

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since 1959, the American Joint Committee on Cancer (AJCC) has published seven editions of the tumor-node-metastasis (TNM) system for cancer staging. In 2017, the 8th edition was announced, in which the revisions were based on the highest level of evidence from newly acquired clinical and pathological data (1). In a fundamental change, breast cancer is now considered as a group of diseases with different molecular characteristics that indicate different prognoses, patterns of recurrence, disseminations, and sensitivities to available therapies (2). Therefore, the committee incorporated biomarkers (histologic grade, hormone receptor, HER2 expression, and multigene panels) into the traditional anatomic TNM staging (1). Here, we introduce the major changes of the 8th edition of the AJCC staging system of breast cancer to radiologists, by presenting representative cases that will be staged differently under the new system. The changes in the 8th edition are briefly summarized in Table 1.
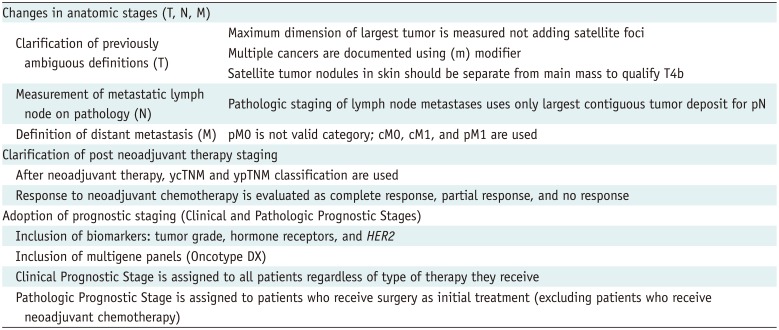
Table 1
Summary of Changes in 8th Edition
![]()
Go to : 
Brief Overview of the 7th Edition
The 7th edition of the AJCC staging system was mainly based on anatomical staging, which used the extent of the primary tumor (T), status of the regional lymph nodes (N), and metastasis status (M). This has remained largely unchanged in the 8th edition. The T stage is based on the size and degree of loco-regional invasion by the primary tumor and is categorized from T1 to T4. The N stage is determined by the extent of nodal involvement including axillary, internal mammary, and ipsilateral supraclavicular lymph nodes. Distant metastases are evaluated to determine the M stage. The 7th edition used nine stages (0, IA, IB, IIA, IIB, IIIA, IIIB, IIIC, and IV) based on different combinations of T, N, and M status (Table 2).
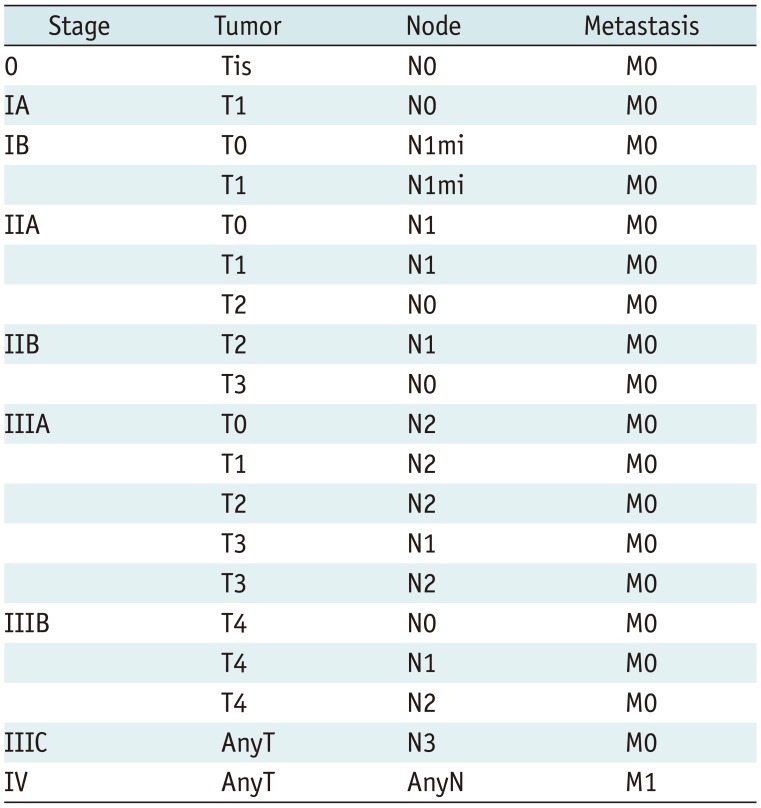
Table 2
7th Edition of American Joint Committee on Cancer Staging System for Breast Cancer
![]()
Go to :
Changes in the Anatomic Stage
The AJCC committee maintained the anatomic stages for countries in which the tests for biomarkers were unavailable and for uniformity in terminology with past studies and different researchers. In the 8th edition, the fundamental rules for anatomic staging have not been changed, but several previous ambiguous definitions have been clarified.
Tumor
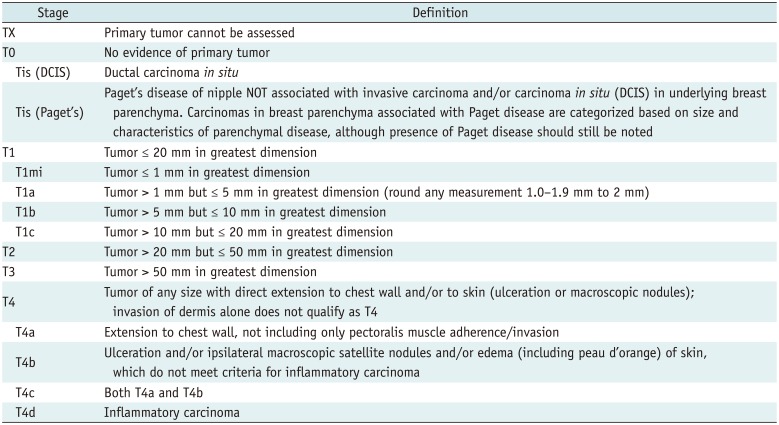
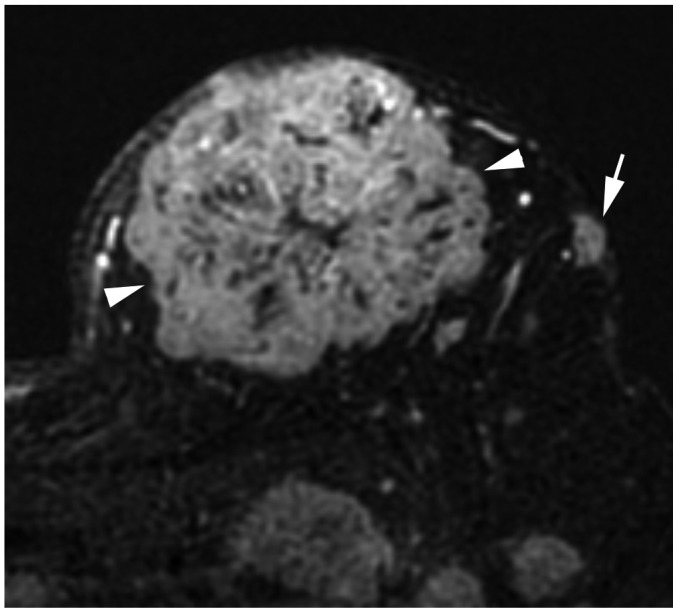
In the 8th edition, lobular carcinoma in situ has been removed from the in situ carcinoma (pTis) category and classified as a benign entity. Except for invasive carcinoma and ductal carcinoma in situ (DCIS) being included in the staging system, the criteria for the T categories remain the same as those in the 7th edition. DCIS and Paget disease of the nipple, not associated with parenchymal carcinoma, are classified as Tis (DCIS) and Tis (Paget disease). Categories T1–3 have been assigned to an invasive carcinoma without loco-regional invasion according to the size of the invasive component (Table 3). For staging, the maximum invasive tumor size is measured because it is a reasonable estimate of the tumor volume (Fig. 1) (3). The 8th edition clarifies that only the maximum dimension of the largest tumor is measured, without adding small microscopic satellite foci of the tumor. In that case, multiple cancers are documented using the modifier (m) (Fig. 2). On imaging, the measurement of the largest tumor should be combined with the size of microcalcifications or architectural distortions associated with the primary tumor, because they could influence the surgical extent. The T1 category is defined as a tumor of 20 mm or less and is divided into T1mi (≤ 1 mm), T1a (> 1 mm but ≤ 5 mm), T1b (> 5 mm but ≤ 10 mm), and T1c (> 10 mm but ≤ 20 mm); T2 category are tumors > 20 mm but ≤ 50 mm; T3 category are tumors > 50 mm (1). The T4 category is assigned when there is either chest wall or skin invasion by the breast cancer cells. Extension into the chest wall is T4a category and it means invasion of the ribs, intercostal muscles, and serratus anterior muscle; however, invasion of only the pectoral muscles does not qualify as T4. Magnetic resonance imaging (MRI) provides a more accurate assessment of chest wall extension than mammography or ultrasound (4). Satellite tumor nodules in the skin are T4b, but the nodules must be separate from the primary tumor and macroscopically identified (Fig. 3). Ulceration or edema of less than one-third of the skin of the breast, which does not qualify as inflammatory breast cancer (IBC), is regarded as T4b. On the MRI, direct skin invasion causes skin thickening, multiple nodules, ulceration, and a fungating mass (5). Invasion of the dermis alone does not qualify as T4; a T4c category is determined when conditions of both T4a and T4b are met (Fig. 4). IBC (T4d) is primarily a clinical diagnosis made when diffuse erythema and edema involving at least one-third of the skin of the breast is observed (Fig. 5). It is highly aggressive with rapid evolution and is associated with poor prognosis (67); therefore, a neglected, locally advanced breast cancer should not be classified as IBC. On mammography, IBC presents as diffuse skin thickening and trabecular distortion, whereas, on ultrasound, it presents a mass or parenchymal distortion and diffuse skin thickening. On MRI, the primary lesions present mostly as multiple small, confluent, enhancing nodules accompanied with diffuse skin thickening (89). For the T staging of breast cancer on imaging, the longest diameter should be measured, multiple tumor nodules should be identified, and loco-regional invasion should be evaluated by careful examination of the nipple, skin, and underlying chest wall.
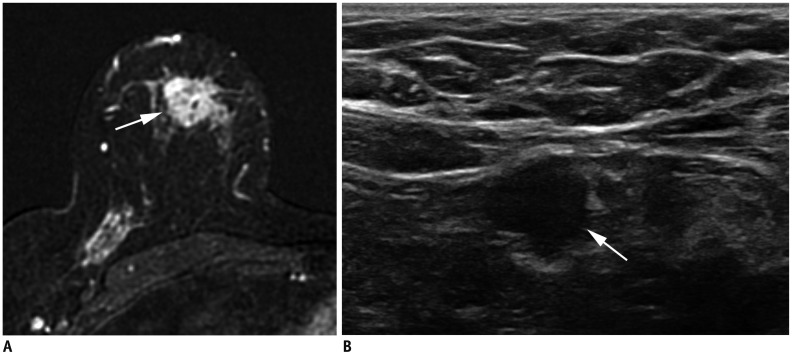
 | Fig. 1Measurement of tumor size.Maximum tumor size measures 4.3 cm on ultrasound image (arrow). It also measures 4.3 cm pathologically. Therefore, both clinical and pathologic T category is T2. T = tumor
|
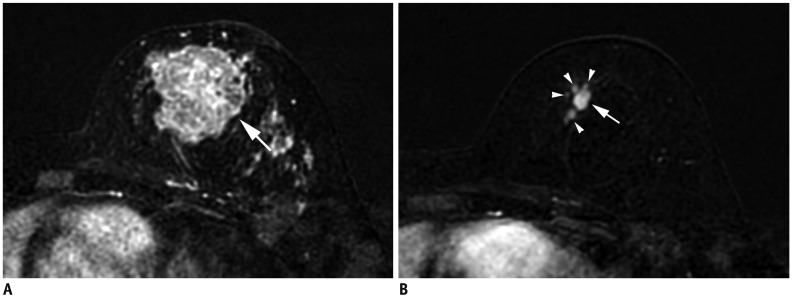
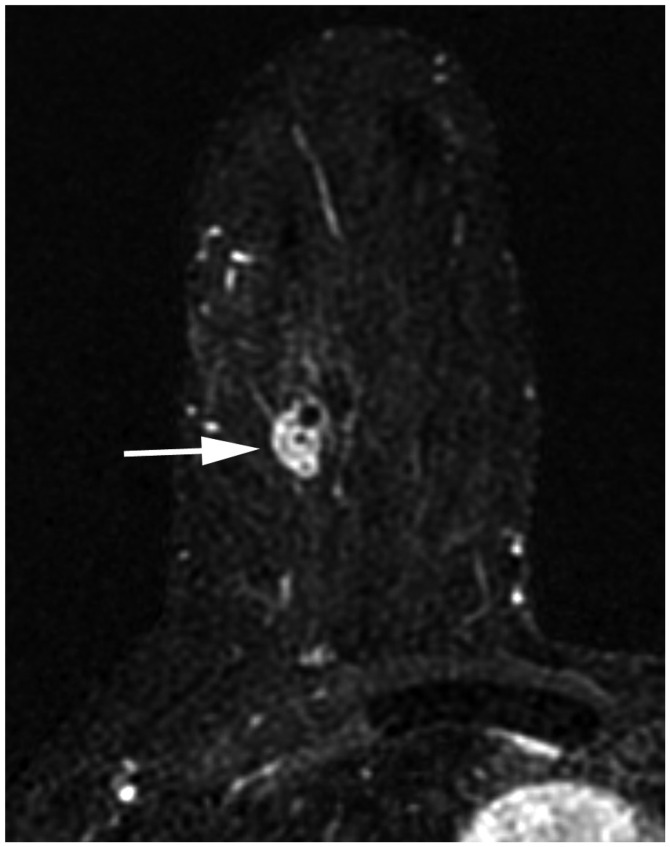
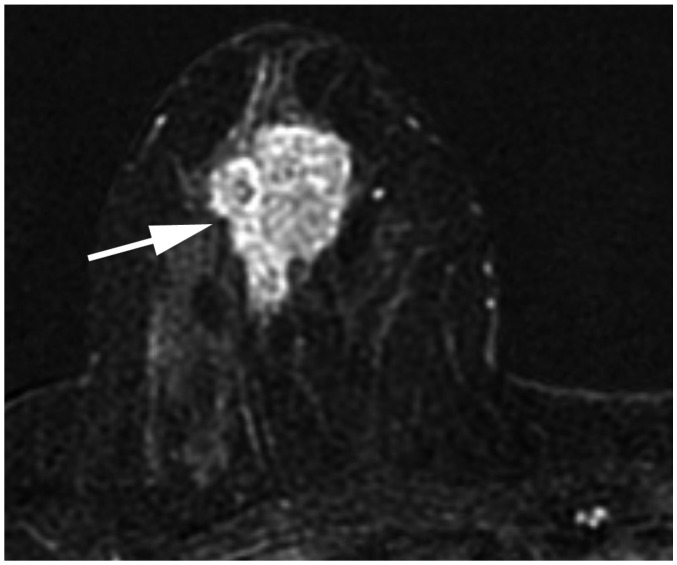
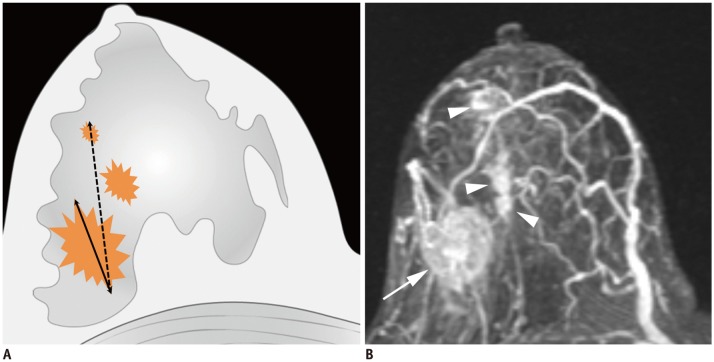 | Fig. 2Determination of T categories.
A. Maximum size of largest tumor is measured (solid line), but size of smaller tumors is not added (dotted line). B. Magnetic resonance maximum intensity projection image demonstrates multiple synchronous tumors in breast. Maximum invasive size of largest tumor is 2.4 cm (arrow), and size of smaller tumors (arrowheads) is not added. Therefore, cT2 (m) is designated for T stage.
|
 | Fig. 3T4b breast cancer.MRI shows primary breast cancer in left upper breast (arrowheads). Separate skin nodule is identified at left upper outer part, which qualifies as T4b (arrow). MRI = magnetic resonance imaging
|
 | Fig. 4T4c breast cancer.
A. MRI shows left breast cancer with skin ulceration (arrow) and rib extension (arrowheads). B. Physical examination shows ulceration extending to less than one third of breast, which does not meet definition of IBC. IBC = inflammatory breast cancer
|
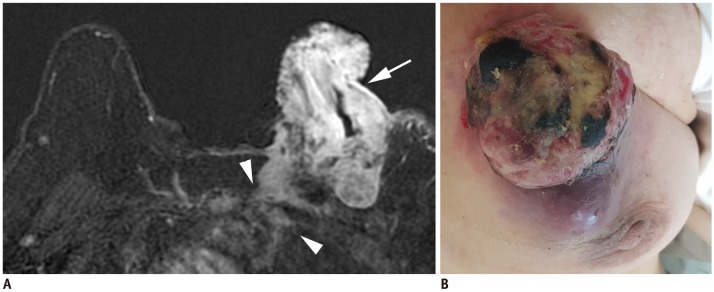
 | Fig. 5Left IBC (T4d).
A. MRI shows diffuse skin enhancement (arrowheads) and chest wall extension (arrow). B. Physical examination of left breast shows erythema and peau d'orange (orange peel skin) appearance of skin, which meets definition of IBC.
|
Table 3
Definition of Primary T Categories
![]()
Lymph Nodes
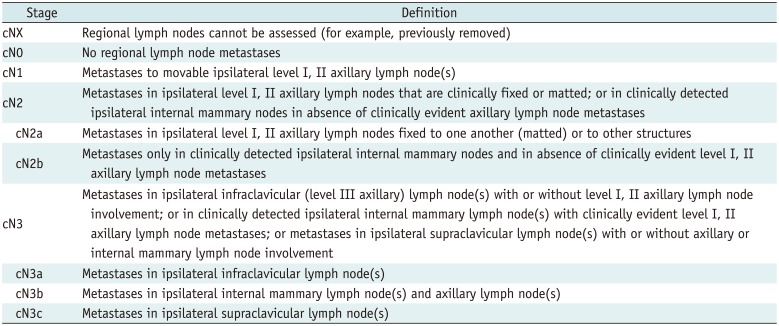
Unlike T categories, nodal staging uses separate clinical N (cN) and pathologic N (pN) categories. For the clinical evaluation of the node status, the 8th edition does not contain any significant changes from the 7th edition (Table 4). Although the clinical stage can be determined without an imaging evaluation, imaging is valuable in assessing regional lymph node metastases. The method of confirmation of metastatic lymph nodes should be noted: cN, confirmed by clinical findings; cN(f), confirmed by fine-needle aspiration or core biopsy; or cN(sn), confirmed by sentinel node biopsy. The regional lymph nodes occur in the ipsilateral axillary, ipsilateral internal mammary, and ipsilateral supraclavicular areas. The levels of axillary lymph nodes are defined using the pectoralis minor muscle as a landmark: level I lymph nodes are on the lateral border of the pectoralis minor muscle, level II nodes are between the medial and lateral borders of the pectoralis minor muscle, and level III nodes are on the medial border of pectoralis minor muscle. Imaging findings for metastatic axillary lymph nodes include loss of fatty hilum, eccentric cortical thickening, round shape, extranodal extension, and marked hypoechoic cortex on the ultrasound (10); round or irregular shape, increased density, or loss of fatty hilum on mammography (11); and loss of fatty hilum (12), round shape (13), and eccentric cortical thickening on MRI (1314). The cN1 indicates metastases to one or more movable, ipsilateral, levels I and II axillary lymph nodes. The cN2a indicates metastases to fixed, ipsilateral, levels I and II axillary lymph nodes; cN2b indicates metastases to ipsilateral internal mammary lymph nodes without evidence of axillary lymph node metastases. The cN3a indicates ipsilateral level III lymph nodes regardless of the status of levels I and II axillary lymph (Fig. 6); cN3b indicates both ipsilateral internal mammary and axillary lymph node metastases (Fig. 6); and cN3c indicates ipsilateral supraclavicular lymph node metastases (Fig. 6).
 | Fig. 6cN3 category.
A, B. cN3a: Ultrasound images from right breast cancer case show enlarged hypoechoic lymph nodes with loss of fatty hilum not only in right axilla (A) level II (arrows), but also on (B) level III (arrow). Note pectoralis minor muscle (arrowheads), which is landmark for grouping axillary lymph nodes. C, D. cN3b: (C) MRI of case of cancer in right breast shows enlarged lymph nodes in right axilla (arrow). (D) Enlarged right internal mammary lymph node is also noted (arrowhead). E, F. cN3c: (E) Ultrasound of left breast cancer case shows enlarged lymph node in left axilla (arrow). (F) Enlarged left supraclavicular lymph node is also noted (arrowhead). AX = axilla
|
Table 4
Definition of Clinical Regional Lymph N Categories
![]()
The 8th edition clearly indicates that pathologic staging of lymph node metastases uses only the largest contiguous tumor deposit for pN. Pathologic classification is defined by the regions of lymph nodes involved and the number of ipsilateral axillary lymph node metastases (Table 5). The American College of Surgeons Oncology Group Z0011 trial sparked debates about whether an imaging evaluation of axillary lymph nodes should be performed (1516). Since patients with T1 or T2 tumors, undergoing only a sentinel node biopsy, did not have an inferior survival rate compared to those who received a complete axillary node dissection, some researchers argued that an imaging evaluation of axillae for early stage breast cancer was unnecessary (16). However, the axillary evaluation retained its importance in other studies (1718). An evaluation of the axillary lymph nodes should cover both levels I and II. When lymph node metastases are suspected, the level III internal mammary chain, and supraclavicular area should also be evaluated.
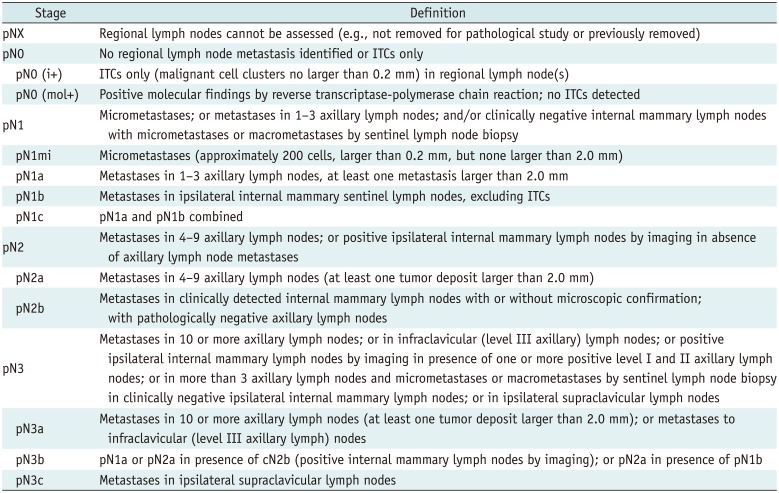
Table 5
Definition of Pathologic Regional Lymph N Categories
![]()
Metastasis
Stage M1 is designated when distant metastases are found, including contralateral lymph node metastases (Table 6). Metastases can be detected in various imaging studies. The 8th edition clarifies that pM0 is not a valid category; benign biopsy of a suspicious lesion does not guarantee the absence of metastatic lesions elsewhere, and therefore, only cM0, cM1, and pM1 grades are used. The most common sites of breast cancer metastases are bone, lung, brain, and liver (19). Category M1 indicates stage IV disease regardless of T or N status and shows the poorest prognosis. For patients with stage I-IIB, systemic evaluation including bone scan, abdominal computed tomography (CT), or chest CT is only recommended when there are clinical signs, symptoms, or laboratory abnormalities suggesting metastases. For patients with a locally advanced disease, screening systemic evaluation using positron emission tomography can be performed (Fig. 7) (20).

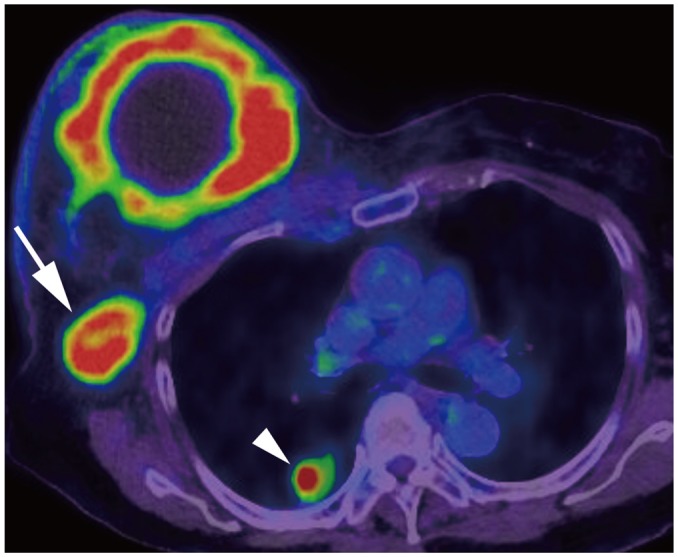 | Fig. 7Right breast cancer with lung metastasis (M1).On positron emission tomography-computed tomography, 10-cm cancerous mass is seen in right breast and multiple FDG uptakes are seen in right axillary lymph nodes (arrow); there are lung nodules with FDG uptake, suggesting lung metastasis (arrowhead). FDG = fludeoxyglucose, M = metastasis
|
Table 6
Definition of Distant M Categories
![]()
Post-Neoadjuvant Therapy Staging
Neoadjuvant therapy is widely performed in locally advanced breast cancer, IBC, and even operable breast cancer (21). After neoadjuvant therapy, the y prefix is used. The ycT is determined by measuring the largest single focus of the residual tumor by examination or imaging (Fig. 8). When there is no residual disease, it is classified as ycT0. IBC (cT4d) retains the same classification stage even if complete resolution of the tumor is observed. The ycN is determined by clinical or radiographic findings of residual lymph nodes. Pre-treatment M1 disease is designated as M1 throughout treatment. When surgery is performed after neoadjuvant chemotherapy, the yp classification is applied. The response to neoadjuvant chemotherapy is evaluated as complete response (CR), partial response, or no response. CR is designated to the tumor when residual invasive cancer is not found in the breast tissue and lymph nodes, clinically or pathologically (Fig. 9). The presence of in situ cancer constitutes a pathologic CR. Partial response is defined as a decrease in the T or N category without any evidence of increase in either the T or N category. No change or an increase in the T or N category is defined as no response.
 | Fig. 8Size measurement after neoadjuvant chemotherapy.
A. Initial MRI shows 4.3-cm irregular breast cancer in left breast (T2) (arrow). B. After neoadjuvant chemotherapy, cancer reduced to multiple small masses (arrowheads); largest one measures 10 mm (arrow). Therefore, post treatment T category is ycT1b (m).
|
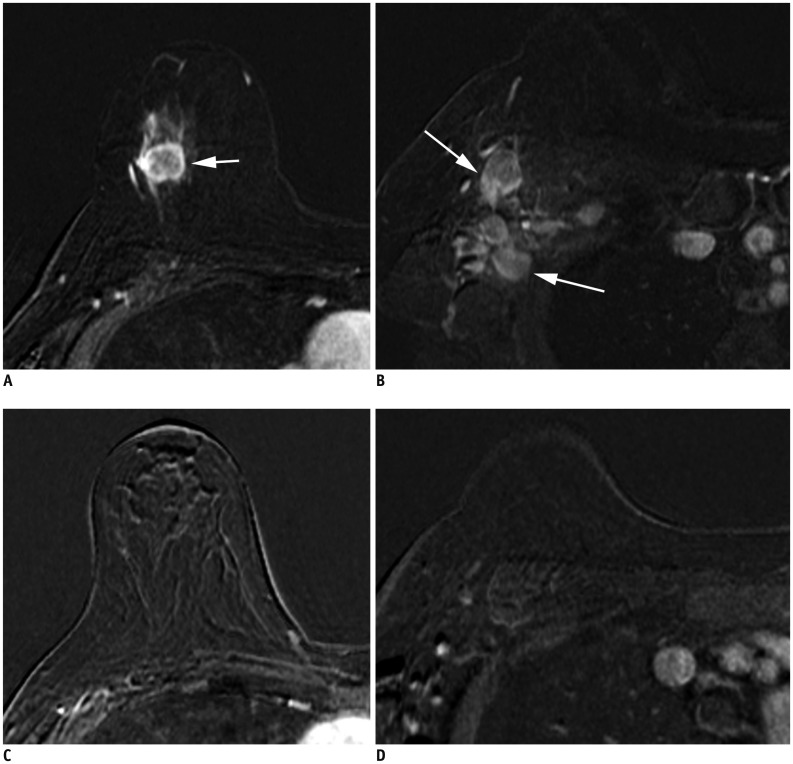 | Fig. 9Patient with cancer in right breast with MRI before (A, B) and after neoadjuvant chemotherapy (C, D).
A. Initial MRI shows 2.2-cm right breast cancer (arrow). B. Ipsilateral matted axillary lymph node enlargement is noted (arrows). Initial stage is T2N2aM0. C. After neoadjuvant chemotherapy, there is no residual mass. D. Axillary lymph nodes have disappeared, which suggests clinical CR (ycT0N0M0). Histopathologic evaluation shows absence of invasive carcinoma in breast and lymph nodes, indicating pathologic CR (ypT0N0M0). CR = complete response
|
Go to :
Adoption of the Prognostic Stage
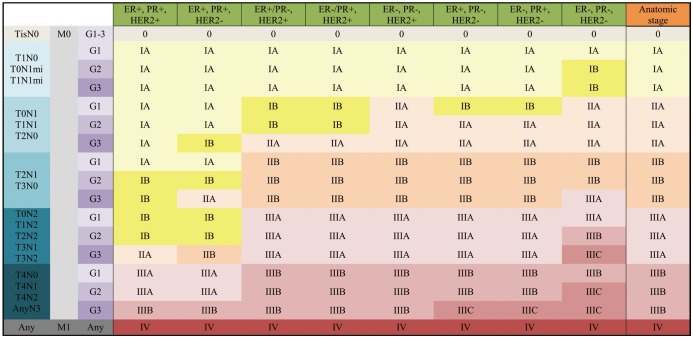
For the 8th edition, the AJCC committee created the prognostic staging protocol. This integrates biomarkers into the TNM staging system, making use of the results from large cohort studies, which shows that not only pathologic stage, but also different biomarkers could affect survival (122). The biomarkers indicate tumor grade, hormone receptor status, and HER2. Multigene panel status is also incorporated into the staging system in limited sub-groups. The 8th edition defines clinical and pathologic prognostic stages that combine anatomic staging with tumor grade, hormone receptor status, and HER2 status (Figs. 10, 11).
 | Fig. 10Clinical Prognostic Stage is assigned to all patients regardless of type of therapy given.ER− = estrogen receptor-negative, ER+ = ER-positive, G = grade, HER2− = HER2 negative, HER2+ = HER2-positive, mi = micrometastasis, PR− = progesterone receptor-negative, PR+ = PR-positive, Tis = in situ
|
Tumor Grade
Tumor grade is an important prognostic factor independent of the tumor size and number of positive lymph nodes (23). Tumor grade reflects tumor differentiation with worse prognosis observed in tumors with a high histologic grade or poor differentiation, than those with a low grade or well-differentiated (Fig. 12) (24). A modified Scarff-Bloom-Richardson system measuring tubules (glands), nuclear pleomorphism, and mitotic counts is used to evaluate the tumor grade (2425).
 | Fig. 12Right breast cancer with low histologic grade.
A. MRI demonstrates breast cancer measuring 2.3 cm in upper breast (arrow). B. Ultrasound shows enlarged, right axillary lymph node with eccentric cortical thickening (arrow). After partial mastectomy, cancer measures 2.5 cm with two level-I lymph node metastases. Cancer is ER+/PR+ and HER2−. Histologic grade is 1, and anatomic stage is IIB (T2N1M0). However, due to low histologic grade and biomarker status, Clinical Prognostic Stage is IIA and Pathologic Prognostic Stage is IA.
|
Hormone Receptor and HER2 Expression
Evaluating the expression of estrogen receptors (ERs) and progesterone receptors (PRs) in breast cancer is important, because selective ER modulators slow the progression of ER-positive and PR-positive tumors (2627). Furthermore, breast cancer is related to several oncogenes including HER2. The presence of HER2 is associated with a poor prognosis in untreated patients (282930). However, HER2 targeting agents (trastuzumab) improve the prognosis for patients with HER2 positive tumors (3132). A high Ki-67 level reflects rapidly dividing tumor cells, although there is no universal cut-off for measuring Ki-67 levels (3334). According to the ER/PR and HER2 status and with additional information about Ki-67, the 8th edition identifies four subtypes: luminal A (hormone receptor-positive, HER2-negative, low Ki-67), luminal B (hormone receptor-positive, HER2-negative, high Ki-67), HER2 (HER2-positive regardless of the hormone receptor status), and basal (both hormone receptor and HER2 negative) (3536). The luminal A type has the best prognosis, with excellent response to endocrine therapies. The luminal B type is less responsive to endocrine therapies and has worse prognosis than the luminal A type. The HER2 type responds to HER2 targeting agents and proper treatment improves the prognosis. The basal type, also known as a triple-negative tumor, has the worst prognosis (Fig. 13).
 | Fig. 13cT1N0M0 cancer.MRI shows that cancer measures 1.3 cm (arrow). There is no suspicious lymph node enlargement. Pathology shows 0.9-cm grade-2 carcinoma, but no hormone receptor or HER2 overexpression is noted. Therefore, anatomic stage is IA (T1N0M0), but it is triple negative cancer; thus, Clinical and Pathologic Prognostic Stages are higher, IB.
|
Multigene Panel Status
Multigene panel tests measure the expression levels of a large number of genes in breast cancer tissue, and several panels are available for the same. Among them, Oncotype DX has the best available evidence, and thus, it is the one incorporated into the 8th edition (3738394041). Based on this evidence, patients with hormone receptor-positive, HER2-negative, and lymph node-negative tumors with a recurrence score less than 11 on the Oncotype DX, are placed into stage I (T1a-T1bN0M0) regardless of T size. Other multigene panels, including Mammaprint (42), EndoPredict (4344), PAM50 (4546), and the Breast Cancer Index (4748) have shown results similar to those of Oncotype Dx, but at present they are not included in the TNM staging system.
Prognostic Stage Groups
Two large cohorts, the MD Anderson Cancer Center study (22) and the National Cancer Data Base (NCDB) study (David JW, unpublished data), were analyzed to incorporate biomarkers into prognostic staging (1). The first study identified risk profiles using not only pathologic stages, but also high tumor grade, ER-negative status, and HER2-negative status (2249). The second unpublished study used the NCDB to reveal that patients with triple-negative tumors, regardless of grade, should be categorized at least one stage higher than other sub-types (David JW, unpublished data). Grade-3 tumors, HER2-negative, and ER-negative or PR-negative tumors should also have a higher stage (Fig. 14). Patients whose tumors expressed both ER and PR, with or without HER2 over-expression, had better survival (Fig. 15). Based on that study, the 8th edition defines Clinical and Pathologic Prognostic Stages that combine anatomic staging with tumor grade, hormone receptor (ER/PR) status, and HER2 status. A Clinical Prognostic Stage is assigned to all patients regardless of the type of therapy they received (Fig. 10). A Pathologic Prognostic Stage is assigned to patients who receive surgery as the initial treatment, excluding patients who receive neoadjuvant chemotherapy (Fig. 11). Using the NCDB data, three-year overall survival rate was calculated with the inclusion of grade, hormone receptor, and HER2 status. These results were compared with the 7th edition, and downstaging or upstaging was performed for the 8th edition. Additionally, pT1-T2, pN0, M0, ER-positive, and HER2-negative cancers were assigned as Pathologic Prognostic Stage group IA, when the Oncotype Dx recurrence score was less than 11 (Fig. 16).
 | Fig. 14cT2N0M0 cancer.MRI shows 3.7-cm enhancing cancer (arrow). No axillary metastasis is found. Anatomic stage is IIA. Tumor grade is 3, and hormone receptor and HER2 expressions are negative. This tumor has high histologic grade and is triple-negative; therefore, Clinical Prognostic Stage is higher, IIB.
|
 | Fig. 15cT3N1M0 cancer downgraded by prognostic stage.
A. Ultrasound image indicates complex cystic and solid mass in left lower outer breast (arrows). B. Left axillary ultrasound image shows cortically thickened lymph node (arrow). Anatomic stage is IIIA. Tumor grade is 1, ER and PR expression are found, and HER2 shows no overexpression; therefore, Clinical Prognostic Stage is IIA, and Pathologic Prognostic Stage is IB.
|
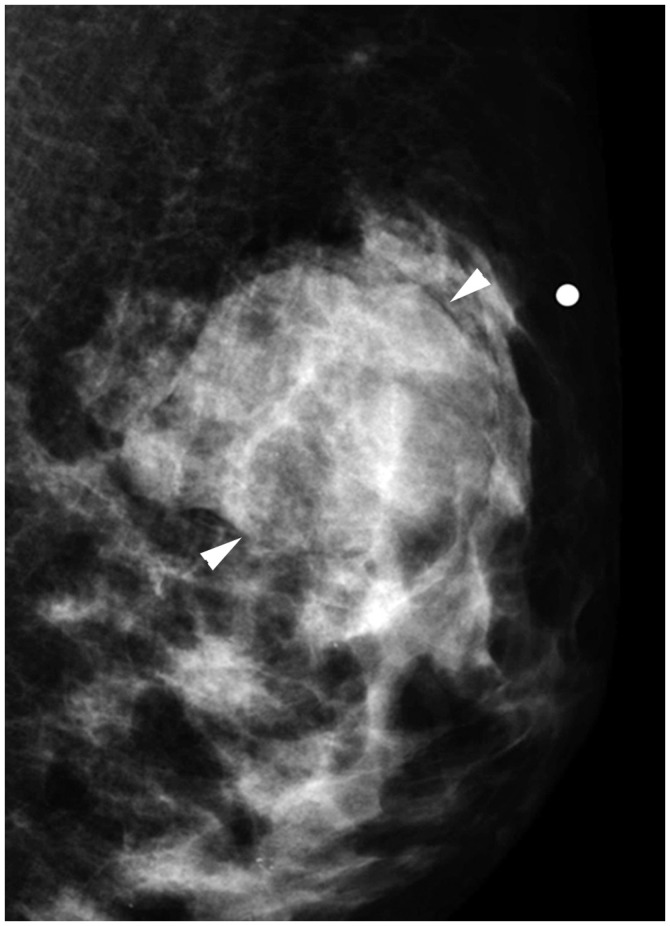 | Fig. 16cT2N0M0 cancer.Mediolateral oblique mammographic view demonstrates mass in left upper outer breast (arrowheads). Lymph nodes are not enlarged. Anatomic stage is IIA. Tumor is ER expression positive, HER2 shows no overexpression, and Oncotype Dx recurrence score is 5; therefore, Pathologic Prognostic Stage is IA.
|
Go to :
CONCLUSION
In the 8th AJCC staging system of breast cancer, anatomic staging is maintained and the traditional role of radiology remains important. Anatomic staging is still the main system when immunohistochemical examinations are unavailable. However, radiologists should understand the importance of biomarkers in breast cancer staging. Different prognostic stages are assigned to tumors with the same anatomic stage depending on the histologic grade, hormone receptor status, HER2 status, and multigene panels. Different prognostic stages will call for different therapies for breast cancers with the same anatomic stage; therefore, radiologists' role in evaluating tumor response after appropriate therapies is also important.
Go to :
 XML Download
XML Download