

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
1. Background
Population aging is progressing rapidly in many countries around the world. In Korea, older people aged 65 or older were reported to account for 13.8% of the total population in 2017 and the proportion of older people is estimated to increase to 41% in 2060 in Korea [1]. In terms of the healthcare of older people in the community, the increase of frail older people is of equal or greater importance than the rapid rate of aging. It has been reported that frailty occurred in 15.3% of community-dwelling older people aged 70 or over, and the prevalence of frailty was 18.5% in older women and 8.3% in older men [2], and the perspective about the health of older people is shifting from age to weakness. Therefore, it is an important role of community nursing to provide the necessary preventive nursing care to prevent the occurrence of frailty in older people, ensure the early detection of frailty through periodic health assessment, and prevent the progression of frailty resulting in disease or disability through the integrated management of frailty [3].
Frailty is a condition in which an individual continues to be at a risk of injury for a long period or an individual's overall health status can be compromised [4]. It can occur in all age groups, but it is a major healthcare problem for older people because it is closely related to the aging process [5]. Considering the vulnerability of older people, even when there is no physiological functional decline or deficiency, if the social, emotional, and environmental support is reduced, frailty may occur and it should be approached by multidimensional assessments [6].
Frail older people have difficulty coping with even a small stressful situation, have limitations in performing daily living activities, have an increased risk of accidents such as falls, and experience frequent hospitalization [789]. This not only shortens the life span of older people, but also has a significant impact on the quality of life, and it also leads to the deterioration of the state of the healthcare finance due to the increased burden of medical expenses [7].
Although studies on frailty have been extensively conducted since the 1980s, the definition of frailty has been limited to some attributes depending on the researchers' point of view. Therefore, the measurement instruments have been generally confined to physical domains [5], and only some tools have dealt with psychological domains [1011], but there is a gradually increasing tendency to perceive frailty as a broad, multifaceted concept encompassing physical, psychological, and socioenvironmental factors [1213]. Since various attributes were not considered when measuring frailty, the prevalence of frailty were reported to be different in related studies [14]. The review and analysis of studies on frailty carried out so far give an insight into the past, present and future of the body of accumulated knowledge.
The existing research methods have limitations in analyzing and gaining an insight into the vast amount of research data accumulated so far on a subject. Text Network Analysis is a type of social network analysis [15] that quantitatively analyzes the structure, pattern, and characteristics of a network by modeling the relationships among individuals and groups as nodes and links. It analyzes a lot of accumulated research data in terms of structures, communication processes, relationships, and visualizes them, thereby providing a comprehensive view of a subject. Thus, it has recently been used in various sciences including nursing. Keywords are chosen by the researcher to represent the main topic and key concepts of the paper, and since they are used as small units to analyze the research papers, they can be a good means to investigate the research trends through text network analysis [16]. With respect to the studies using text network analysis in the field of nursing, Lee et al.[17] analyzed the research trends of the science of nursing using the papers published in the Journal of Korean Academy of Nursing, and Park et al.[18] presented research directions for researchers by analyzing the trends of research on hospice care through comparison between domestic and foreign studies. Research trends of studies on patient adherence has also been previously analyzed [19], and Kim and Jang [20] has presented an analysis of the historical trends of studies on frailty.
Geriatric frailty is a nursing problem that needs to be addressed by the early assessment of geriatric frailty and provision of holistic nursing interventions so that older people can maintain independent functions and improve their quality of life. Therefore, for the development of gerontological nursing practice, it is necessary to analyze researches related to frailty of older people to establish a theoretical basis and present the direction of future research. Therefore, this study aimed to investigate the key concepts of studies related to frailty through text network analysis and examine the relationships among the key concepts and the structure in order to understand the research trends and establish the knowledge structure.
2. Purpose
The purpose of this study was to identify core keywords and the sub-topic groups of studies on geriatric frailty by analyzing and clustering keywords based on the co-occurrence frequency and centrality using text network analysis of author keywords of studies on geriatric frailty carried out so far.
METHODS
1. Study Design
This study is a descriptive research to identify key concepts and investigate relationships among the concepts in domestic and foreign studies on geriatric frailty through an analysis of author keywords of research papers by the text network analysis technique.
2. Methods and Procedures
In this study, we analyzed author keywords of the research papers related to geriatric frailty published in the journals of medicine, the science of nursing, and health science from January 1981 to April 2016, and the keywords were extracted from the journals searched through WOS (Web of Science). The term frailty was first used in 1974, but it is not possible to search the abstracts and keywords of research papers published before 1981, so only studies published since 1981 were included in the study. By reviewing abstracts and keywords, we excluded papers of unrelated fields, such as papers about animal experiments, those of which the participants were children or those of which the research topic is not geriatric frailty.
The research procedures were largely composed of three stages, as shown in Figure 1.: 1) collection of research papers, 2) keyword extraction and matrix generation, and 3) text network analysis.
1) Collection of research papers
The key search term in English was “frail” or “frailty”, journal categories were limited to ‘geriatrics’ ‘geriatrics gerontology’, ‘general internal medicine’, ‘public environmental occupational medicine’, ‘nursing’, and ‘psychology’, the type of documents was limited to articles, and the language was limited to English. As a result, 10,367 documents were retrieved and a database was constructed. Based on the selection and exclusion criteria, we reviewed the titles and abstracts of the research papers and excluded irrelevant or repeatedly included papers. The papers about which we did not reach an agreement were reviewed by the third researcher, and 6,424 research papers were finally selected. The third researcher is a professor of the department of community health nursing who has performed several researches on the health and frailty of older people.
2) Extracting and cleaning keywords
Using the Bibexcel program, we extracted the author keywords of the collected documents and performed text analysis. The analysis of the relationship between keywords was performed using NetMiner ver.4.0. The Bibexcel program enables keyword analysis, co-citation analysis, and citation frequency analysis. Data conversion was performed by converting the matrix or network data in order to use the data in the bibliometric analysis program [21].
The extracted keywords were refined through the following procedure. The process of standardization is to remove synonyms and derivative words and exclude irrelevant additional expressions or words. When extracting keywords, we excluded general verbs, nouns not related to the main topic of this study, and general terms (special symbols, additional words, and words not directly influencing the research topic of this study) that are difficult to regard as key concepts of this study [22]. Regarding whether to include synonyms or related words such as ‘old’, ‘elderly’, and ‘aged’, one of the related words was designated as a representative word through the discussion among one nursing professor, one medical professor, and one doctoral student in medical school. The plural nouns were changed into singular forms and words with similar meanings were grouped together through the process of standardization. For example, ‘aged’, ‘age-old’, and ‘old’ were standardized into ‘aged’, and ‘frail’, ‘weak’, and ‘fragile’ were standardized into ‘frail’. The matrix between the keywords was constructed using the standardized keywords.
3) Analysis of co-occurrence frequencies
Using the Bibexcel program, high frequency keywords were extracted by analyzing the frequency of co-occurrence of keywords in the frailty network. Co-occurrence refers to the case where two keywords appear together in a research paper, and the top 30 keywords were selected by arranging the number of research papers in which the keywords appeared in the order of decreasing frequency.
4) Data processing
We performed pruning to find out the influential keywords among extracted keywords. Pruning removes nodes with a degree of connection below a specific value, and this process makes it easy to locate influential nodes and enables clear visualization. We performed node filtering by selecting only keywords with a degree of connection of 3 or more, eliminated the self-loops (diagonal) generated in the data conversion process, and simplified the network by excluding the relationships with a low co-occurrence frequency from analysis.
5) Analysis of the connection structure of the network and centrality analysis
The degree of connection between keywords, attributes, and strengths were quantitatively analyzed by converting the 2-mode network in the form of research paper-keyword into the 1-mode network in the form of keywordkeyword. The density, degree, centralization, and inclusiveness of the network, which are the representative indicators of the connection or bond among keywords, were examined. Density is defined as the ratio of the number of relationships actually formed to the total number of possible relationships, and centralization refers to the degree to which the relationships are concentrated on a few individuals. Inclusiveness means the number of nodes connected to each other in the network. Centrality analysis was conducted to find important nodes in the network. Centrality analysis is performed to find out which keyword among various keywords is located at the center, and centrality was divided into degree centrality, betweenness centrality, and closed centrality. The degree centrality indicates the degree of connection with other nodes, and it is increased as more nodes are connected. The betweenness centrality is measured mainly in terms of the role of a keyword as the intermediator and mediator in the entire network, and the closed centrality indicates that a keyword is located closest to the search term (frailty, frail). The keywords that are close to each other can be regarded as those that influence other keywords rapidly, and the closed centrality is the most important concept of centrality in co-occurrence word analysis [15]. In this study, keywords which were included in the top 30 keywords in terms of co-occurrence frequency and each type of centrality were designated as core keywords.
6) Cohesion analysis
Cluster analysis was performed to examine the structure of the network and investigate clustering. Cluster analysis can be used to identify the detailed internal structure of the network [23]. Cohesion analysis makes it possible to find out which keywords are studied together and thereby identify sub-research areas. A dendrogram can be used to identify keywords with similar role equivalence based on the similarity of keywords by equivalance analysis.
RESULTS
1. General Characteristics of Studies on Frailty
A total of 6,424 research papers on frailty were analyzed in this study, and the number of analyzed articles by period was 142 for the 1980s, 753 for the 1990s, 2,643 for the 2000s, and 2,886 for the 2010s, so the number of studies on frailty has considerably increased since 2000. The number of keywords by period was 62 for the 1980s, 361 for the 1990s, 997 for the 2000s, and 965 for the 2010s, so a total of 2,385 keywords were extracted.
2. Core Keywords of Studies on Frailty
The density of the frailty network was 0.16, the average degree of connection was 5.42, and the inclusiveness (the ratio of connected nodes to all nodes) was 91.5%. The keyword rankings were determined based on 1) high co-occurrence frequency, 2) degree centrality, 3) betweenness centrality, and 4) closed centrality of author keywords of research papers on frailty, and the top 30 keywords for each criterion were referred to as core keywords.
1) Keywords with high co-occurrence frequency
With respect to keywords with high co-occurrence frequency, the number of occurrence of the keywords was 147 for disability, 126 for nursing home, 116 for sarcopenia, 106 for exercise, and 88 for dementia in the order of occurrence frequency. As a result of classification of keywords according to the domains based on the subheadings of MeSH, the majority of keywords belonged to the healthcare and physical domains (Table 1).
2) Degree centrality
The degree centrality of the entire network was 0.23 on average and the centralization was 43.2%. The keyword with the highest level of degree centrality was ‘long term care’ (0.55), followed by ‘gait’ (0.42), ‘physical activity’ (0.42), ‘quality of life’ (0.42), and ‘physical performance’ (0.38) (Table 2).
3) Betweenness centrality
The betweenness centrality of the geriatric frailty network was 0.01 on average and the centralization was 10.6 %. The keyword with the highest level of betweenness centrality was ‘disability’ (0.12), followed by ‘frailty’ (0.10), ‘gait’ (0.09), ‘quality of life’ (0.09), and ‘long term care’ (0.09) (Table 2).
3. Groups of Sub-topics of Studies on Frailty
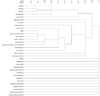
In order to investigate the sub-structure of the geriatric frailty network, cohesion analysis was conducted based on similarity. Thirteen subgroups with a high level of cohesion were identified and they were classified into the final seven groups excluding the groups with a single term. The names of the subgroups were selected by the researcher in consideration of the terms including the keywords with high centrality. As a result, the first group was named aging and frailty, the second, sarcopenia, the third, inflammation, the fourth, mortality, the fifth, frailty index, the sixth, older people, and the seventh, physical activity. The process by which core keywords are clustered according to cohesion is shown by a dendrogram (Figure 3).
The first group included ‘aged’, ‘aging’, ‘frail’, and ‘frail elderly’ and the second group included ‘sarcopenia’. The third group included ‘inflammation’, ‘interlukin-6’, and ‘lymphocyte count’, and the fourth group included ‘mortality’, ‘longevity’, and ‘survival’. The fifth group included ‘comprehensive geriatric assessment’, ‘geriatric assessment’, and ‘frailty index’, and the sixth group included ‘older people’ and ‘elderly’. The seventh group included ‘physical function’, ‘physical performance’, ‘exercise’, and ‘mobility’.
DISCUSSION
In this study, we analyzed the author keywords of studies on geriaric frailty carried out from 1981 to 2016 by applying text network analysis, and we intend to make a few suggestions about the direction of future studies related to geriatric frailty in the field of nursing based on the core keywords identified by the analysis. The average degree of connection of the geriatric frailty network was 5.4 times, and the density was as low as 0.16, but the level of inclusiveness was as high as 91.5%. These results are thought to show that the frailty network has a structure in which many keywords are clustered around several major keywords. In addition, cluster analysis showed that the frailty network is composed of seven subnetworks.
A total of 2,385 keywords were extracted from 6,424 research papers related to geriatric frailty. In this study, keywords with high co-occurrence frequency were ‘disability’, ‘nursing home’, ‘sarcopenia’, ‘exercise’, and ‘dementia’ in the decreasing order of frequency. This finding shows that many quantitative studies on them have been carried out. Because frailty is the concept at the boundary between health and disability, frail older people are more likely to develop severe conditions when exposed to stress and thus be at a stage of disability impeding daily activities, compared to healthy older people, and disability limiting daily activities is used as a criterion of admittance into nursing home facilities. This seems to be the reason for a high frequency of occurrence of the words ‘disability’ and ‘nursing home’ [724]. In addition, it seems that since sarcopenia, which causes frailty, is reported to reduce activities and functions of frail older people, and be closely associated with an increase of mortality rate, related studies have been actively conducted [2425]. In comparison with the results of Kim and Jang [20], which analyzed the top 15 keywords of studies on frailty with a high level of degree centrality and betweenness centrality according to the periods, it was found that the words of disability, sarcopenia, and dementia are keywords with a high level of degree centrality and betweenness centrality in studies conducted in the 2000s, and are keywords with a large direct and indirect influence. ‘Nursing home’ was a central keyword with high degree centrality in the studies of the 1980s, and ‘exercise’ was a keyword with high betweenness centrality in the studies of the 2010s [20], so they were consistently found to be influential keywords although there were differences according to the periods.
Among the top 30 keywords with the highest co-occurrence frequency, ‘nursing home’, ‘exercise’, ‘depression’, ‘geriatric assessment’, ‘quality of life’, ‘physical activity’, ‘inflammation’, ‘epidemiology’, ‘comprehensive geriatric assessment’, ‘comorbidity’, and ‘longevity’ were included in the top 30 keywords of all categories of centrality, i.e., degree centrality, betweenness centrality, and closed centrality, so they were found to be influential variables and core keywords in researches on frailty. On the other hand, ‘rehabilitation’, ‘screening’, ‘prevention’, and ‘accidental fall’ were included in the top 30 in terms of the frequency of occurrence but they were not included in the top 30 in terms of centrality, so they were found to be keywords with a low level of influence. Compared with the study results of Kim and Jang [20], ‘screening’ was found to be a keyword with high betweenness centrality in the studies of the 2010s, and ‘accidental fall’ was a keyword with high degree centrality and betweenness centrality in the research conducted in the 2000s. ‘Rehabilitation’ and ‘prevention’ have been studied extensively, but they have not been linked to various detailed concepts, and studies on them have been conducted independently and have not been in the range of core research. However, ‘prevention’ and ‘screening’ are important keywords in nursing in order to prevent frailty in older people, perform early detection of frailty through periodical assessments, and prevent the progression of frailty, and help the patient's recovery of health through appropriate interventions when frailty is detected. Therefore, they need to be studied in connection with various concepts related to geriatric frailty in the future.
With respect to ‘geriatric assessment’ and ‘comprehensive geriatric assessment’, which are keywords with a high frequency of occurrence and high centrality, they changed from ‘assessment’ and ‘evaluation’ in the 1980s to ‘geriatric assessment’ in the 1990s to ‘disability evaluation’ in the 2000s to ‘geriatric assessment’ and ‘comprehensive geriatric assessment’ in the 2010s. This result is consistent with the gradual transitional changes in the frailty assessment tools from earlier instruments which emphasized physical domains to the development and use of multidimensional instruments that include the psychological, social, and environmental domains [51324].
As for the keywords which showed high centrality although they were not among the top 30 in terms of the frequency of occurrence, the keywords with high degree centrality were gait, incidence, nutritional status, weight loss, reliability, biomarker, muscle strength, mobility, nutrition, nursing, and geriatric oncology. Gait, weight loss, muscle strength, and mobility are included in the evaluation criteria of frailty [46], and biomarker is a test to measure inflammatory changes, one of the pathophysiological changes of frailty. These facts are thought to explain the fact that the words were found to be closely connected to frailty. The result that biomarker and geriatric oncology have emerged as keywords with high degree centrality in the studies of frailty conducted in the 2010s [20] showed that they have recently been actively studied in connection with studies on frailty. The core keywords with a high level of betweenness centrality were ‘frailty’, ‘gait’, ‘mobility’, ‘incidence’, ‘sex difference’, ‘nutrition’, ‘biomarker’, ‘nutritional status’, ‘weight loss’, and ‘reliability’. Except for ‘frailty’ and ‘sex difference’, they also correspond to the keywords which are among the top 30 keywords in terms of degree centrality although they are not included in the top 30 in terms of the frequency of occurrence, and this result indicates that they not only have a lot of direct connections with other keywords but also play a role of making connections among keywords. The keywords with a high level of closed centrality were ‘cognition’, ‘mortality’, ‘older people’, ‘deficit accumulation’, ‘aged’, ‘elderly’, ‘mobility’, ‘aging’, ‘severity of illness index’, and ‘frail older people.’ In relation to geriatric frailty, ‘cognition’, ‘deficit accumulation’, ‘mobility’, and ‘severity of illness index’can be regarded as keywords that influence other keywords rapidly.
Cluster analysis is a method to group closely correlated keywords into subnetworks and the studies on geriatric frailty are classified into 7 subgroups of ‘aging’, ‘sarcopenia’, ‘inflammation’, ‘mortality’, ‘frailty index’, ‘older people’, and ‘physical activity’.
As described above, we investigated of central research topics of studies on frailty using the co-occurrence frequency and three centrality indicators, and the results of this study showed that the central topics consisted mostly of physiological variables except for ‘depression’ and ‘quality of life’. Frailty has been identified as a predictor variable for cognitive decline and depression in older women, and prevention and delay of frailty in older people have also been reported to be important in the prevention of cognitive impairment and depression [26]. In addition, it has been reported that research has shown that the prevention of depression leads to the reduction of frailty, so attention is being paid to the relationship between frailty and depression [27]. Especially in the old age, social support is reduced for various reasons such as the loss of family members and friends, retirement, and unemployment, leading to the exacerbation of frailty in terms of social and environmental aspects. Therefore, assessment of the status of the social support system, finances, the degree of social isolation, and degree of loneliness in older people is required [28]. In addition, with respect to environmental aspects, environmental hazards that can trigger or accelerate frailty need to be defined and evaluated on an ongoing basis [29]. Moreover, it is also necessary to take measures for older people considering the multi-faceted characteristics of frailty encompassing physical, mental, social, and environmental frailty from a comprehensive perspective, such as the improvement of the residential environment, improvement of transportation, strengthening of visiting nursing service, improvement of the volunteering service system, and development of cultural leisure activities.
Although it was not derived as a central topic, qualitative research is also an important topic. Since most of the studies have approached geriatric frailty in terms of observable, external aspects of the phenomenon, it is necessary to conduct qualitative research that presents a comprehensive understanding of older people's overall experiences of frailty in the future. The description of older people's experience of frailty will provide caregivers and health care professionals with a better understanding of frail older people [30].
As a result of classifying the keywords of researches on frailty using the MeSH indexes, it was found that studies have been centered on healthcare and physical domains, and the research in mental, social and environmental domains has been limitedly conducted. Since the Federal Council on Aging in the United States first defined frailty in 1983, the term frailty has been used to classify older people with physical disabilities, emotional impairments, or inadequate physical or social environments. However, in this study, the review and analysis of studies accumulated over the past forty years showed that only physical frailty and frailty from a medical perspective have been emphasized. Therefore, in the future, more attention needs to be paid to the frailty in mental, social, and environmental areas, which has recently been attracting attention.
CONCLUSION
With global population aging, interest in healthcare for older people is increasing in the medical field, and the integrated management of frailty, which occurs commonly in older people, is an important challenge in the community. In this study, we derived author keywords of studies related to geriatric frailty through text network analysis and classified the research topics into 7 subnetworks in order to present the direction of research required for systematic management of frailty. The derived core keywords and subnetworks showed that studies of geriatric frailty have been focused on frailty in terms of physical frailty and healthcare. These study results suggest that frailty should be defined in terms of mental, cognitive, social and environmental aspects as well as physical frailty in the future, and that management of geriatric frailty including management of frailty in these areas should be developed and applied in an integrative way.
Based on the results of this study, we make the following suggestions. First, through the qualitative research on geriatric frailty, it is necessary to understand various aspects of frailty experienced by older people. Secondly, there is a need to understand emerging research trends through comparative keyword analysis between the studies conducted in the countries that are interested in the management of geriatric frailty and make efforts to manage it systematically and domestic studies, and to explore the direction of the development of domestic research based on the results. Third, studies on definition and management of frailty in terms of mental, social, and environmental aspects should be actively carried out, and an integrated system for prevention and management of frailty including physical frailty should be established. Since this study only analyzed the researches contained in one database, there is a need for follow-up studies that encompass various databases in order to gain a more comprehensive understanding of research trends. In addition, in order to increase the validity of the knowledge structure derived through textual network analysis, it is necessary to develop or incorporate a theory or model that will provide a conceptual framework.




 XML Download
XML Download