

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The external carotid artery (ECA) and its branches serve as the major vascular channels of the head and neck region. The ECA arises in the carotid triangle from the common carotid artery (CCA) along with the internal carotid artery (ICA). The ECA is the main feeding vessel to the tissues of the head and neck region through its 8 branches, namely the superior thyroid artery (STA), ascending pharyngeal artery (APA), lingual artery (LA), facial artery (FA), occipital artery, posterior auricular artery (PAA), superficial temporal artery, and maxillary artery. In addition, the ECAs also play an important role in providing collateral blood supply to the brain through the many connections between the branches of the ECA and cranial branches of the ICA and vertebral arteries [1]. Injuries to the carotid arteries in cases of neck trauma is the cause of inaccessible exsanguinating haemorrhage, requiring emergency surgical intervention [23]. Pseudoaneurysms occurring consequent to blunt carotid injury commonly affect branches of the ECA than the main ECA itself [4]. The clinical significance of the ECA and its branches is further reinforced by their application in a wide range of radiological and surgical procedures such as intra-arterial infusion chemotherapy [56], carotid stenting and endarterectomy [78] as well as various head and neck surgeries [91011]. A comprehensive understanding of the normal as well as variant anatomy of the ECA is hence essential for the discerning radiologist as well as the judicious surgeon for successful completion of procedures and avoidance of vascular complications in the head and neck region.
Materials and Methods
The present prospective study was done over a period of 4 years from 2012 to 2016 after obtaining clearance from the institutional ethical clearance committee. 80 hemi-necks obtained from 40 formalin embalmed cadavers (32 male ad 8 female) were dissected and the external carotid arteries were traced from the origin to termination. Cadavers in which embalming had been done through CCA and those with injuries in the head and neck region were excluded from this study. The cadavers were aged between 50 and 80 years. Variations encountered in the origin and branching pattern of the ECA were documented with digital photography. The data was tabulated and the percentage of cadavers with variations in the branching pattern of ECA as well as variations in the level of the carotid bifurcation were computed and analysed.
Results
Variations in the level of carotid bifurcation
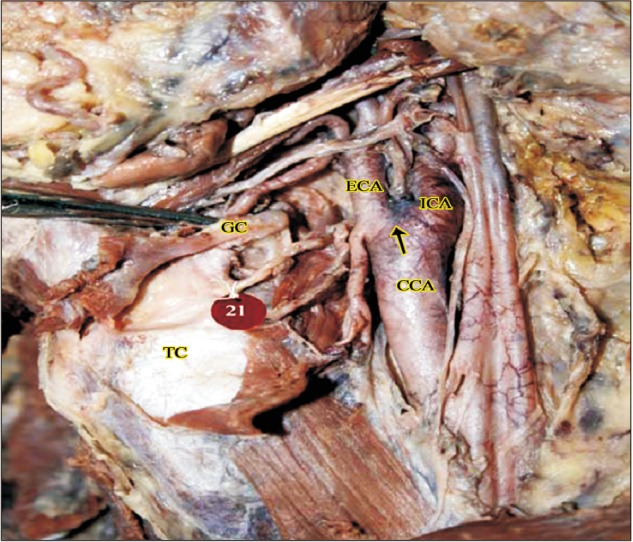
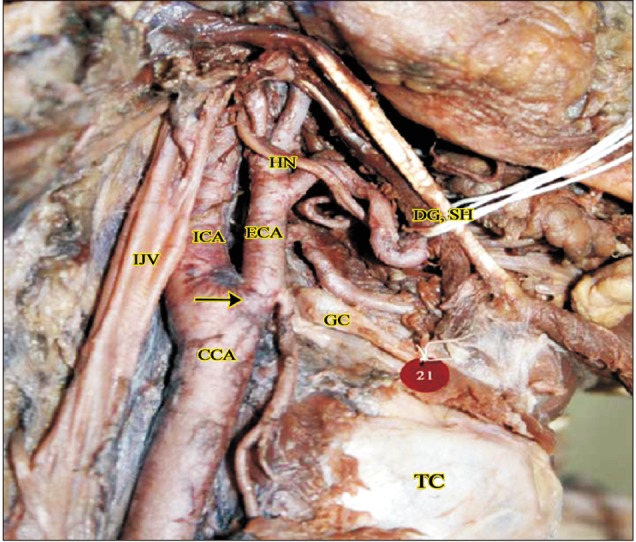
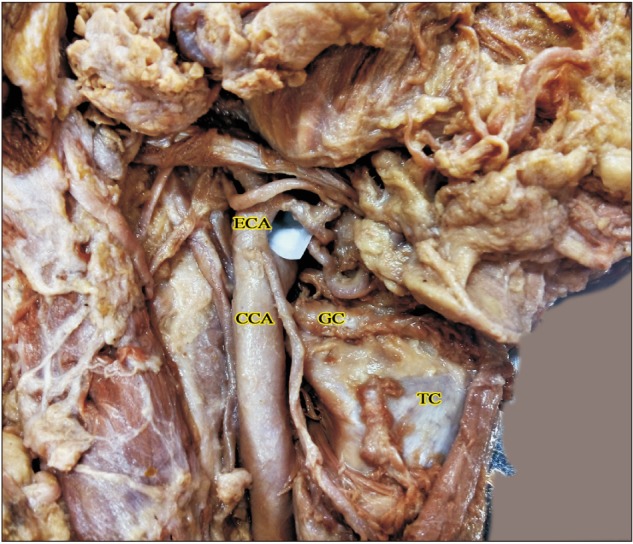
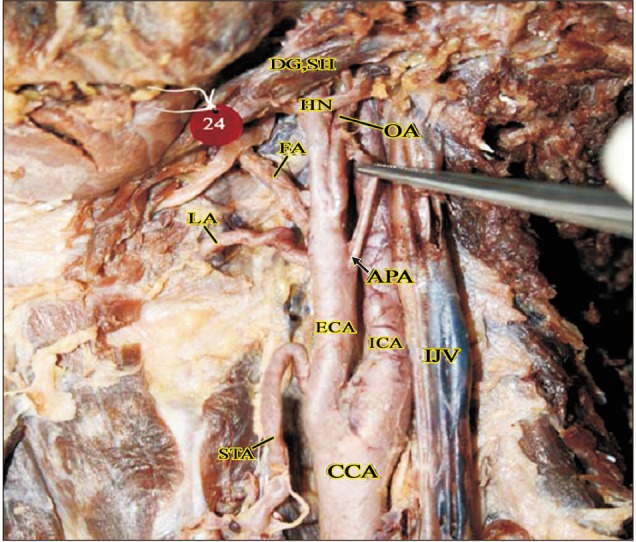
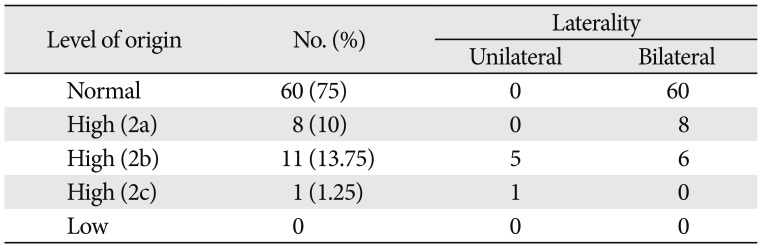
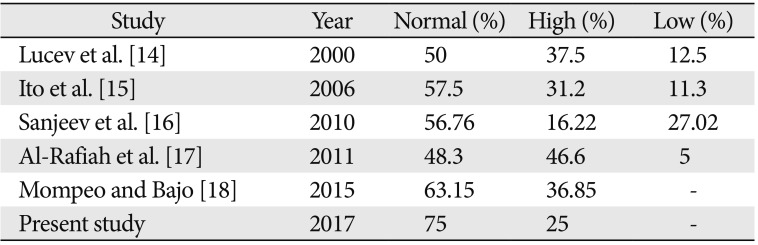
The ECA took origin at the level of upper border of thyroid cartilage (TC) in 60/80 cases (75%). Higher level of origin was noted in the remaining 20 of 80 cases (25%). Higher levels of carotid bifurcation were further categorized keeping the TC as anatomical landmark (Table 1, Figs. 1,2,3). No lower levels of origin were noted in this study. The anteromedial position of the ECA relative to the ICA at the level of the carotid bifurcation was noted in all the cases.
Variations in the branching pattern
Anterior branches
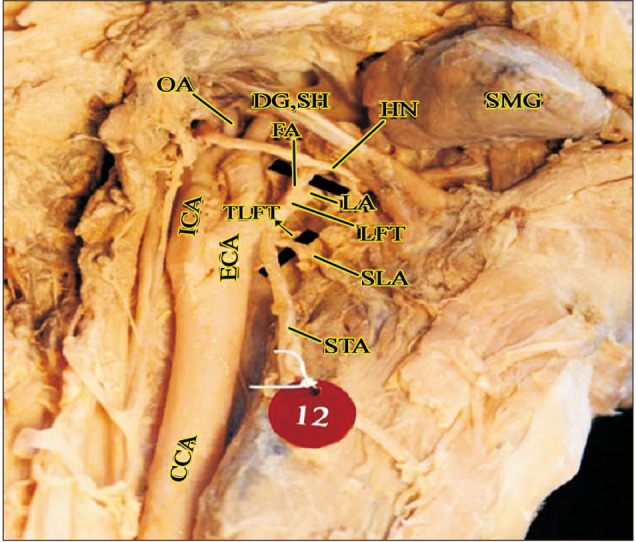
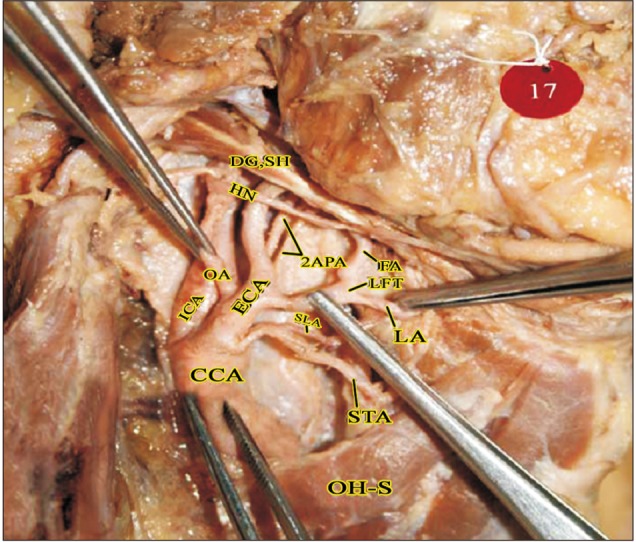
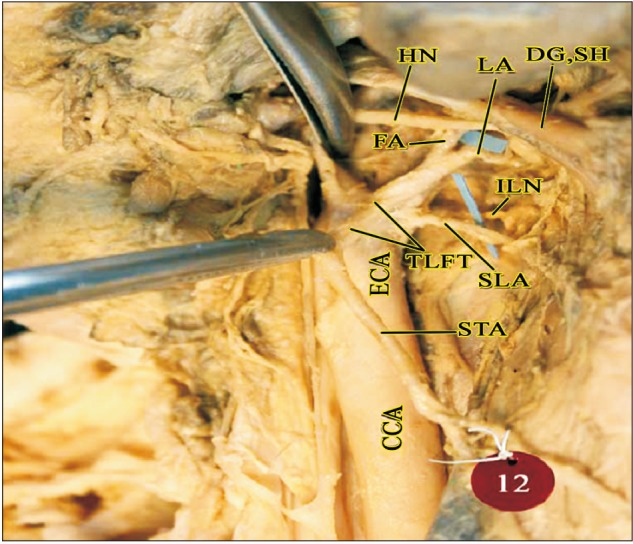
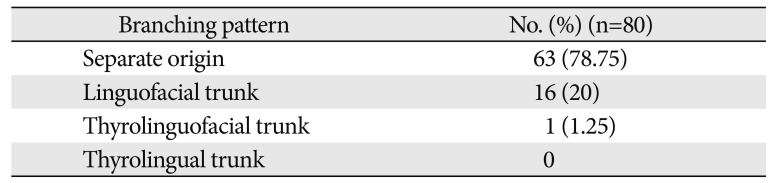
The anterior branches of the ECA include the STA, LA, and FA. Out of the 80 hemi-necks studied, separate origins for the anterior branches of the ECA were observed in 63 cases (78.75%). In the remaining 17 cases, formation of common trunks was observed. The linguofacial trunk was the commonest observed variation with the thyrolinguofacial trunk (TLFT) occurring only in a single case (Fig. 4). The TLFT was found to arise 6 mm above the carotid bifurcation and after a short length of 3 mm, divided into the STA and a common linguofacial trunk (Fig. 4).
Out of the 16 linguofacial trunks noted, the trunks were bilaterally present in 10 of 80 cases (12.5%) and in the remaining 6 of 80 cases (7.5%), unilateral occurrence was observed. No thyrolingual trunks were observed. The findings are summarized in Table 2.
Medial branches
The APA is the smallest branch of the ECA and arises from its medial surface near the origin. Normal branching pattern of the APA was observed in 78/80 cases (97.5%). An unusually high origin of the APA was observed in 1 case (1.25%) where the APA arose 20 mm above the carotid bifurcation from the posterolateral aspect of the ECA, opposite to the LA (Fig. 5). In addition, double ascending pharyngeal arteries were observed arising from the posteromedial aspect of ECA in 1 case (1.25%) (Fig. 6).
Posterior branches
No significant variations were observed in the branching pattern of the occipital and posterior auricular arteries.
Terminal branches
The ECA terminated at the level of the neck of mandible by dividing into superficial temporal and maxillary arteries in all the cases. No variations were noted.
Accessory branches
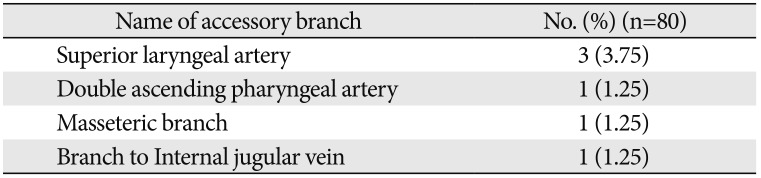
Accessory branches were found to arise from the ECA in 6 of 80 cases (7.5%) (Table 3).
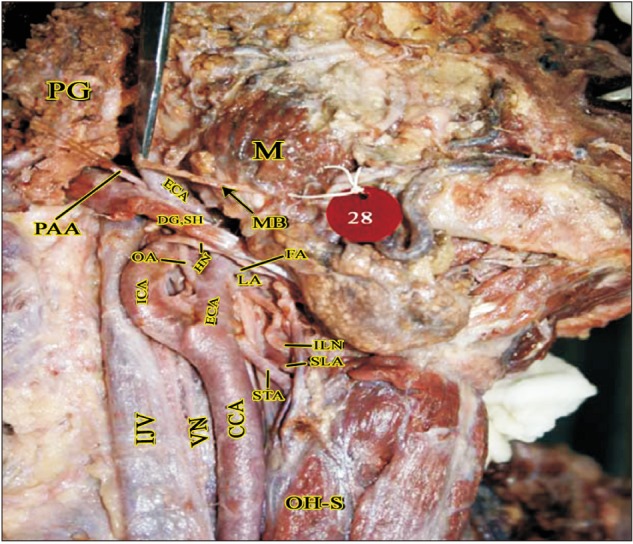
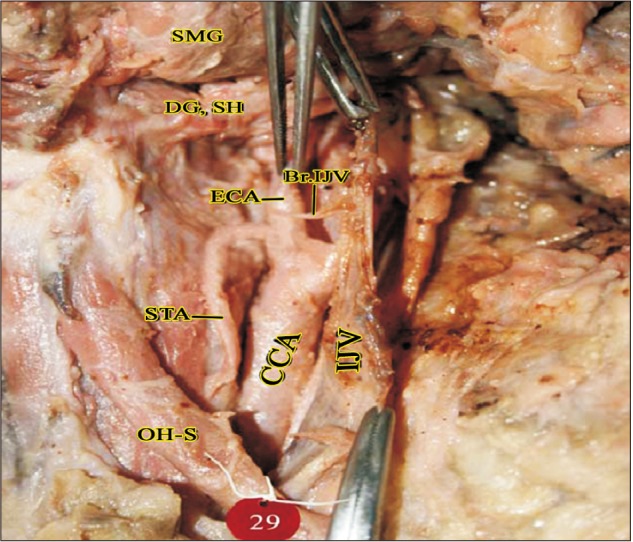
The muscular branch to the masseter muscle was seen arising from the anterior aspect of the ECA just above the PAA in the parotid region (Fig. 7). A slender branch to the internal jugular vein was seen arising from the anteromedial aspect of ECA 3 mm above the STA origin (Fig. 8). Superior laryngeal artery (SLA) was found arising directly from ECA in 3.75% cases (Fig. 9).
Discussion
Numerous variations in the external carotid vascular anatomy have been described in the available literature. The carotid bifurcation is an important anatomical and surgical landmark requiring special mention in the pathogenesis of carotid atheromatous disease and its consequent management by carotid stenting and endarterectomy [12]. A higher level carotid bifurcation may cause further distal extension of plaque making standard approaches inadequate for plaque removal and arteriotomy repair [13]. The level of the carotid bifurcation has been studied by various authors in the past. Higher levels of carotid bifurcation have been frequently reported in studies done by Lucev et al. [14], Ito et al. [15], Sanjeev et al. [16], Al-Rafiah et al. [17], and Mompeo and Bajo [18]. According to Al-Rafiah et al. [17] and Mompeo and Bajo [18], the commonest position of high carotid bifurcation was at the level of the hyoid bone in 25% and 36.85% cases respectively which correlates with our study. Lower levels of bifurcation have also been reported by the same authors with varying frequencies. Carotid bifurcations as low as intrathoracic bifurcations have also been reported in available literature [1920]. A low carotid bifurcation may be associated with Klippel-Feil anomaly [20] and may cause difficulties during surgeries like cervical discectomy [21]. With reference to previous similar studies (Table 4), it may be noted that a higher level bifurcation is more common and lower bifurcations are less frequent. This correlates well with the present study also where no low level bifurcations were found. At the same time, a high carotid bifurcation (CB) should caution surgeons regarding the close proximity of hypoglossal nerve and superior cervical ganglion as well as possible STA origin from the CB [2223]. The position of the CB depends on how low or high ECA originates from the third aortic arch [23].
It can thus be concluded that the level of the carotid bifurcation exhibits a great degree of anatomical variability and cautious ascertaining of its position is mandatory to avoid complications during angiographic and surgical interventions.
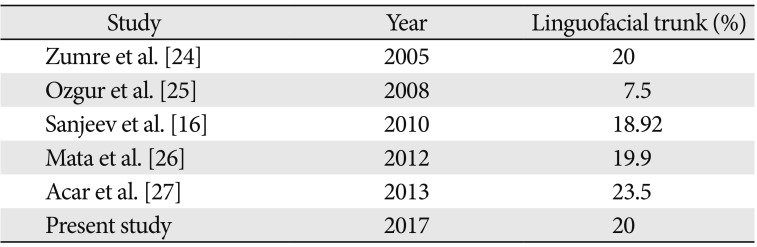
The occurrence of common trunks in the branching pattern of the ECA has frequently been described in the current literature. The linguofacial trunk, by far, appears to be the commonest variation with high incidence as per literature reports (Table 5). The linguofacial trunk was observed in 20% cases in the present study.
A unilateral TLFT was observed in a single case in our study (1.25%). This coincides with findings of previous studies where a TLFT is a relatively rare occurrence with the incidence reported to be 1.7% by Al-Rafiah et al. [17], 2.5% by Zumre et al. [24], and 0.3% by Vazquez et al. [28]. It is important to recognize these anatomical variations as the superior thyroid, facial and lingual arteries may be used as recipient vessels for microsurgical reconstruction in head and neck cancers [29].
Thyrolingual trunks have also been reported with a lesser incidence by Hayashi et al. [13] (1%), Ozgur et al. [25] (2.5%), and Acar et al. [27] (2%). However, no thyrolingual trunks were found in our study.
According to Baik et al. [30], common linguofacial trunks arising from the ECA may place the LA or FA in closer proximity to the tonsillar fossa, increasing the risk of iatrogenic vessel injury. The linguofacial trunk is also a common site of traumatic pseudoaneurysm after tonsillectomy [31].
Mata et al. [26] suggests that the embryology of the combined trunks would be in keeping with the angiogenesis theory, which suggests that confluence of the vessels and vessels with large diameter are more common in fetuses compared with adults as TLFTs are more common in fetuses and tend to disappear in adults. Iwai et al. [29] states that the TLFT represents the STA developing ectopically from the linguofacial trunk.
Knowledge of variations in the origin of the APA is vital for the exact identification of the neck vessels during surgery, to avoid a fatal mix-up with the ICA, as cited by Al-Rafiah et al. [17].
Hayashi et al. [13] observed the origin of APA from the ECA with relation to the origin of LA and found high origin above LA in 66% cases and below LA in 9% cases. We found a high origin of APA at the level of the LA in our study. Bergman et al. [32] states that the APA may be occasionally doubled or tripled. In the present study, an accessory APA with higher level of origin was observed in one case. Sanjeev et al. [16] observed accessory branches arising from the ECA in 13.5% cases as compared to 7.5% cases in the present study. When present, accessory branches of the ECA are often found to be the SLA as has been observed by the same authors previously [33]. The SLA arose from the ECA in 3.75% cases in the present study. This can be compared with the findings of Nayak et al. [34] where SLA arose from ECA in 5.4% cases and our previous study where SLA was found arising from ECA in 5% of the cases [33]. An accessory muscular branch supplying the masseter was seen in one case in this study. Masseteric branches from ECA have been observed by Marinho et al. [35] and Ariji et al. [36] in imaging studies. In addition, a slender branch to the internal jugular vein was seen arising from the anteromedial aspect of the ECA in the present study in one case. To the best of our knowledge, there are no previous reports of such a branch in the available literature. Standard textbooks [3738] describe the tunica adventitia of large arteries and veins as being supplied by their own vasa vasora which are derived from adjacent arteries.
The branches of the ECA are the key landmarks for adequate exposure and appropriate placement of cross-clamps to carry out successful removal of plaque and minimize postoperative complications in a bloodless surgical field [13]. Caution must be paid with ligature of blood vessels of the carotid triangle, because if these blood vessels are not distinguished, this may have catastrophic consequences in cerebral circulation or it can cause bleeding in the region of the ECA [39].
The branching pattern of the ECA in the neck shows considerable amount of variability and a clear anatomical understanding of the angioarchitecture will help to improve overall procedure outcome and prevent fatal complications. Prior angiographic assessment to ascertain the level of carotid bifurcation as well as the branching pattern of the carotid arterial system may prove valuable to avoid injury to vital structures such as hypoglossal nerve and minimise troublesome haemorrhage during surgical exploration of the head and neck region.
 XML Download
XML Download