonadism. This is in agreement with previous studies that reported decreased penile trabeculae smooth muscle cells [2425] as well as cardiomyocytes [2627] in hypogonadal states. Studies have also reported disorganization of smooth muscle cells and decreased myofilament quantity in castrated animals [2428]. This decrease may be attributed to increased programmed cell death, atrophy and dedifferentiation into other phenotypes [28]. Androgen deprivation is known to result in the upregulation of angiotensin II (AT2) receptors within the vascular wall [2729]. These receptors are known to activate caspases [26], the primary mediators of apoptosis, while causing the downregulation of anti-apoptotic molecules, B-cell lymphoma 2 [27]. Another possible explanation for the decrease in smooth muscle cells may be androgen deficiency-associated atrophy. Although we could not find any published literature detailing atrophy of vascular smooth muscles in hypogonadal states, androgen deprivation in animals have shown to induce atrophy of penile cavernosal smooth muscle cells [243031]. This is supported by skeletal muscle atrophy and fatigue normally observed in hypogonadal men [432]. The decrease in smooth muscle cells can also attributed to their dedifferentiation into other phenotypes. Unlike skeletal or cardiac muscle cell that are terminally differentiated, smooth muscle cells retain remarkable plasticity and can undergo phenotypic changes in conditions such as vascular wall injury [33]. Concordant with this, surgical castration as well as blockade of 5α reductase has been demonstrated to cause dedifferentiation of prostate smooth muscle cells into fibroblasts [3435]. Furthermore, it is known that androgens induce mesenchymal stem cells into the smooth muscle cell lineage, and androgen deficiency accordingly causes these stem cells to follow adipocyte lineage [31]. However, we did not identify any deposition of adipose tissue within the vessel wall. Vascular smooth muscle cells are important in regulation of vascular tone, blood pressure and wall integrity [36]. Decreased smooth muscle cell quantity is associated with various arterial pathologies such as aneurysms [37], hypertension [36], vascular calcification as well as rapture of atherosclerotic plaque [38]. Therefore, decreased smooth muscle density observed in this study may provide a structural basis for the higher incidences of aneurysms as well as hypertension among hypogonadal men [5].
The present study also demonstrates that castration results in increased volumetric density of vascular collagen fibers, proportional to the duration of hypogonadism. Similar changes have been reported to occur in the penis [242539] and myocardium [4041] in studies involving androgen hormone deficiency. These results supported by the observation that androgen receptor knockout in mice exacerbates cardiac fibrosis [42]. Increased collagen fiber could be attributed to accumulation of fibroblasts within the vessel wall or their differentiation into a more proliferative and synthetic phenotype, myofibroblasts [43]. Various pathways involved in increased collagen fiber synthesis in hypogonadal states have been described. It is known that androgens have an inhibitory effect on the production of transforming growth factor β (TGF-β) by various inflammatory cells such as macrophages and monocytes [44]. Thus, androgen ablation results in the upregulation of TGF-β production [1945], resulting in the activation of fibroblasts, with increased production of extracellular matrix [46]. TGF-β also induces the differentiation of these fibroblasts into more synthetic types, the myofibroblasts [47]. Another possible explanation for the decrease in smooth muscle cells is the upregulation of AT2 production and expression in cardiomyocytes and vascular smooth muscle cells [27]. AT2 promotes fibrosis by activating fibroblasts as well as enhancing their differentiation into myofibroblasts, with increased production of extracellular matrix [48]. Collagen fibers are important for structural support of the vessel wall by preventing overstretching during systole [49]. Their excess production however leads to stiffening of arteries, reducing vessel compliance [50]. This also occurs with aging and has been implicated in the pathogenesis of hypertension [50]. Therefore, vascular fibrosis observed in this study constitutes a possible structural basis that could partly explain the higher prevalence of hypertension among hypogonadal men.
The present study also demonstrates that androgen deprivation by castration results in decreased quantity of adventitial elastic fibers, coupled with fragmentation of medial elastic lamellae. Changes in vascular elastic fibers and medial elastic lamellae with hypogonadism remain hitherto undescribed, although similar findings have been reported in the penile elastic fiber system [253951] and in vascular aging [5253].
The molecular mechanisms underlying elastic fiber reduction and fragmentation of medial elastic lamellae in hypogonadism remain relatively unexplored. However, matrix metalloproteinases (MMPs), particularly MMP2 and MMP9 have been shown to have high affinity for elastin and are involved in their degradation during extracellular matrix remodeling [545556]. These MMPs can be activated by various cytokines such as TGF-β and tumor necrosis factor α [5758]. Since expression of these cytokines is normally upregulated in hypogonadal states [19], it is possible that the decrease in elastic fibers as well as elastic lamellae fragmentation observed in this study is attributed to cytokine-mediated MMP degradation. Furthermore, some workers have argued that androgens regulated protein synthesis of connective tissue, and decrease in their production could therefore give rise to the switch from elastic fibers to collagen fibers, forming another possible basis for the decreased elastic fiber density [59]. The decrease in volumetric density of elastic fibers suggests a higher rate of degradation by MMPs compared to the rate of deposition by fibroblasts.
Together with collagen fibers, elastic fibers and lamellae are important in maintaining the compliant nature of dynamic structures such as arteries [60]. They are integral to the windkessel mechanism that enables conduit arteries such as the aorta to deform during systole and use the stored energy to recoil to their original states during diastole, thereby driving blood through the circulatory system [5356]. However, with aging, there is loss of elastic fibers as well as fragmentation of elastic lamellae [6162]. As such, the load is transferred to collagen fibers, which are stiffer, resulting in loss of vessel compliance [56]. Such changes are known to cause an increase in systolic blood pressure, a key risk factor for the development of heart failure [5361]. Also, fragmentation of elastic lamellae results in loss of integrity of the vessel wall, which contributes to aneurysmal dilatations [6364].
The results of this study therefore suggest that androgen deprivation results in loss of vessel compliance due to elastic fiber and lamellae degradation. This is consistent with the increased arterial stiffness is patients receiving androgen deprivation therapies [6566]. These results may therefore explain the higher incidences of heart failure [6] as well as aneurysms [5] in hypogonadal men.
Limitations
Castration is a surgical procedure that causes tissue injury. Therefore, some of the changes observed in this study may have been due to reactive processes to tissue injury. However, based on the fact that the changes observed in this study were proportional to the duration of androgen deficiency, they are most likely to be due to gonadal hormone deficiency rather than surgical trauma. We were unable to determine whether the decrease in smooth muscle composition was as a result of atrophy, apoptosis or both.
Nonetheless, this is the first study to the best of our knowledge, to detail changes in the vascular structure in induced hypogonadism. The results of the current study may constitute an anatomical basis for the higher incidences of CVDs among hypogonadal males.

 XML Download
XML Download