

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast cancer is the most common malignancy in women worldwide, and the first-line choice of treatment is surgery. For the best surgical plan, preoperative evaluation using contrast-enhanced magnetic resonance imaging (CEMRI) is an important and accurate modality for the assessment of tumor extent and for decision making regarding surgical strategy for patients with breast cancer [1]. Dynamic CEMRI depicts morphological features and perfusion characteristics of lesions related to neo-angiogenesis. It is also sensitive for identifying multifocal, multicentric, and contralateral disease [2]. Although it has a high sensitivity―ranging from 88% to 100%―the specificity and positive predictive value (PPV) of CEMRI are limited, given that both benign and malignant lesions demonstrate enhancement [3]. Additionally, it is more expensive, time consuming, and not easily accessible compared with conventional mammography, which itself has limited availability [4].
Along with the development of digital mammography, a novel technique known as contrast-enhanced digital mammography (CEDM) was first introduced by Lewin et al. [5] in 2003. It detects angiogenesis in breast cancer by tracking the uptake of iodine-based contrast agent in breast tissues. Several preliminary studies have demonstrated that CEDM provides useful information regarding morphology and vascular enhancement, similar to that of CEMRI [6]. CEDM has also demonstrated comparable diagnostic performance to CEMRI in terms of detecting index breast cancer and multifocal cancers, and the estimation of tumor extent [6]. CEDM depicts angiogenesis of breast cancer similar to CEMRI. CEDM improves the sensitivity of breast cancer detection while maintaining specificity because of its higher contrast and better lesion delineation than mammography alone, even in dense breasts [7]. CEMRI is, however, associated with a high false-positive (FP) rate and a low specificity for breast cancer detection, leading to overdiagnosis and overtreatment of breast cancer such as the conversion from breast-conserving surgery (BCS) to mastectomy [8].
The role of CEDM as a possible alternative to CEMRI for preoperative evaluation and guidance in appropriate treatment options is gaining acceptance. Clinical results of CEDM have been published during the past few years, and it has been reported that the feasibility of CEDM for detecting primary cancers was similar to CEMRI [9]. However, to the best of our knowledge, there are a few studies that have compared the diagnostic performance and effects of both modalities on surgical management [610].
Accordingly, this prospective study aimed to compare the diagnostic performance of CEDM and CEMRI for the detection of index and secondary cancers (multifocality and multicentricity), and occult cancer in the contralateral breast, in women with newly diagnosed breast cancer, and to determine whether CEDM or CEMRI resulted in changes to the surgical management of the affected breast due to findings detected on imaging.
METHODS
Patient selection
From November 2016 to October 2017, 293 patients were consecutively diagnosed with primary breast cancer at Kangbuk Samsung Hospital, and were invited to enroll in the present study. Patients with contraindications to contrast agent according to the guidelines of the Korean Society of Radiology, such as a history of an allergic reaction [11], were excluded. Patients for whom the plan changed from surgery to neoadjuvant chemotherapy after performing CEDM or CEMRI, and who were initially diagnosed with bilateral breast cancer, were also excluded. Ultimately, 84 patients were included in this single-center, prospective investigation, which was approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 2016-08-016). The Korean Food and Drug Administration approved the use of iodinated contrast material for the purposes of this study. Informed consent was obtained from all patients before initiation of the study. Patients were characterized based on clinical information, such as age at diagnosis, family history of breast cancer, personal history of breast cancer, menopausal status, and reasons for initial presentation.
Contrast-enhanced digital mammography and contrast-enhanced magnetic resonance imaging techniques
Initial mammographic studies were performed using standard craniocaudal (CC) and mediolateral oblique (MLO) views using a full-field digital mammography unit (Lorad Selenia; Hologic, Danbury, USA). Patients underwent breast ultrasonography (US) examinations (iU22 platform, Philips Healthcare, Bothell, USA; Aixplorer, SuperSonic Imagine, Aix-en-Provence, France) using a 5–12 and 5–15 MHz linear transducer.
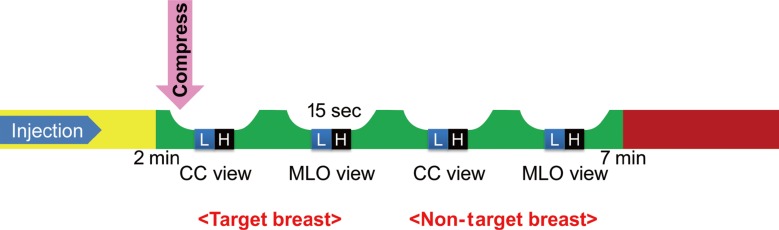
All CEDM examinations were performed within 7 days of CEMRI using a digital mammography device capable of dualenergy CEDM acquisition (Selenia Dimensions; Hologic, Bedford, USA). An intravenous injection of Omnipaque 350 (GE Healthcare, Shanghai, China; 1.5 mL/kg of body weight, with a flow rate of 2 mL/sec using a power injector) was administered to the arm contralateral to the target breast using an 18-gauge needle without compression of the breast. Approximately 2 minutes after the injection, the patient was positioned for CEDM imaging of both breasts, similar to a conventional mammogram. Each view was acquired using a pair of low-energy (Rh or Ag filtration; 26–32 kVp) and high-energy (Cu filtration; 49 kVp) images. Four routine views were acquired within 5 minutes, starting at 2 minutes after the injection (Figure 1). The mean radiation dose per view was 1.2 mGy for digital mammography and <3.0 mGy for CEDM (4.2 cm compressed breast thickness) [12]. The target breast was defined as the side containing the proven malignancy, and the nontarget breast as the opposite side of the proven malignancy. The order of image acquisition was CC and MLO views of the target breast, and CC and MLO views of the nontarget breast (Figure 1). Using post-processing I-view software (Hologic, Bedford, USA), subtraction images of the low- and high-energy acquisitions that emphasized the enhancement of the injected iodine were obtained.
CEMRI was performed using a 3.0-Tesla system (Achieva; Philips Medical System, Best, the Netherlands) equipped with a dedicated 7-channel SENSE breast coil. The following images were acquired after obtaining localized images: T2-weighted (W) turbo spin-echo axial images (repetition time [TR]/echo time [TE], 3,790/100; 332×316 matrix; field of view [FOV], 200×340 mm; slice thickness, 3 mm; gap, 1 mm), T1-W turbo spin-echo axial images (TR/TE, 620/10; 332×332 matrix; FOV, 200×340 mm; slice thickness, 3 mm; gap, 1 mm), and dynamic contrast-enhanced examination using a fat-suppressed T1-W 3D fast field echo sequence (TR/TE, 7.0/3.5; 452×410 matrix; FOV, 340×340 mm; slice thickness, 2 mm; no gap). Finally, delayed axial T1-W spin-echo images (TR/TE, 532/10; 448×378 matrix; FOV, 380×380 mm; slice thickness, 5 mm; gap, 2.5 mm) were acquired for the evaluation of the axilla using a body coil. Six series of axial dynamic CEMRI for both breasts were obtained at 0, 1, 2, 3, 5, and 7 minutes after intravenous injection of 1.0 M gadobutrol (7.5 mL, Gadovist; Bayer Schering Pharma, Berlin, Germany).
Interpretation of contrast-enhanced digital mammography and contrast-enhanced magnetic resonance imaging
All mammography, US, imaging-guided biopsy, and CEMRI reports were completed before surgery by four dedicated breast imaging radiologists (I.Y., S.H.K., S.H.C., and Y.J.C., with 6–24 years' experience in breast imaging) according to the American College of Radiology Breast Imaging Reporting and Data System (BI-RADS) [13]. All patients were examined using CEMRI first, followed by CEDM. The median interval between the two modalities was 5.1 days (range, 1–29 days). CEMRI and CEDM were interpreted on the same day of examination. CEDM results were reviewed by two radiologists (I.Y., S.H.K.), who were blinded to the CEMRI results. The two radiologists interpreted each modality independently. Because there is no current BI-RADS for CEDM, the CEDM results were assessed using a BI-RADS-like classification (scale 1–5) [14]. In the final assessment of the radiological study, benign lesions were classified as categories 1–3, and suspicious lesions as categories 4–6. There were no lesions classified as category 0 for either CEDM or CEMRI.
For CEDM and CEMRI, the visibility and detection of the index and secondary cancers were analyzed. To evaluate secondary cancers, the presence of multifocal or multicentric lesions was analyzed in the ipsilateral breast and occult cancers in the contralateral breast. Multifocal lesions were defined as ≥2 cancer lesions in the same quadrant, and multicentric lesions were defined as ≥2 cancer lesions located in different quadrants [15]. The extent of the background parenchymal enhancement (BPE) in CEDM and CEMRI was classified into two groups using the BI-RADS lexicon, namely, minimal-to-mild and moderate-to-marked degrees [13].
In the case of unexpected additional suspicious enhancing lesions (BI-RADS category 4–5) on CEDM or CEMRI, one of the four radiologists performed a second-look breast US and US-guided core biopsy, or wire localization for excisional biopsy was performed if they had correlated suspicious US findings with CEDM or CEMRI. If there was no suspicious US finding (BI-RADS category 1–3) correlated with an enhanced lesion, postoperative follow-up imaging, including mammography, US or CEMRI, was recommended 6 to 12 months after surgery.
Histopathological analysis
Index cancer was defined as invasive carcinoma and ductal carcinoma in situ (DCIS). The other suspicious lesions in the ipsilateral or contralateral breast were characterized based on their pathological characteristics, such as a histological type of malignancy or benign lesion. All results were based on postoperative histopathological reports of surgical specimens or imaging-guided core or excisional biopsy specimens. Noncancerous (benign) lesions were defined according to the 2012 World Health Organization classification of tumors of the breast [16]. Among the benign lesions, high-risk lesions included lobular carcinoma in situ (LCIS), atypical ductal hyperplasia (ADH), atypical lobular hyperplasia (ALH), atypical columnar cell hyperplasia, usual ductal hyperplasia, papillary lesions of the breast including intraductal papilloma, flat epithelial atypia, radial scar, and sclerosing adenosis [17]. Cancers were counted as positive lesions, and noncancerous lesions were counted as negative lesions.
Lesions were divided using the results of CEDM or CEMRI after surgery as follows: true-positive (TP) lesion, histologically proven malignancy after excision with suspicious finding on CEDM or CEMRI; FP lesion, no suspicious finding (BI-RADS category 1–3) on second-look US or histologically proven benign lesion that showed as a suspicious lesion on CEDM or CEMRI; true-negative (TN) lesion, histologically proven noncancerous lesion without any suspicious findings on CEDM or CEMRI; and false-negative (FN) lesion, proven malignancy without any suspicious findings on CEDM or CEMRI. Previously described definitions of multifocal or multicentric lesions were applied to pathological interpretations [15]. Occult breast cancer in the contralateral breast defined as cancer was only detected on CEDM or CEMRI and not on mammography and US.
Change in surgical management
Patients who underwent US-guided wire localization for an unexpected additional suspicious lesion(s) detected on CEDM or CEMRI were reassessed by the surgeon to determine surgical management. All breast specimens were sent to pathology for intraoperative evaluation. The margin status was classified as positive when invasive or in situ disease was observed at the inked surgical margin, and negative when tumor cells were >2 mm from the inked margin [18]. When tumor cells were positive at the margin, the tumor was designated for wider excision. When the result was positive at the margin after three consecutive margin excisions, BCS was converted to mastectomy. The changes in surgical management due to CEDM or CEMRI findings were divided into three categories as follows: from lumpectomy to mastectomy when unexpected multicentric disease was detected on CEDM or CEMRI; contralateral breast surgery due to cancer lesions detected on CEDM or CEMRI; excisional biopsy when CEDM or CEMRI detected an FP lesion in the ipsilateral or contralateral breast. For decision making in surgical management, each surgeon first reviewed the CEMRI results and subsequently planned the surgical strategy. They reviewed CEDM results later and, if the surgical plan was changed, these cases were categorized into “changed owing to findings detected on CEDM.” Identically, each surgeon first reviewed the CEDM results and planned the surgical strategy. They reviewed CEMRI results later and, if the surgical plan was changed, these cases were categorized into “changed owing to findings detected on CEMRI.” The final surgical strategy was based on the results of both CEDM and CEMRI.
Statistical analysis
Categorical data are summarized using frequencies and percentages. For detection of secondary cancers (multifocality and multicentricity) in the ipsilateral breast and occult cancer in the contralateral breast, the sensitivity, specificity, PPV, and negative predictive value (NPV) were evaluated using BI-RADS category ≥4 as suspicious assessments. However, only the sensitivity for index cancers were calculated because it was impossible to estimate specificity because there were no TN or FP lesions. The results were calculated with corresponding 95% confidence intervals for both imaging modalities and compared using McNemar's test. Statistical analyses were performed using PASW version 18.0 (IBM Corp., Armonk, USA); p<0.05 was considered to be statistically significant.
RESULTS
Patient characteristics
Eighty-four women with 84 index cancers were included in the analysis. The mean age at the time of enrollment was 50.9±9.1 years (range, 28–73 years). Thirteen of the 84 patients (15.5%) had a family history of breast cancer. Three patients (3.6%) had a personal history of breast cancer. Reasons for initial presentation included a palpable breast mass (n=28, 33.3%) and an abnormal screening mammogram or US (n=56, 66.7%). Fifty patients (59.5%) were premenopausal at diagnosis.
Histological findings
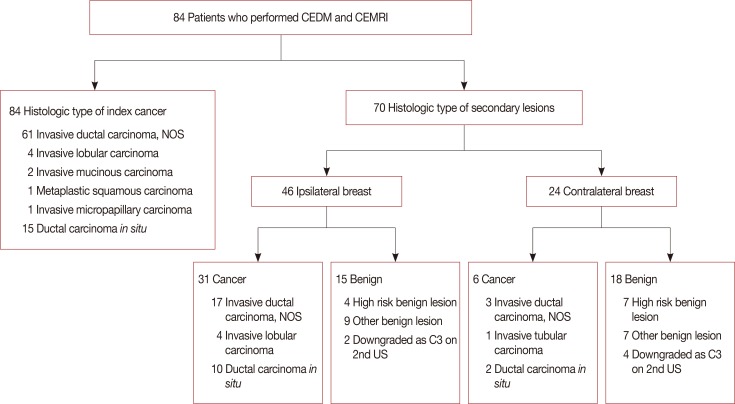
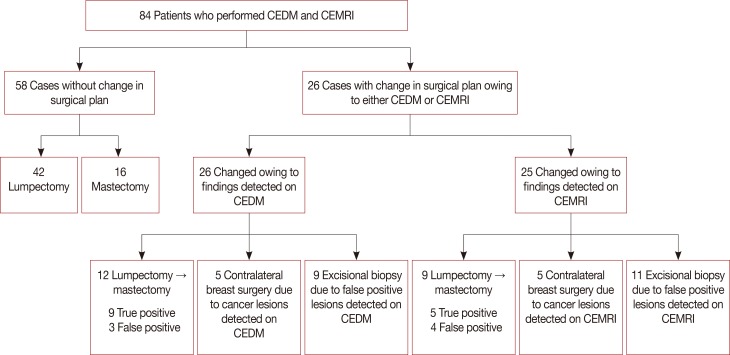
Histological findings for the index cancers and secondary lesions are summarized in the flow diagram presented in Figure 2. Of the 84 index cancers, the most common type was invasive ductal carcinoma (IDC), not otherwise specified (n=61, 72.6%), followed by DCIS (n=15, 17.9%). There were 70 secondary lesions detected using CEDM or CEMRI. Of the 70 lesions, 37 (52.9%) were malignant (multifocality, n=25; both multifocal and multicentric, n=6; occult cancer in the contralateral breast, n=6), and 33 lesions (47.8%) were benign. Fibrocystic change was the most common histological finding (13/33, 39.4%) among benign lesions.
Radiological and histopathological correlation
The correlation of CEDM and CEMRI final assessments with histopathological results are summarized in Table 1, which reports the TP, FP, TN, and FN results for CEDM and CEMRI.
True-positive findings
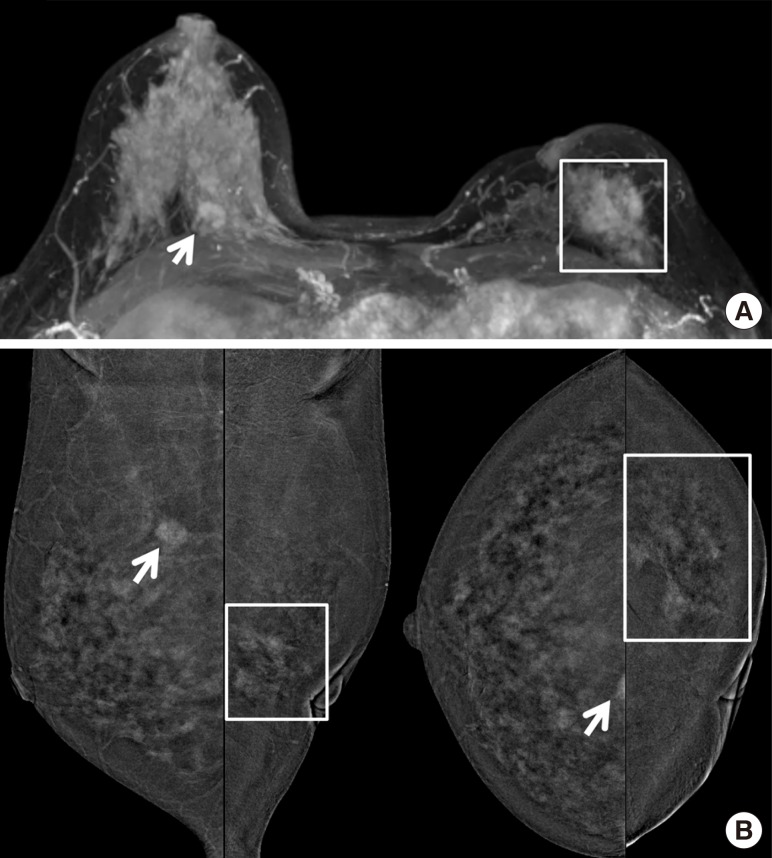
Compared with CEMRI, CEDM detected fewer index cancers (92.9% [78/84] vs. 95.2% [80/84], p=0.563) (Figure 3). For detection of secondary cancers in the ipsilateral breast (83.9% [26/31] vs. 83.9% [26/31], p=0.999) and occult cancer in the contralateral breast (83.3% [5/6] vs. 83.3% [5/6], p=0.999), both CEDM and CEMRI yielded identical results.
False-positive findings
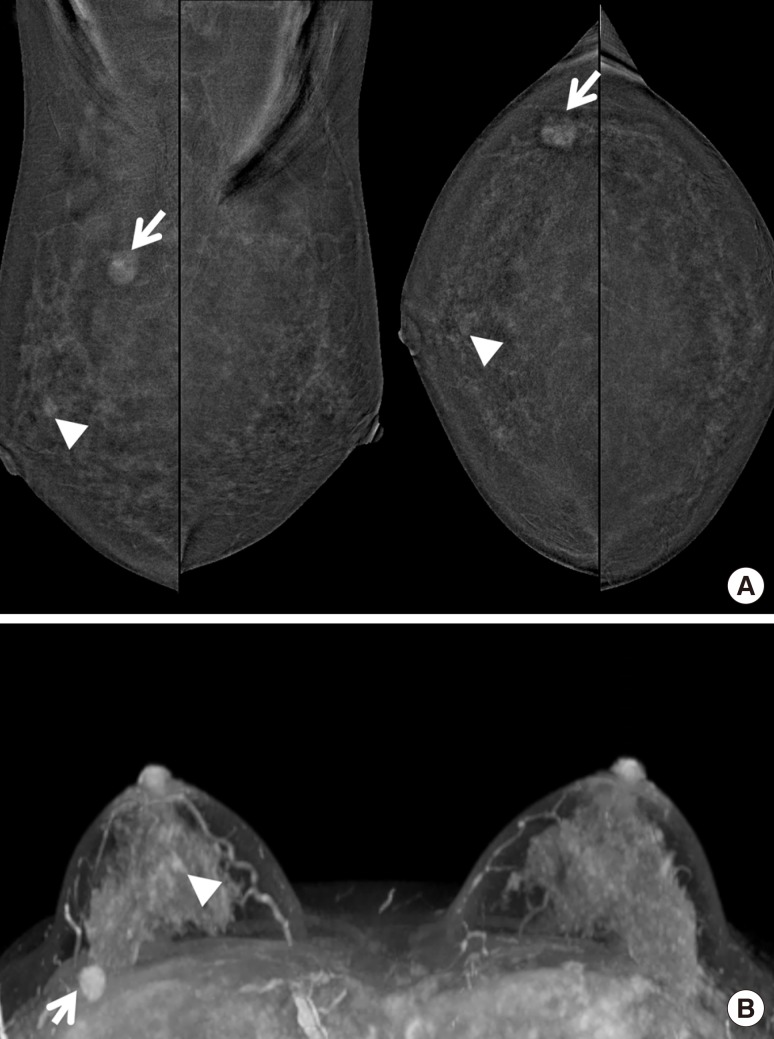
CEDM had fewer FP findings compared with CEMRI (66.7% [10/15] vs. 93.3% [14/15], p=0.843) in detecting cancers in the ipsilateral breast (Figure 4). Among the 10 FP lesions detected on CEDM, nine patients underwent surgical excision, and one had no suspicious findings (BI-RADS category 1–3) on second-look US. After surgical excision, three FP lesions were high-risk lesions. CEMRI detected 14 FP lesions in the ipsilateral breast, 12 patients underwent surgical excision, and two had no suspicious findings (BI-RADS category 1–3) on second-look US. After surgical excision, four FP lesions were high-risk.
True-negative findings
CEDM depicted a total of 15 TN lesions, eight of which were discordant with CEMRI. As an example, an enhancing lesion was suspicious on CEMRI, a finding that was corroborated with a second US, and CEDM confirmed it as a benign lesion.
False-negative findings
CEDM missed a total of six index cancers (6/84, 7.1%) and six secondary cancers (6/36, 16.7%) in the ipsilateral and contralateral breasts. Among the 12 missed lesions, nine of 12 (75%) were diagnosed as DCIS. Among the six missed index cancers, three lesions were detected on CEMRI instead, two lesions on US, and one lesion was detected on initial mammography.
CEMRI missed a total of four index cancers (4/84, 4.7%). First lesions were 1.2 cm and 0.8 cm multifocal IDCs, which were not enhanced on either CEMRI or CEDM. The second lesion was a 3.5-cm intermediate grade DCIS, which was first detected as a multifocal clustered microcalcification on initial mammography. The lesion was not enhanced on either CEMRI or CEDM. The third lesion was a multifocal invasive lobular carcinoma, which was described as BPE on CEMRI and a 7.0-cm enhancing lesion on CEDM. The final lesion was a 2.0-cm intermediate grade DCIS, which was first detected as a nodule accompanied by microcalcifications on both US and initial mammography. The lesion was not enhanced on either CEMRI or CEDM.
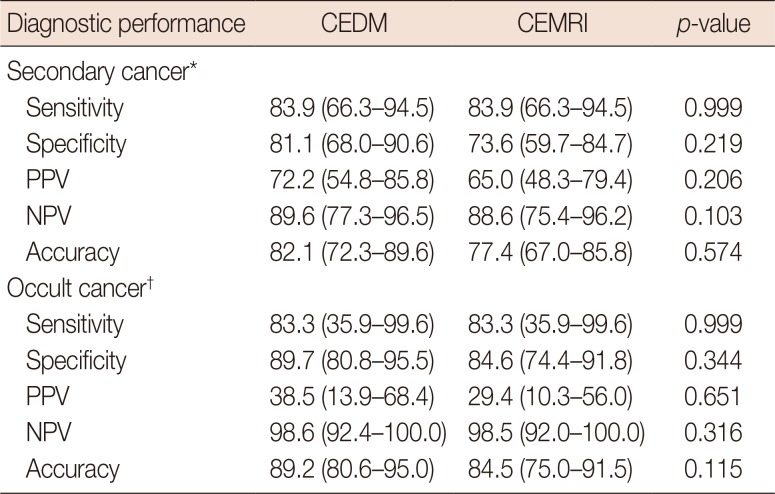
Diagnostic performance
The sensitivity, specificity, PPV, NPV, and accuracy of CEDM and CEMRI are reported in Table 2. For the detection of index cancer, CEDM had a similar sensitivity (92.9% [78/84] vs. 95.2% [80/84], p=0.563). For the detection of secondary cancers in the ipsilateral breast, CEDM had identical sensitivity (83.9% [26/31] vs. 83.9% [26/31]) and higher specificity (81.1% [43/53] vs. 73.6% [39/53]) than CEMRI, without a statistically significant difference (p=0.999 and p=0.219, respectively).
Conversion of surgery
A flow diagram of surgical management based on CEDM or CEMRI is shown in Figure 5. Among the 84 patients, 26 had a change in their surgical management. CEDM resulted in similar changes in surgical management compared with CEMRI (30.9% [26/84] vs. 29.7% [25/84], p=0.610). Regarding changes in surgical management due to FP findings, no significant differences were found between CEDM and CEMRI (34.6% [9/26] vs. 44.0% [11/25], p=0.782).
DISCUSSION
CEDM depicts angiogenesis of breast cancer by tracking the uptake of iodine-based contrast agent in breast tissues, similar to CEMRI, which detects angiogenesis by uptake of gadolinium contrast agent in breast tissues. CEDM offers many advantages compared with CEMRI, such as a shorter procedure time, low cost, no need to schedule according to menstrual cycle, and no risk for claustrophobia [19]. CEDM also demonstrated diagnostic performance comparable with CEMRI for detecting index breast cancer, estimating tumor extent and finding multifocal cancers.
Because CEDM has only been recently introduced for diagnostic use, few studies have compared CEDM with CEMRI in terms of diagnostic utility. Previous investigations have reported comparable diagnostic performance of CEDM and CEMRI in detecting breast index cancer, estimating tumor extent and finding multifocal cancers. A study by Lee-Felker et al. [9] reported that CEDM and CEMRI detected 94% and 99% of index cancers, respectively, which is similar to our detection rate of 92%–95%.
Both CEDM and CEMRI can enhance and detect occult cancer due to tumor angiogenesis [7]. Both imaging modalities are based on the increase in enhancement in malignant lesions after intravenous contrast agent administration due to the presence of more and larger vessels with higher permeability to the vascular space [20]. However, neo-angiogenesis varies according to the type of malignancy. It is more pronounced in IDC, and is not always present in DCIS and lobular carcinomas [21]. Therefore, the additional benefit of CEDM and CEMRI in detecting DCIS or suspicious microcalcifications remains unclear. There are only a few studies that have reported the enhancement of DCIS on CEDM or CEMRI [22]. Consistent with previous studies, most of our FN lesions were also DCIS and ILC. In our study, CEDM missed a total of six index cancers (6/84, 7.1%) and six secondary cancers (6/37, 16.2%) in the ipsilateral and contralateral breast. Among the 12 missed lesions, nine of 12 (75%) were DCIS, and none (0/12, 0%) were ILC. CEMRI missed a total of four index cancers (4/84, 4.8%) and six secondary cancers (6/37, 16.2%) in the ipsilateral and contralateral breast. Among the 10 missed lesions, five of 10 (50%) were DCIS, and two of 10 (20%) were ILC.
Regarding diagnostic performance, Jochelson et al. [23] found that CEDM had a lower sensitivity for depicting secondary cancers in the ipsilateral breast than CEMRI (56% vs. 88%), but with a higher PPV (97% vs. 85%, p<0.01). In our study, CEDM resulted in a higher PPV for secondary (72.2% vs. 65.0%) cancers in the ipsilateral breast than CEMRI, with fewer FP findings (10/15 [66.7%] vs. 14/15 [93.3%]) in the ipsilateral breast. The cause of high FP findings on CEMRI is due to high-risk lesions. Nadler et al. [24] reported that the FP rate of high-risk lesions (including LCIS, ADH, and ALH) on CEMRI was 19%. This high FP rate on CEMRI leads to a lower specificity compared with CEDM in detecting secondary cancers, which may affect decisions regarding surgical management.
Decision making regarding the surgical extent of breast cancers depends on various factors, including disease extent within the affected breast and patient preferences. Mammography, US, and CEMRI are used to identify additional cancer foci and determine tumor extent. Although CEMRI has advantages in finding multifocal lesions, it also has disadvantages including high cost and time-consuming procedure prone to more FP findings. FP findings lead to an increased number of biopsies and conversion from BCS to mastectomy [25]. In our study, CEDM demonstrated similar changes in surgical management due to FP findings compared with CEMRI (34.6% [9/26] vs. 44.0% [11/25], p=0.782). Based on this result, CEDM can be as useful a tool as CEMRI for surgical planning purposes. Results from more evidenced-based studies are, nevertheless, needed.
BPE is caused by enhancement of normal breast tissue after intravenous contrast material administration [26]. The degree of BPE is related to the vascular supply and permeability of the breast parenchyma [27]. There is debate, however, as to whether BPE negatively affects the sensitivity and specificity of CEMRI interpretation by obscuring enhancing malignancies [28]. There have been a few studies assessing the extent of BPE on CEDM and CEMRI. Sogani et al. [29] reported that a similar proportion of patients had minimal or mild BPE on CEDM (68%–76%) and CEMRI (69%–76%). In this study, we also found that most patients had minimal or mild BPE on CEDM (57/84, 67.9%) and CEMRI (58/84, 69.0%) (p>0.05). This result indicates that the degree of BPE was not significantly different between CEDM and CEMRI. Because BPE is dependent on hormone levels, which vary according to menopausal status and phase of the menstrual cycle in premenopausal women [27], some have proposed performing CEDM and CEMRI according to menstrual phases. However, others have found no clear pattern in the variation of BPE across the different phases of the menstrual cycle on either CEDM or CEMRI [29]. They also suggest that menstrual cycle timing may not need to be considered when scheduling examinations for evaluating BPE. In our study, CEDM was performed within 7 days of CEMRI. Based on a previous study, the effect of time interval (7 days) between two examinations can be minimal for evaluating BPE.
Our study had several limitations, the first of which was the small number of subjects in the study population. Second, we categorized a total of seven lesions as benign based on second-look breast US results (BI-RADS category 1–3) and did not perform a biopsy. Only imaging follow-up was performed on the seven lesions, and there was no lesion that was upgraded to a suspicious lesion (BI-RADS category ≥4) until the 1-year follow-up. Finally, in addition to IDC patients, we also enrolled DCIS and ILC patients. Most of our FN results from CEDM were DCIS (9/26) or ILC (0/8). To validate the sensitivity of CEDM in detecting DCIS (17/26) or ILC (8/8), further investigation is needed.
Our investigation, however, also had several strengths. This study was the first CEDM study conducted in South Korea. Second, CEDM was safe and technically feasible. The type of contrast medium (i.e., iodinated), the dosage, and the speed of injection were identical to those used in computed tomography (CT) protocols. This implies that CEDM confers the same degree of safety and hazard as CT, with significantly greater benefit. It is also inexpensive, less time consuming, offers easy interpretation of images, and has similar diagnostic accuracy compared with CEMRI. In our study, there was only one patient who experienced side effects from CEDM, and no technical failures occurred from CEDM. The patient experienced nausea and vomiting 1 minute after injection of contrast media; however, the symptoms subsided gradually after injecting dexamethasone and pheniramine. Moreover, the radiation dose was estimated to be only 1.2 times that of a regular mammogram [30]. The radiation dose for CEDM (sum of high- and low-energy image dose) for a woman with average breast size (equivalent to 4.2-cm compressed breast thickness with 50% fat and 50% glandular composition) is <3.0 mGy [12]. Finally, CEDM provides an easy and simple method for the surgeon and clinician to interpret images without having to know the many complicated parameters of CEMRI.
In conclusion, CEDM yielded diagnostic results comparable with CEMRI in depicting index cancers, secondary cancers, and occult cancer in the contralateral breast. Owing to fewer FP results, CEDM resulted in fewer changes to surgical management compared with CEMRI, and the degree of BPE was not significantly different between CEDM and CEMRI.

 XML Download
XML Download