

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Low-density lipoprotein cholesterol (LDL-C) is one of the most well-established risk factors for cardiovascular disease (CVD). Previous studies have shown a log-linear association per unit change in LDL-C and the risk of CVD regardless of study design (e.g., prospective cohort studies, randomized controlled trials, or Mendelian randomization studies).1 Although statins reduce LDL-C by 30%–50% and subsequently decrease the risk of cardiovascular (CV) events, a substantial CVD risk remains.2 In addition, CVD is still the leading cause of death worldwide, accounting for nearly 30% of all mortality.3 Therefore, efforts to further reduce the risk of CV events have continued.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor is one of the recently developed drugs, expected to reduce the risk of CVD by additional LDL-C reduction. The PCSK9 gene was first discovered in 2003 and, in 2006, it was found that this mutation was associated with reduced LDL-C levels as well as a lower incidence of CVD.45 Under normal conditions, PCSK9 binds to LDL receptor and, thus, promotes the lysosomal degradation of LDL receptor. This process inhibits the recycling of LDL receptor, reduces LDL receptor expression on hepatocyte surface, and finally decreases uptake of LDL-C from the circulation.6 The mechanism of the PCSK9 inhibitor is to reduce circulating PCSK9 levels, thereby increasing hepatic LDL receptor expression and lowering circulating LDL-C levels. As statin inhibits cholesterol synthesis in the liver, combination therapy of PCSK9 inhibitor and statin may have a synergy effect on reducing LDL-C throughout different mechanisms.7 PCSK9 inhibitor is a good example of a translational research with only 12 years from discovery of gene to approval of drugs.
In 2015, the USA Food and Drug Administration (FDA) approved PCSK9 inhibitors, evolocumab and alirocumab, to be used as an adjunct to diet and maximally tolerated statin therapy for treatment: 1) in patients with clinical atherosclerotic CVD who have not reached LDL-C goals; and 2) in patients with heterozygous familial hypercholesterolemia. Evolocumab was also indicated as an adjunct to diet and other LDL-lowering therapies (e.g., statins, ezetimibe, LDL apheresis) in patients with homozygous familial hypercholesterolemia who require additional lowering of LDL-C.89 In the same year, the European Medicines Agency (EMA) approved the use of PCSK9 inhibitors, evolocumab and alirocumab: 1) in patients with primary hypercholesterolemia or mixed dyslipidemia, as an adjunct to diet: (i) in combination with a statin and/or other lipid-lowering therapies in those who have not reached LDL-C goals with maximum tolerated dose of a statin, or (ii) alone or in combination with other lipid-lowering therapies in those who are statin-intolerant, or for whom a statin is contraindicated; and 2) in patients aged 12 years or over with homozygous familial hypercholesterolemia in combination with other lipid-lowering therapies.1011
In several clinical trials, PCSK9 has been shown to significantly reduce LDL-C by 50%–60% compared with placebo.121314 Furthermore, in the Global Assessment of Plaque Regression With a PCSK9 Antibody as Measured by Intravascular Ultrasound (GLAGOV) trial, evolocumab showed plaque regression as well as greater reduction in atheroma volume, compared with placebo.13 In the Open-Label Study of Long-term Evaluation Against LDL-C (OSLER) randomized trial, evolocumab demonstrated sustained reduction in LDL-C (>50%) up to 4 years and 53% decrease in cardiac events at 1 year.1516 In consistent with the OSLER results, the Long-term Safety and Tolerability of Alirocumab in High Cardiovascular Risk Patients with Hypercholesterolemia Not Adequately Controlled with Their Lipid Modifying Therapy (ODYSSEY LONG TERM) trial reported that alirocumab reduced LDL-C by 62% and major adverse CV events by 48% in high-risk patients.17 Recently, 3 major outcome trials to examine the impact of PCSK9 inhibitors on CV events have been reported.141819 This review summarizes the 3 CV outcome trials with PCSK9 inhibitors and discuss their clinical implications.
FOURIER TRIAL (EVOLOCUMAB)
The first completed trial that investigate the effects of PCSK9 inhibitor on CV outcomes is the Further cardiovascular OUtcomes Research with PCSK9 Inhibition in subjects with Elevated Risk (FOURIER) trial with evolocumab, a fully human monoclonal antibody to PCSK9.14 FOURIER was a randomized, double-blind, placebo-controlled trial that enrolled patients aged 40–85 years old with 1) atherosclerotic CVD: myocardial infarction (MI), nonhemorrhagic stroke, or symptomatic peripheral artery disease (PAD) and 2) LDL-C level ≥70 mg/dL or non-high-density lipoprotein cholesterol (HDL-C) ≥100 mg/dL while taking an optimized lipid-lowering therapy with statin (Table 1). A total of 27,564 patients were randomly assigned to receive subcutaneous injections of evolocumab (either 140 mg every 2 weeks or 420 mg monthly) or placebo.20 As the LDL-C lowering effects is equivalent between the 2 regimens, patients were allowed to choose the dosing frequency and to switch every 12 weeks. However, dose titration was not permitted. The primary efficacy endpoint was the composite of CV death, MI, stroke, hospitalization for unstable angina (UA), or coronary revascularization. The key secondary efficacy endpoint was the composite of CV death, MI, or stroke.20
Table 1
Comparison of study design, populations, and CV outcomes of PCSK9 inhibitors

CV; cardiovascular, PCSK9; proprotein convertase subtilisin/kexin type 9, MI; myocardial infarction, PAD; peripheral artery disease, LDL-C; low-density lipoprotein cholesterol, HDL-C; high-density lipoprotein cholesterol, UA; unstable angina, Q2W; every 2 weeks, QM; every month, SC; subcutaneously, CHD; coronary heart disease.
*Death resulting from an acute MI, heart failure, stroke, CV procedures, CV hemorrhage, other CV causes and sudden cardiac death; †Any death with a clear relationship to underlying CHD (death secondary to acute MI, sudden death, heart failure, etc.).
The mean age of participants was 62.5 years, and 75.4% of them were men. Patients with prior MI, non-hemorrhagic stroke, and symptomatic PAD were 81.1%, 19.4%, and 13.2%, respectively.14 At baseline, 80.1% of the patients had hypertension, 36.6% had diabetes mellitus, and 69.3% were taking high-intensity statin (Table 2). Baseline median LDL-C level was 92 mg/dL both in the evolocumab and placebo groups. At 12 months, 87% of patients had LDL-C level of 70 mg/dL or lower and 42% had LDL-C level of 25 mg/dL or lower. In the evolocumab group, median LDL-C level at 12 months was 30 mg/dL (interquartile range, 19–46 mg/dL), which seemed to remain relatively constant until the end of the trial. At 42 months, as compared with placebo, evolocumab reduced LDL-C levels by 54% (mean absolute reduction of 50 mg/dL; p<0.001).
Table 2
Comparison of baseline characteristics among CV outcome trials with PCSK9 inhibitor
Primary and secondary endpoints were significantly reduced in the evolocumab group, compared with placebo. During median follow-up of 2.2 years, the primary endpoint occurred in 1,344 patients (9.8%) in the evolocumab group and 1,563 patients (11.3%) in the placebo group: hazard ratio (HR) of 0.85 (95% confidence interval [CI], 0.79–0.92; p<0.001). The key secondary endpoint occurred in 816 patients (5.9%) in the evolocumab group and 1,013 patients (7.4%) in the placebo group: HR of 0.80 (95% CI, 0.73–0.88; p<0.001). For individual outcomes, evolocumab treatment significantly reduced the risk of MI, stroke, and coronary revascularization. However, there was no observed effect of evolocumab on either CV death or all-cause mortality. Relative risk reductions in primary and secondary endpoints were 15%–20% and absolute risk reduction (ARR) was 1.5% for both endpoints. This suggests that the number of patients who need to be treated to prevent one additional event (number needed to treat; NNT) is about 66. The benefits of evolocumab regarding primary and secondary efficacy endpoints were consistent across subgroups by age, sex, type of atherosclerotic CVD, baseline LDL-C levels, and intensity of statin therapy.1421 Of note, the magnitude of the risk reduction in the primary endpoint tended to increase over time, from a HR of 0.88 (95% CI, 0.80–0.97) in the first year to a HR of 0.81 (95% CI, 0.73–0.89) beyond the first year.
In a prespecified secondary analysis with 25,982 patients (94% of total patients), 10% of them had LDL-C levels <19 mg/dL and 2% had LDL-C levels <10 mg/dL at 4 weeks. Major CV events in these patients with very low LDL-C levels progressively decreased, showing a monotonic relationship between achieved LDL-C levels and CV outcomes, even with LDL-C levels <8 mg/dL.22 Several other post hoc analyses of FOURIER trial have been reported.23242526 Overall, evolocumab showed greater risk reduction in patients with additional risk factors as they have higher risk for CVD. Evolocumab significantly reduced primary endpoint both in patients with and without PAD: HR of 0.79 (95% CI, 0.66–0.94; p=0.0098) in patients with PAD; HR of 0.86 (95% CI, 0.80–0.93; p=0.0003) in patients without PAD; Pinteraction=0.40. However, ARR for primary endpoint was greater in patients with PAD than those without PAD (3.5% vs. 1.6%). Interestingly, evolocumab also significantly reduced the risk of acute limb ischemia, major amputation, or urgent peripheral revascularization for ischemia: HR of 0.58 (95% CI, 0.38–0.88; p=0.0093).23 Similarly, evolocumab significantly reduced CV risk in patients with and without diabetes, but greater ARR in patients with diabetes compared with those without diabetes (2.7% vs. 1.6%).24 Another analyses in high-risk subgroup with recent MI (<2 years), multiple prior MIs (≥2), and residual multivessel coronary artery disease also demonstrated greater ARR than that in low-risk group (3.4% vs. 0.8%, 3.7% vs. 1.3%, and 3.6% vs. 1.2%, respectively).25 According to high-sensitivity C-reactive protein (hsCRP) strata (<1, 1–3, and >3 mg/dL), ARR for primary endpoint tended to increase with hsCRP levels (1.6%, 1.8%, and 2.6%, respectively).26
Regarding safety, general adverse events as well as serious adverse events were not different between evolocumab and placebo groups except injection-site reactions (2.1% vs. 1.6%).14 Among patients without diabetes at the start of the trial (n=16,676), the prevalence of new-onset diabetes was similar between evolocumab and placebo groups (8.1% vs. 7.7%): HR of 1.05 (95% CI, 0.94–1.17). Neither serious adverse events nor adverse events occurred in patients achieving very low LDL-C levels.22 The binding antibodies to evolocumab was developed in 43 patients (0.3%) while neutralizing antibodies were not developed in the evolocumab groups.19
In summary of FOURIER trial including post hoc analyses, evolocumab effectively decreased LDL-C level more than 50% at 48 months when added on statin therapy. In patient with stable atherosclerotic CVD, evolocumab reduced the risk of primary efficacy endpoint by 15% (ARR, 2.0%) and composite of CV death, MI, and stroke by 20% (ARR, 2.0%).14 These results were similar in those with low LDL-C level (<70 mg/dL) or maximal-potency statin. Greater risk reduction was derived in subgroups at high risk for major vascular events: PAD (ARR for primary endpoint, 3.7%); diabetes (2.7%); MI within prior 2 years (3.4%); ≥2 prior MI (3.7%); residual multi-vessel disease (3.6%); and higher baseline hsCRP (2.6%).23242526 Based on the results of recent clinical trials, in December 2017, the USA FDA has revised the indications for evolocumab, as follows: 1) to reduce the risk of MI, stroke, and coronary revascularization in adults with established CVD; 2) as an adjunct to diet, alone or in combination with other lipid-lowering therapies (e.g., statins, ezetimibe), for treatment of adults with primary hyperlipidemia (including heterozygous familial hypercholesterolemia) to reduce LDL-C; and 3) as an adjunct to diet and other LDL-lowering therapies (e.g., statins, ezetimibe, LDL apheresis) in patients with homozygous familial hypercholesterolemia who require additional lowering of LDL-C.27 However, there was no observed effect of further reductions in LDL-C levels by evolocumab on CV death or all-cause mortality. During the trial, evolocumab treatment was generally safe and well-tolerated.
ODYSSEY OUTCOMES TRIAL (ALIROCUMAB)
The Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab (ODYSSEY Outcomes) trial was completed in January 2018.28 As the study results have not been published yet, this part is mainly based on the results presented at the 67th Annual Scientific Session of American College of Cardiology in Mar 2018.18 The ODYSSEY OUTCOMES trial was a randomized, double-blind, placebo-controlled trial that enrolled patients aged 40 years or older with 1) recent acute coronary syndrome (acute MI or UA) event within the preceding 1–12 months and 2) LDL-C level ≥70 mg/dL, non-HDL-C ≥100 mg/dL, or apolipoprotein B ≥80 mg/dL while taking a high-intensity or maximum tolerated dose of statin (Table 1). A total of 18,924 patients were randomly assigned to receive subcutaneous injections of alirocumab (either 75 or 150 mg every 2 weeks) or placebo.29 In the ODYSSEY Outcomes trial, dose of alirocumab was adjusted or changed to placebo in blinded fashion to achieve LDL-C level of 15–50 mg/dL. The primary efficacy endpoint was the composite of coronary heart disease (CHD) death, non-fatal MI, ischemic stroke, or hospitalization for UA. The main secondary endpoints were as followings in hierarchical order: 1) major CHD event (CHD death or non-fatal MI), hospitalization for UA, or ischemia-driven coronary revascularization procedures; 2) major CHD event; 3) any CV event (any CV death, any non-fatal CHD event, or non-fatal ischemic stroke); 4) all-cause mortality, non-fatal MI, or non-fatal ischemic stroke; and 5) all-cause mortality. Other secondary endpoint included CHD death and hospitalization for congestive heart failure.29
The mean age of participants was 58.6 years, and 74.8% of them were men. Patients with non-ST elevation MI, ST elevation MI, and UA were 48.5%, 34.5%, and 16.8%, respectively.18 Median time from index acute coronary syndrome to randomization was 2.6 months. At baseline, 64.7% of the patients had hypertension, 28.8% had diabetes mellitus, and 88.6% were taking high-intensity statin (Table 2). Baseline median LDL-C level was 87 mg/dL both in the alirocumab and placebo groups. As compared with placebo group, reduction in LDL-C levels in the alirocumab group slightly decreased over time from 56 mg/dL (64%) at 4 months to 48 mg/dL (55%) at 48 months. This may be attributed to study design of targeting LDL-C level of 25–50 mg/dL. At 48 months, mean LDL-C level in the alirocumab group was 53 mg/dL.
Compare to placebo, alirocumab significantly reduced the risk of both primary and secondary endpoints. During median follow-up of 2.8 years, the primary endpoint occurred in 903 patients (9.5%) in the alirocumab group and 1,052 patients (11.1%) in the placebo group: HR of 0.85 (95% CI, 0.78–0.93; p=0.0003).18 Primary efficacy endpoint was similar across subgroups according to age, sex, region, time from index event to randomization, or baseline LDL-C levels. The composite of all-cause mortality, non-fatal MI, or non-fatal ischemic stroke occurred in 973 patients (10.3%) in the alirocumab group and 1,126 patients (11.6%) in the placebo group; HR of 0.86 (95% CI, 0.79–0.93; p=0.0003). Although evolocumab treatment did not have a benefit on CV or all-cause mortality, alirocumab significantly decreased all-cause mortality compared with placebo (3.5% vs. 4.1%); HR of 0.85 (95% CI, 0.73–0.98; p=0.026). ARR in primary endpoint and all-cause mortality with alirocumab treatment were 1.6% and 0.6%, respectively. This suggests that NNT for primary endpoint and all-cause mortality are around 63 and 166, respectively.
In post hoc analysis of the ODYSSEY Outcomes trial, the greatest benefit was observed in patients with baseline LDL-C ≥100 mg/dL: ARR for primary endpoint of 3.4% (HR, 0.76; 95% CI, 0.65–0.87); CHD death of 1.0% (HR, 0.72; 95% CI, 0.53–0.98); CV death of 1.3% (HR, 0.69; 95% CI, 0.52–0.92); all-cause death of 1.7% (HR, 0.71; 95% CI, 0.56–0.90).18 In other words, in those with baseline LDL-C ≥100 mg/dL, NNT for primary endpoint, CV death, and all-cause death was around 29, 77, and 59, respectively.
Overall adverse events in the alirocumab group did not differ from the placebo groups except injection-site reactions (3.8% vs. 2.1%).18 Development of new-onset diabetes was similar between alirocumab and placebo groups (9.6% vs. 10.1%). In the ODYSSEY Outcomes trial, the development of binding or neutralizing antibodies to alirocumab was not known yet. However, in the previous phase 3 ODYSSEY trials, detection rate of antidrug antibodies (ADAs) was low (transient, 5.1% and persistent, 1.4%) and LDL-C lowering effect of alirocumab was similar and maintained over time regardless of ADA status.30
In summary of the ODYSSEY Outcomes trial, alirocumab effectively decreased LDL-C level by 55% at 48 months when added on statin therapy. In patient with acute coronary syndrome within a year, alirocumab reduced the risk of primary efficacy endpoint by 15% (ARR, 1.6%) and all-cause death (ARR, 0.6%).18 Greater risk reduction was observed in patients with higher baseline LDL-C (≥100 mg/dL): ARR of 3.4% for primary endpoint and 1.7% for all-cause death. Overall, alirocumab treatment was safe and well-tolerated during the trial.
SPIRE-1, 2 TRIALS (BOCOCIZUMAB)
In contrast to evolocumab and alirocumab, which are fully human monoclonal antibody, bococizumab is a humanized monoclonal antibody retaining about 3% of the murine sequence in the antigen-binding complementarity-determining region.19 During the 6 Studies of PCSK9 Inhibition and the Reduction of Vascular Events (SPIRE) lipid-lowering trials, ADAs to bococizumab has developed at a high rate. In addition, development of high-titer of ADA was associated with attenuation of LDL-C lowering effect of bococizumab over time. Another issue with bococizumab was wide variation in LDL-C lowering and this was occurred even in those without ADA.31 Based on these results, the sponsor decided to discontinue further development of bococizumab in November 2016. Therefore, event-driven CV outcome trials with bococizumab, SPIRE-1 and -2, were terminated earlier than originally planned.19 The following is the result of SPIRE-1 and -2 with median follow-up of 10 months. The SPIRE-1 and -2 studies were randomized, double-blind, placebo-controlled trials that enrolled patients: 1) with or at high risk for CV event; and 2) with LDL-C level ≥70 mg/dL or non-HDL-C ≥100 mg/dL in SPIRE-1; LDL-C ≥100 mg/dL or non-HDL-C ≥130 mg/dL in SPIRE-2 (Table 1). All patients had received statin therapy at least the previous 4 weeks unless they had complete statin intolerance. A total of 27,438 patients (16,817 in SPIRE-1 and 10,621 in SPIRE-2) were randomly assigned to receive subcutaneous injections of bococizumab (150 mg every 2 weeks) or placebo.1932 The primary endpoint was the composite of non-fatal MI, non-fatal stoke, hospitalization for UA, or CV death. The secondary endpoint was the composite of non-fatal MI, non-fatal stroke, or CV death.
The mean age of participants was 62.9 years, and 70.4% of them were men. Patients with previous CVD, hypertension, and diabetes were 84.5%, 80.0%, and 47.5%, respectively, and 84.5% of patients were taking high-intensity statin. Baseline mean LDL-C level was 109 mg/dL in all patients, but patients participated in SPIRE-2 had higher baseline LDL-C level than those in SPIRE-1 (133 vs. 94 mg/dL).19 Bococizumab treatment significantly reduced LDL-C levels by 64% at 14 weeks. However, reduction in LDL-C levels in the bococizumab group was attenuated over time: 42% at 52 weeks and 38% at 104 weeks. Consistent with finding in the previous 6 SPIRE lipid-lowering trials,31 the LDL-C lowering-effect of bococizumab showed wide individual variation in SPIRE-1 and -2.19 During median follow-up of 7 months in SPIRE-1, the primary endpoint occurred in 173 patients both in the bococizumab (3.01%) and placebo (3.02%): HR of 0.99 (95% CI, 0.80–1.22; p=0.94). By contrast, in SPIRE-2 with longer median follow-up of 12 months, the primary endpoint occurred in 179 patients (3.32%) in the bococizumab (3.01%) and 224 patients (4.19%) in the placebo group: HR of 0.79 (95% CI, 0.65–0.97; p=0.02). As mentioned earlier, patients enrolled in SPIRE-2 had higher level of LDL-C compared to those in SPIRE-1. This suggests that bococizumab treatment has a benefit in higher-risk patients.
Although serious adverse events were similar in the 2 groups, overall adverse events were higher in the bococizumab group compared with the placebo groups. High rate of injection-site irritation/reaction in the bococizumab group primarily accounted for increased adverse events (16.8% vs. 3.6% for injection-site irritation and 10.4% vs. 1.3% for injection-site reaction; both p<0.001). Compared with the placebo group, blood glucose level slightly increased (1.7 mg/dL) in the bococizumab group. However, there was no difference either in new-onset diabetes or glycated hemoglobin levels between the groups. The status of ADA has not been known yet in SPIRE-1 and -2 trials. In the previous 6 SPIRE lipid-lowering trials ADA and neutralizing antibodies were detected in 48% and 29%, respectively, of the patients receiving bococizumab.31
In summary of SPIRE trials, bococizumab effectively decreased LDL-C level by more than 60% in early period. However, immunogenicity of humanized monoclonal antibodies, not fully human, caused the development of ADA and subsequently attenuation of LDL-C lowering effect of bococizumab. The high rate of injection-site reaction was also attributed to different immunogenicity. These results led to early termination of SPIRE-1 and -2 trials. Nevertheless, bococizumab treatment significantly reduced the risk of primary and secondary endpoint by more than 20% (ARR, 0.9%) in higher-risk patients.
CONCLUSION
During short- to medium-term follow-up, PCSK9 inhibitors reduced LDL-C by 50% or more and decreased major CV events in patients with the atherosclerotic CVD. These results have verified CV benefit by lowering of LDL-C levels below current goals and, thus, reinforce the current concept, ‘the lower, the better.’ The magnitude of the risk reduction in CV outcomes tended to increase over time. In addition, these benefits appeared to be greater in those having high risks such as PAD, diabetes, recent or multiple CV events, residual multivessel disease, and higher baseline LDL-C or hsCRP levels. Taken together, although change in ARR was modest, it will be expected to be greater in patients with high risks and over time. Regarding safety, in contrast to humanized monoclonal antibodies, fully human PCSK9 inhibitors were generally safe and well-tolerated.
As most clinical trials with PCSK9 inhibitor as well as CV outcomes trials were conducted in high risk patients, studies including patients with lower risk and more diverse populations are need. In addition, as there is only one study showing the benefit of mortality, further large trials with long term follow-up are warranted. Aside from the issues of frequent subcutaneous injection in clinical practice, cost-effectiveness is one of the most important disadvantages of PCSK9 inhibitors. Although comparisons of results from different clinical trials are essentially inappropriate because of different populations through different protocols and different sites, with respect to NNT, the CV benefit of PSCK9 inhibitor may be comparable to statin, sodium glucose co-transporter 2 inhibitor or glucagon like peptide-1 receptor agonists, which have demonstrated CV benefit (Table 3).33343536 Therefore, if further analysis is performed to determine specific populations having cost-effectiveness, the future of PCSK9 inhibitor may be prosper.
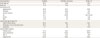
Table 3
Comparison of the NNT of PCSK9 inhibitors with other drugs

| Class | Study | Outcome | NNT | Year |
|---|---|---|---|---|
| Statin36 | Mortality | 83 | 5 | |
| Non-fatal MI | 39 | 5 | ||
| Stroke | 125 | 5 | ||
| PCSK9 inhibitor | FOURIER (evolocumab)1423242526 | CV death, MI, stroke, or coronary revascularization | 20 | 5 |
| 27* | 3 | |||
| 37† | 3 | |||
| 29‡ | 3 | |||
| 27§ | 3 | |||
| 28∥ | 3 | |||
| 38¶ | 3 | |||
| CV death, MI, or stroke | 50 (30) | 3 (5) | ||
| ODYSSEY (alirocumab)18 | CHD death, non-fatal MI, ischemic stroke, or UA requiring hospitalization | 29** | 2.8 | |
| CV death | 77** | 28 | ||
| All-cause mortality | 59** | 2.8 | ||
| SGLT2 inhibitor | EMPA-REG OUTCOME (empagliflozin)33 | Death from CV causes, non-fatal MI, or non-fatal stroke | 63 | 3.1 |
| GLP-1 RA | LEADER (liraglutide)34 | Death from CV causes, non-fatal MI, or non-fatal stroke | 53 | 3.8 |
| SUSTAIN-6 (semaglutide)35 | CV death, non-fatal MI, or non-fatal stroke | 44 | 2 |
NNT; number needed to treat, PCSK9; proprotein convertase subtilisin/kexin type 9, MI; myocardial infarction, CV; cardiovascular, CHD; coronary heart disease, UA; unstable angina, SGLT2; sodium glucose co-transporter 2, GLP-1 RA; glucagon like peptide-1 receptor agonist, hsCRP; high sensitivity C-reactive protein.
*In patients with peripheral artery disease, †diabetes, ‡MI within prior 2 years, §residual multivessel disease, ∥≥2 prior MI, ¶higher baseline hsCRP, and **baseline LDL-C ≥100 mg/dL.
 XML Download
XML Download