

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Variant angina pectoris (VAP) was, firstly described by Prinzmetal et al.1 in 1959. Within decades, we have identified the clinical features of this disease, as well as the treatment. Clinically, we generally use oral calcium channel antagonists, which can effectively control the disease. The cause of VAP has not yet been clearly demonstrated, but many studies have shown that VAP causes vascular smooth muscle hyperresponsiveness, which leads to coronary artery spasm as the main pathological mechanism. Other factors include autonomic nervous system dysfunction, and endothelial or microvascular dysfunction.2 VAP often occurs in normal angiographic arteries, but it is also seen in mild and serious atherosclerotic stenosis.3 According to previous reports of patients with coronary spasm, coronary heart disease complicated by coronary spasm showed poor prognosis.45 Although plaque itself may induce spasm, it is difficult to prove, but it is known that coronary artery spasm itself can induce the rupture of a stable atherosclerotic plaque, resulting in coronary artery thrombosis and myocardial infarction.
Thirty years ago, Yasue et al.6 found that in patients with VAP the survival rate without myocardial infarction (MI) at 10 years was more than 81%, indicating that the conversion of VAP to acute MI is rare. We now report a case of a typical VAP developing into acute MI with concurrent percutaneous coronary intervention (PCI).
CASE REPORT
A 48-year-old woman was admitted to the emergency department of Chonnam National University Hospital for severe chest pain. She suffered from new onset effort angina 2 days before and her pain was aggravated 4 hours prior to presentation. It radiated to the left shoulder and had a squeezing nature. She had no specific cardiovascular risk factors except for hypertension. She underwent coronary angiography (CAG) and was diagnosed as VAP at her local hospital 2 years before. She was not an alcohol drinker. She developed chest pain around 5 p.m. associated with cold sweating. Twelve-lead electrocardiogram (ECG) showed sinus bradycardia and T wave inversion in the precordial leads (Fig. 1). Troponin-I was positive at 0.062 ng/mL (reference range 0–0.05 ng/mL). Transthoracic echocardiogram showed good left ventricular systolic function without regional wall motion abnormality. Therefore, she was supposed to receive medical treatment for non-ST elevation MI due to coronary vasospasm. However, she complained of continuous chest pain during the admission and follow-up CAG was performed. CAG revealed critical spasm in the proximal left anterior descending artery (LAD) and myocardial bridge in the middle LAD. After injection of intracoronary nitroglycerin, spasm in the proximal LAD was relieved (Fig. 2). Medications were adjusted to the optimal tolerated doses for vasospasm, such as diltiazem 90 mg, isosorbide dinitrate 40 mg, nitroglycerin 0.6 mg and she was discharged without further chest pain.
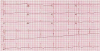 | Fig. 1Twelve-lead ECG showed bradycardia and T wave inversions in precordial lead.ECG; electrocardiogram.
|
 | Fig. 2(A, B) CAG revealed critical spasm in the proximal LAD, and (C, D) spasm was relieved after injection of intracoronary nitroglycerin.CAG; coronary angiography, LAD; left anterior descending artery.
|
One month later, she visited to the emergency department for recurrent chest pain. At admission the ECG showed no ST segment deviation, and T wave inversion seemed to be restored. The patient's symptom was relieved without any management, so she was about to be discharged after 4 hours of observation at the emergent department. She, however, complained of chest pain again, and the ECG showed ST elevation and tall T wave in the leads V2 to V6 (Fig. 3A). Nitroglycerin was applied immediately, and the chest pain subsided with normalized ST segment. The next day, however, her ECG showed deep T wave inversions in the precordial leads compared with the previous ECG (Fig. 3B) and the level of troponin-I was markedly elevated to 2.32 ng/mL. The creatine kinase-MB was elevated to 10.09 ng/mL (1–3.6 ng/mL) and high-sensitivity C-reactive protein was normal. Emergent CAG was performed, and it revealed near-total occlusion in the proximal LAD and the lesion was not fully dilated despite use of intracoronary nitroglycerin (Once 200 µg in the left coronary artery) (Fig. 4). With wiring down to the proximal LAD, predilation was done with 2.5×15 mm balloon at up to 6 atm. We performed intravascular ultrasound (IVUS) to evaluate characteristic of the lesion. The minimal lumen area (MLA) was 2.7 mm2 and mixed plaque burden was 82% with the distal and proximal diameters of 4.0 mm and 3.5 mm (Fig. 5). Therefore, balloon angioplasty was done in the proximal LAD with a 3.0×15 mm balloon, followed by stenting using a 3.5×20 mm bioabsorbable polymer everolimus-eluting stent (Fig. 6). The final CAG showed good distal flow with good stent apposition. Post-stenting IVUS showed that the minimal stent area was 8.4 mm2 with decreased plaque burden at the target lesion (Fig. 7). The quantitative coronary angiography (QCA) baseline reference diameter was 3.51 mm and diameter stenosis 100%. After PTCA, minimal lumen diameter was 1.05 mm and diameter stenosis 70%. Post-stent minimal lumen diameter was 3.52 mm and diameter stenosis 0%. Afterwards, she did not complain further chest pain and was discharged with aspirin, clopidogrel, diltiazem, isosorbide dinitrate, and statin.
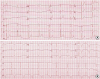 | Fig. 3(A) One month later, ECG showed ST elevation and tall T waves in V2 to V6. (B) The next day, the ECG showed deep T wave inversions in the precordial leads.ECG; electrocardiogram.
|
 | Fig. 4(A, B) CAG revealed near-total occlusion in the proximal LAD. (C) There was nosignificant stenosis in the right coronary artery and (D) the lesion was not relieved despite use of intracoronary nitroglycerin.CAG; coronary angiography, LAD; left anterior descending artery.
|
 | Fig. 5(A) IVUS showed that the MLA was 2.7 mm2 and mixed PB was 82% in the target lesion, (B) the distal diameter was 4.0 mm and (C) the proximal diameter was 3.5 mm.IVUS; intravascular ultrasound, MLA; minimal lumen area, PB; plaque burden.
|


DISCUSSION
Since the 1990s, atherosclerotic lesions have been detected in patients with focal vasospasm in coronary arteries,7 and it is believed that the presence of atherosclerotic lesions is related to the occurrence of vasospasm.8 Although the prognosis of cardiovascular events in patients with coronary artery disease (CAD) is more severe than that of CAD, the presence of organic coronary artery stenosis is an important risk factor for cardiovascular events in patients with VAP.9
Patients with VAP generally have symptoms at rest, especially at midnight, or in the early morning, which, mostly resolve themselves. Chest pain is often accompanied by high blood pressure, dizziness, nausea; and/or vomiting, and some patients may show low blood pressure and fainting as the primary presentation.
ECG often manifests ST segment elevation at the onset of VAP, ST segment normalizes without pathological Q waves after relieving vasospasm.1 In our case on the ECG during the second attack, T waves in V2–V6 were deeply inverted and troponin-I increased. It strongly suggested VAP complicated with acute MI. Therefore, in order to confirm the diagnosis and ensure the treatment effect, CAG were performed.
According to the guidelines for VAP, IVUS is an important tool in the diagnosis of VAP.8 Its main function is to elucidate the etiology and pathology according to its morphological characteristics.8 IVUS can detect thrombosis and plaque burden10 as well as plaque volume11 and thin-cap fibroatheroma.12 We performed IVUS to understand more about the characteristics of the lesion. IVUS has to be considered for patient with vasospasm in the proximal or left main coronary artery which can be life-threatening by spasm. In our case, IVUS showed a large amount of plaque (plaque burden 82%, MLA 2.7 mm2) in the target lesion, which was successfully treated by stenting (post-PCI MSA 8.4 mm2), demonstrating IVUS is a useful tool to assess coronary lesions and to better treat the lesions. While IVUS resolution is limited, it can accurately determine the size of the blood vessel, artery remodeling and the length and size of the stent.13 Thus, if the plaque burden is severe on IVUS assessment in patients with recurrent VAP, treatment with stent implantation rather than medication should be considered.
Medical treatment after PCI in patients with VAP should include calcium channel antagonists, plus dual antiplatelet therapy with aspirin and clopidogrel, and statin.14 In addition isosorbide dinitrate can relieve chest pain. Beta-blockers are not permitted because they cause non-opposed alpha-adrenergic stimulation and increased vasoconstriction.15 VAP is a special type of unstable angina with coronary artery spasm as the main pathogenesis. In the clinical coronary spasm, whether it be from pure spasm, progression of atherosclerosis or mixed angina, all patients will have chest pain, therefore, it is difficult to distinguish between these entities. The diagnosis also depends on CAG judgment. However, there are differences between the three treatments after diagnosis. The coronary spasm requires calcium channel antagonists to prevent vasospasm. Progression of atherosclerosis and mixed angina needed to be treated with medication such as anti-platelet agents and statins to stabilize vulnerable plaques. In case of mixed angina, calcium channel antagonists should also be included.
VAP is a CAD which can be well controlled with medical treatment. However, focal fixed lesions with high plaque burden at the site of vasospasm might be difficult to control by anti-spasmatic medication alone. Therefore, intravascular imaging, especially IVUS, should be considered for patients with focal lesions in the proximal LAD or left main coronary artery, in whom severe vasospasm may have life-threatening consequences.
In conclusion, this case described a unique example of worsening of the previous mild atheromatous plaque lesion in a month, which led to near-total occlusion in a patient with VAP. The previous studies showed that the coronary spasm occurs at the site of preexisting atherosclerosis.16 This suggests that potential arterial dysfunction may be a risk factor for VAP, which is very similar to the characteristics of the case we reported. We must exercise caution in patients with VAP who complain of recurrent chest pain, because there is a possibility of plaque progression or rupture provoking acute coronary syndrome.
 XML Download
XML Download