

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Familial hypercholesterolemia (FH) is typically associated with single gene mutation that is inherited by autosomal dominant manner. Due to high cardiovascular risk, aggressive discovery, diagnosis, and treatment of FH are critical. Although FH is being increasingly spotlighted, we do not have sufficient data on Korean patients with FH. Here, we present the content of symposium of the Education Committee, Korean Society of Lipid and Atherosclerosis held in May 2018: 1) epidemiology, clinical diagnosis, Korean FH data, and regulation in Korea; 2) genes associated with FH, sequencing process in suspicious proband, cascade screening, and difficulty in genetic diagnosis in FH; 3) the importance of lipid-lowering therapy in FH, conventional and novel therapeutics for FH; 4) diagnosis of FH in children and adolescence, screening, and treatment of FH in children and adolescence; 5) history of FH studies in Korea, the structure and current status of FH registry of Korean Society of Lipid and Atherosclerosis; and 6) difficulty in diagnosis of heterozygous and homozygous FH, drug intolerance and achievement of treatment target. Discussion between speakers and panels were also added. We hope that this article is helpful for understanding FH and future studies performed in Korea.
Figures and Tables
Fig. 1
Receiver operating characteristic curves for total cholesterol and LDL-C and the presence of putative pathogenic variant carreirs. The best threshold values identified with the sum of sensitivity and specificity are indicated (from reference Shin et al.4 with permission).
LDL-C, low-density lipoprotein-cholesterol; TC, total cholesterol; AUC, area under the curve.


Fig. 3
A flow example of screening and interpretation of variants potentially causing FH.
FH, familial hypercholesterolemia; NGS, next-generation sequencing; SNV, single nucleotide variant; CNV, copy number variation.

Fig. 4
LDL-C burden in individual with or without FH as a function of the age of initiation of statin therapy (from Nordestgaard et al.7 Permission waived).
LDL-C, low-density lipoprotein-cholesterol; FH, familial hypercholesterolemia; hoFH, homozygous familial hypercholesterolemia; heFH, heterozygous familial hypercholesterolemia; HDL-C, high-density lipoprotein-cholesterol; CHD, coronary heart disease; TG, triglyceride.
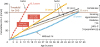
Table 1
Four clinical diagnostic criteria of FH

Table 2
Classification of variants' pathogenicity by the ACMG recommendation

Table 3
Studies of PCSK9 inhibitors in patients with FH

| Variables | TESLA part B | REGN727/SAR236553 | RUTHERFORD |
|---|---|---|---|
| Agent | Evolocumab | Alirocumab | Evolocumab |
| Phase | 3 | 2 | 2 |
| Study subjects & number | hoFH, 50 | heFH, 77 | heFH, 168 |
| Major findings | LDL-C reduction by 31% | Dose dependent LDL-C reduction by 29%–68%, compared to 11% reduction with placebo | Dose dependent LDL-C reduction by 43%–55%, compared to 3% increase with placebo |
| References | Raal et al.11 | Stein et al.12 | Raal et al.13 |
Table 4
Diagnostic criteria of FH in children and adolescence

| Variables | Europe | Simon Broome | US | MEDPED |
|---|---|---|---|---|
| LDL-C | ≥190 mg/dL after 3M of diet intervention | ≥155 mg/dL plus physical findings or family history | ≥160 mg/dL or non-HDL-C ≥190 mg/dL | ≥200 mg/dL in general population |
| ≥160 mg/dL plus family history ≥130 mg/dL & parent has genetic Dx of FH | ≥155 mg/dL with family history | |||
| Physical findings | Tendon xanthoma | |||
| Family history | Premature CHD and/or high cholesterol | Xanthoma and/or myocardial infarction or high cholesterol | FH | |
| Genetic | Detection of FH-causing mutation is gold standard | FH-causing mutation | ||
| Others | LDL-C should be measured at least ≥2 times/3 months | |||
| Secondary causes should be ruled out | ||||
| References | Wiegman et al.14 and Stock.15 | Daniels et al.16 |
Table 5
Treatment of hypercholesterolemia in children and adolescence

Table 6
Inclusion criteria for Korean Society of Lipid and Atherosclerosis FH registry (2015)

Table 7
Clinical characteristics of enrolled probands

Table 8
Cases of FH diagnosed with three different diagnostic criteria

Table 9
European Atherosclerosis Society diagnostic criteria for hoFH (2014)

Table 10
A case of FH patients with difficulty for achieving treatment target

References
1. Austin MA, Hutter CM, Zimmern RL, Humphries SE. Genetic causes of monogenic heterozygous familial hypercholesterolemia: a HuGE prevalence review. Am J Epidemiol. 2004; 160:407–420.

2. Hovingh GK, Davidson MH, Kastelein JJ, O'Connor AM. Diagnosis and treatment of familial hypercholesterolaemia. Eur Heart J. 2013; 34:962–971.
3. de Ferranti SD, Rodday AM, Mendelson MM, Wong JB, Leslie LK, Sheldrick RC. Prevalence of familial hypercholesterolemia in the 1999 to 2012 United States National Health and Nutrition Examination Surveys (NHANES). Circulation. 2016; 133:1067–1072.
4. Shin DG, Han SM, Kim DI, Rhee MY, Lee BK, Ahn YK, et al. Clinical features of familial hypercholesterolemia in Korea: predictors of pathogenic mutations and coronary artery disease - a study supported by the Korean Society of Lipidology and Atherosclerosis. Atherosclerosis. 2015; 243:53–58.
5. Han SM, Hwang B, Park TG, Kim DI, Rhee MY, Lee BK, et al. Genetic testing of Korean familial hypercholesterolemia using whole-exome sequencing. PLoS One. 2015; 10:e0126706.
6. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015; 17:405–424.
7. Nordestgaard BG, Chapman MJ, Humphries SE, Ginsberg HN, Masana L, Descamps OS, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013; 34:3478–3490.
8. Raal FJ, Pilcher GJ, Panz VR, van Deventer HE, Brice BC, Blom DJ, et al. Reduction in mortality in subjects with homozygous familial hypercholesterolemia associated with advances in lipid-lowering therapy. Circulation. 2011; 124:2202–2207.
9. Thompson GR, Blom DJ, Marais AD, Seed M, Pilcher GJ, Raal FJ. Survival in homozygous familial hypercholesterolaemia is determined by the on-treatment level of serum cholesterol. Eur Heart J. 2018; 39:1162–1168.
10. Oh J, Lee CJ, Kim DI, Rhee MY, Lee BK, Ahn Y, et al. Target achievement with maximal statin-based lipid-lowering therapy in Korean patients with familial hypercholesterolemia: a study supported by the Korean Society of Lipid and Atherosclerosis. Clin Cardiol. 2017; 40:1291–1296.
11. Raal FJ, Honarpour N, Blom DJ, Hovingh GK, Xu F, Scott R, et al. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolaemia (TESLA Part B): a randomised, double-blind, placebo-controlled trial. Lancet. 2015; 385:341–350.
12. Stein EA, Gipe D, Bergeron J, Gaudet D, Weiss R, Dufour R, et al. Effect of a monoclonal antibody to PCSK9, REGN727/SAR236553, to reduce low-density lipoprotein cholesterol in patients with heterozygous familial hypercholesterolaemia on stable statin dose with or without ezetimibe therapy: a phase 2 randomised controlled trial. Lancet. 2012; 380:29–36.
13. Raal F, Scott R, Somaratne R, Bridges I, Li G, Wasserman SM, et al. Low-density lipoprotein cholesterol-lowering effects of AMG 145, a monoclonal antibody to proprotein convertase subtilisin/kexin type 9 serine protease in patients with heterozygous familial hypercholesterolemia: the Reduction of LDL-C with PCSK9 Inhibition in Heterozygous Familial Hypercholesterolemia Disorder (RUTHERFORD) randomized trial. Circulation. 2012; 126:2408–2417.
14. Wiegman A, Gidding SS, Watts GF, Chapman MJ, Ginsberg HN, Cuchel M, et al. Familial hypercholesterolaemia in children and adolescents: gaining decades of life by optimizing detection and treatment. Eur Heart J. 2015; 36:2425–2437.
15. Stock J. Landmark position paper on paediatric familial hypercholesterolaemia from the EAS Consensus Panel. Atherosclerosis. 2015; 242:277–280.
16. Daniels SR, Gidding SS, de Ferranti SD. National Lipid Association Expert Panel on Familial Hypercholesterolemia. Pediatric aspects of familial hypercholesterolemias: recommendations from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipidol. 2011; 5:S30–S37.
 XML Download
XML Download