

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neoadjuvant chemotherapy (NAC) is being increasingly used for patients with operable breast cancer to allow for more minimal surgery [1]. Moreover, NAC has been shown to effectively downstage axillary lymph nodes (ALNs) [2]. To avoid complications associated with ALN dissection (ALND), it is preferable to identify nodal disease with a less invasive sentinel lymph node (SLN) surgical procedure, which results in less morbidity [3].
Because identification of the SLNs could be interrupted by blocked lymph passages, there is a risk of a high false negative rate (FNR) of SLN biopsy (SLNB) [4]. There have been several studies examining whether SLNB can precisely predict ALN metastasis after NAC in breast cancer patients with cytology proven node metastasis. Recently, a study reported a SLN identification rate of 89.6% and a FNR of 14.2% after NAC [5].
Although about 30% of patients had pathologic complete response (pCR) in the axilla after NAC, ALND has been suggested for breast cancer patients with biopsy-determined node metastasis breast cancer regardless of response to NAC treatment [67]. Some evidence has suggested that the nodal stage after NAC reflects the prognosis more accurately than the initial axillary status [8]. Therefore, removal of lymph nodes during ALND may not be needed for patients with a complete response (CR). Specifically, there have been several studies of SLNB feasibility in clinical ALN metastasis but not in cytology-determined axillary node metastasis [3910]. In our study, we evaluated the feasibility of SLNB in cytology-determined node-positive breast cancer and evaluated disease-free survival (DFS) and overall survival (OS) in patients who underwent SLNB alone versus those who underwent SLNB with ALND.
Go to : 
METHODS
This study is a registered medical record review based on a prospectively collected database. We evaluated 506 patients who were diagnosed with invasive breast cancer and ALN metastasis by ultrasound of the axilla and have undergone surgical treatment after NAC treatment at Samsung Medical Center between January 2007 and December 2014. Inclusion criteria were as follows: (1) diagnosis of enlarged ALN by breast ultrasonography and by fine needle aspiration cytology upon initial examination, (2) presence of cytology-determined, positive ALN status, (3) completion of the planned-regimen NAC, and (4) completion of excision of a breast cancer and SLNB or ALND. Exclusion criteria were as follows: (1) presence of bilateral breast cancer, (2) inflammatory breast cancer, (3) previous ipsilateral axillary surgery, and (4) distant metastasis.
Radiotherapy was administered in all patients treated by breast-conserving surgery and in some patients treated by total mastectomy. Most patients (95.1%) received NAC with anthracycline- or taxane-based regimens. These regimens included anthracycline plus cyclophosphamide, followed by anthracycline-based, taxane-based, or trastuzumab regimens. Clinical response to treatment was evaluated by breast ultrasonography and breast magnetic resonance imaging (MRI). Clinical CR was explained as disappearance of residual tumor on breast ultrasonography or breast MRI.
Sentinel node biopsy was performed with technetium-99m sulfur-colloid diluted in normal saline solution and/or vital blue dye (0.8% indigo carmine). The site and timing of agent administration were at the physician's discretion. Radiolabeled colloid was injected 2 to 6 hours before surgery and/or 5 mL of 0.8% indigo carmine was injected periareolarly and the breast was massaged for 5 minutes. For the sulfur-colloid injection, a handheld gamma detection probe was used to scan the axilla transcutaneously and identify the most radioactive area. All radioactive and/or blue lymph nodes and palpable lymph nodes were excised and submitted as SLNs. The clinical CR of the breast was defined as a disappearance of all of the tumor deposits on MRI scan or on breast ultrasonogram. The quantification of response by using the categories of CR, partial response, stable disease/progressive disease served as a gross estimate of tumor chemosensitivity.
We sectioned the removed SLNs transversely into 24 sections. After pathological evaluation of the sections, we fixed the tissue with 10% formalin and embedded it in paraffin; the embedded tissue was processed further to prepare hematoxylin and eosin (H&E)-stained sections. We designated metastatic foci of 0.2 to 2 mm as micrometastases, and metastatic clusters smaller than 0.2 mm as isolated tumor cells, whether detected by H&E or by immunohistochemistry. We used anti-estrogen receptor and anti-progesterone receptor monoclonal antibodies to perform immunohistochemical staining of the formalin-fixed paraffin-embedded tissue. Only nuclear staining was scored. A positive test was defined as positive staining of greater than or equal to 1% of tumor cells, while a negative test was defined as staining of less than 1% of tumor cells. We also performed immunohistochemical staining of the formalin-fixed paraffin-embedded tissue using anti-human epidermal growth factor receptor 2 (HER2) monoclonal antibodies. A positive test was defined as staining with a score of 3+. A score of 2+ was interpreted as equivocal. A negative test was defined as staining with a score of 0/1+.
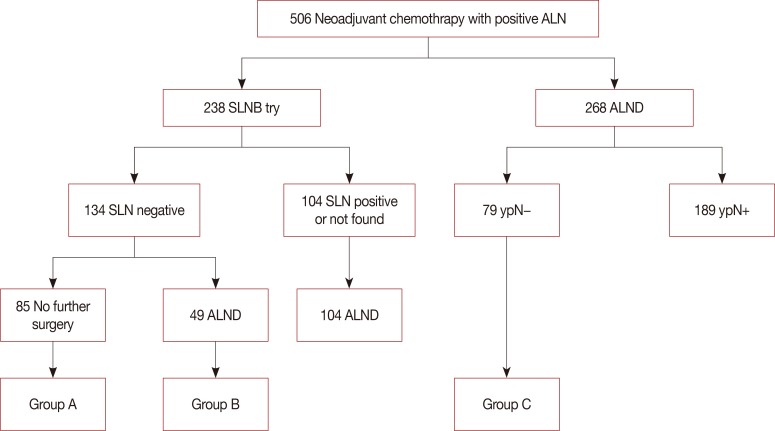
Three of five breast surgeons at our center have started trying SLNB procedures since 2011 in breast cancer patients under NAC treatment, except in cases of disease progression in follow-up breast MRI or breast ultrasonography. Among patients with negative SLN, patients with suspicious enlarged nodes at the time of surgery underwent further ALND. We classified patients into three groups: group A, negative SLN metastasis and no further dissection; group B, negative SLN metastasis however further ALND; and group C, axillary CR with ALND regardless of clinical response (Figure 1). We collected oncological data on axillary recurrence, distant metastasis, and survival outcome. We evaluated and compared oncology outcomes among all groups.
We were aided by the statistical team at the Samsung Medical Center. We categorized patients in whom SLNs were identified as true positive (TP) or false negative (FN). The FNR was calculated as follows: FN/(FN+TP)×100%. The independent t-test was used to compare continuous variables, and the chi-square test and the Fisher exact test were used to compare discrete variables. We used the Kaplan-Meier method with the log-rank test to construct survival curves. Differences were assumed to be significant when the p-value was less than 0.05. All statistical analyses, including the logistic regression and the chi-square tests were performed using the IBM SPSS Statistics for Window, version 23 software (IBM Corp., Armonk, USA). This study was approved by the Institutional Review Board of Samsung Medical Center, Seoul, Korea (IRB file no. 2017-09-051).
Go to :
RESULTS
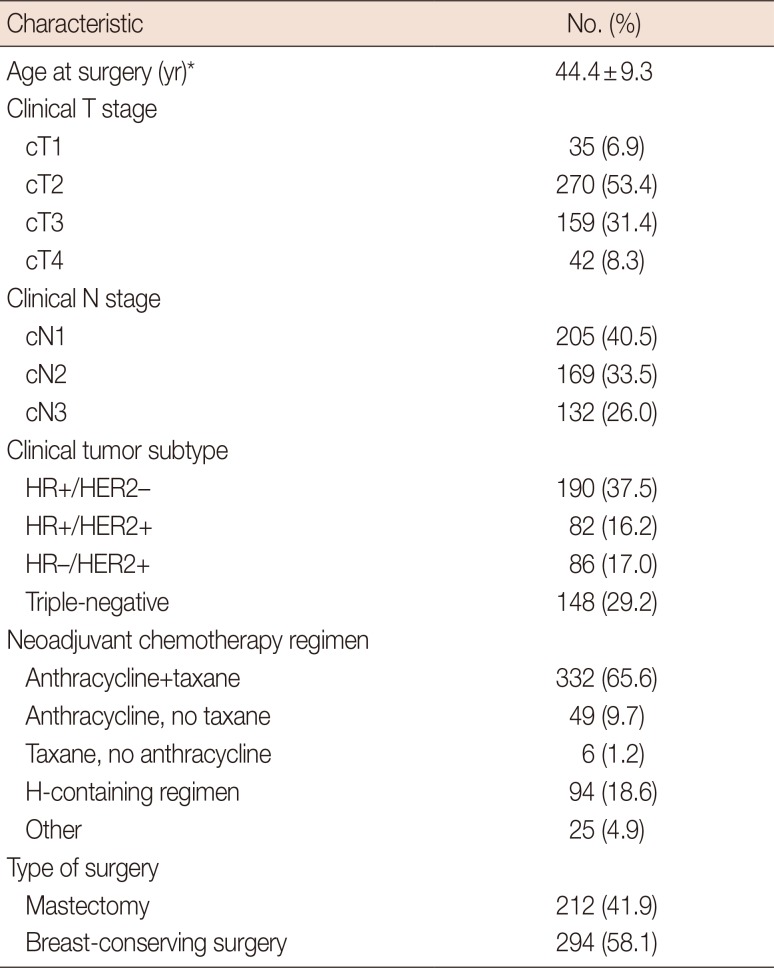
In this study, we included 506 breast cancer patients with cytology proven node metastasis who underwent NAC treatment followed by curative surgery. The mean age at surgery was 44.4±9.3 years. The median follow-up time was 51 months (range, 3–122 months). Of these patients, 134 were SLN metastasis-negative on frozen SLNB. Eighty-five patients with negative SLNs metastasis had no further surgery (group A), while 49 patients with negative SLN metastasis had backup ALND (group B). One hundred and four patients with positive SLN metastasis or undetected SLNs by the radioactive and/or vital blue method had further ALND. Of the patients who did not undergo SLNB, 79 had ALND with no residual axillary metastasis (group C), and 189 patients with pathological node-positive disease underwent ALND (Figure 1).
The clinicopathological and treatment characteristics of patients included in this study are showed in Table 1. Regarding the breast cancer subtype, 37.5% of patients had hormone receptor (HR)-positive/HER2-negative breast cancer, 16.2% had HR-positive/HER2-positive breast cancer, 17.0% had HR-negative/HER2-positive breast cancer, and 29.2% had triple-negative breast cancer (TNBC). For NAC, 65.6% of the patients received anthracycline- and taxane-based regimens and 18.6% of the patients received trastuzumab-containing regimen. Clinical nodal stage data showed an incidence of 40.5% for clinical N1 stage, 33.5% for clinical N2 stage, and 26.0% for clinical N3 stage. Clinical tumor stage data showed an incidence of 6.9% for clinical T1 stage, 53.4% for clinical T2 stage, 31.4% for clinical T3 stage, and 8.3% for clinical T4 stage.
The SLN identification rate was 98.3% (234/238 patients). The median number of retrieved SLNs was 5 (range, 2–9), and 104 of the 238 patients who underwent SLNB had positive SLNs. The FNR of SLNB after NAC was 7.5% (8/106 patients).
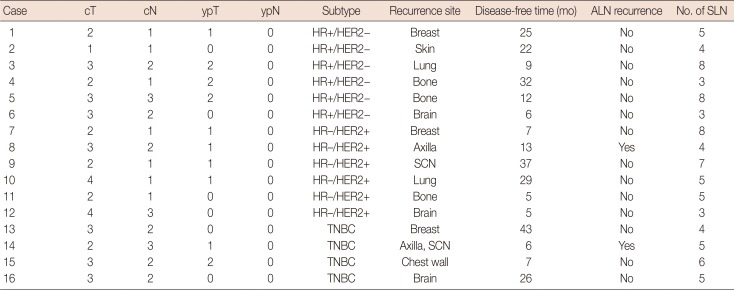
The characteristics of the SLN biopsy group and pathological node negative ALND group are shown in Table 2. Group C showed a higher mastectomy rate (p=0.001), clinical tumor stage (p=0.001), clinical node stage (p=0.022), and pathol-ogic nodal stage (p<0.001) than did groups A and B. However there was no significant difference in age, clinical tumor subtype, chemotherapy regimen, pathologic tumor stage, clinical response after NAC and lymphovascular invasion among the three groups. Sixteen of the 85 patients in the SLNB alone group (group A) experienced recurrences. Six patients were pathologic T0 stage, six were pathologic T1 stage, and four were pathologic T2 stage. Six patients were HR-positive/HER2-negative, six were HR-negative/HER2-positive, and four had TNBC. Systemic metastasis occurred in the bone, lungs, and brain in eight patients, and axillary metastasis occurred in two patients (Table 3).
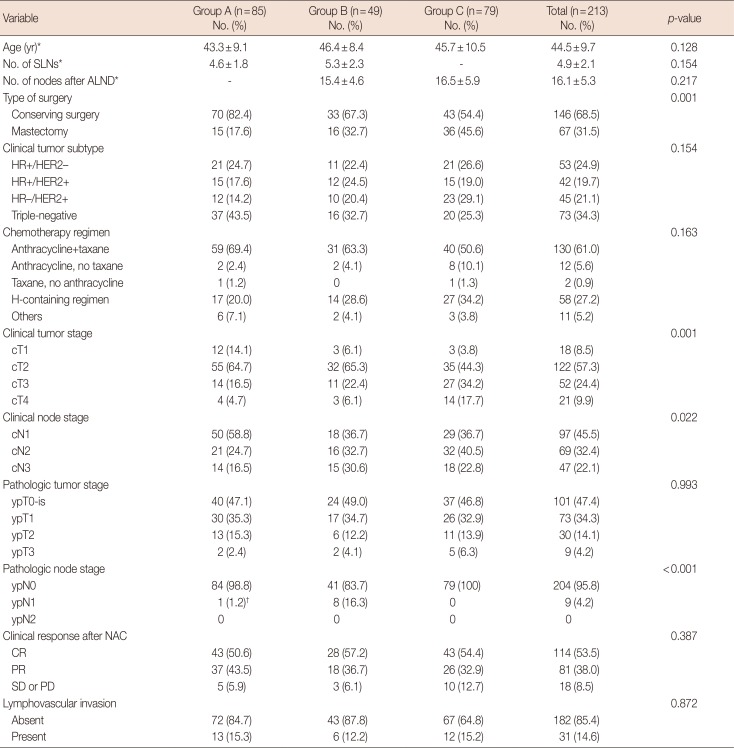
Table 2
Characteristics of the sentinel lymph node biopsy-negative group and pathologic node-negative ALND group
ALND=axillary lymph node dissection; SLN=sentinel lymph node; HR=hormone receptor; HER2=human epidermal growth factor receptor 2; H=trastuzumab; NAC=neoadjuvant chemotherapy; CR=complete response; PR=partial response; SD=stable disease; PD=progressive disease.
*Mean±SD; †Negative in frozen biopsy but microinvasive in permanent biopsy.
![]()
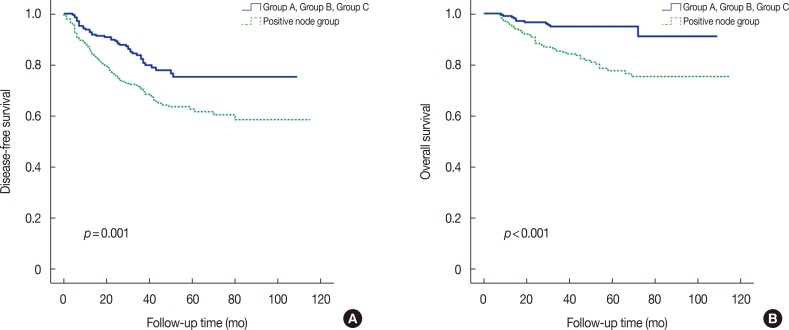
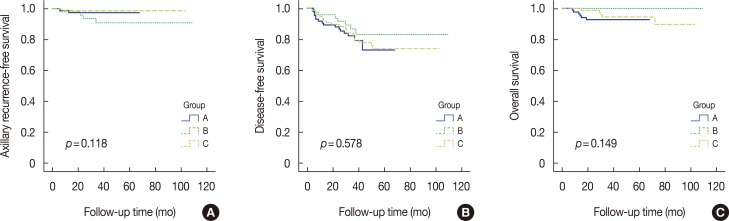
We compared survival outcomes between the node-negative group (combined groups A, B, and C) and the node-positive group. There was a significant difference in DFS and in OS between the node-negative (combined groups A–C) and the node-positive groups (5-year DFS: 78.3% vs. 62.7%, p=0.001; 5-year OS: 94.9% vs. 77.8%, p<0.001) (Figure 2). Figure 3 compares the survival outcomes in groups A, B, and C. Axillary recurrence-free survival was not significantly different among groups (5-year axillary recurrence-free survival: group A, 97.4% vs. group B, 90.9% vs. group C, 98.7%, p=0.118). There was also no difference among groups A, B, and C in DFS (81.2% vs. 85.7% vs. 77.2%, p=0.578) or in OS (92.9% vs. 100% vs. 93.7%, p=0.149).
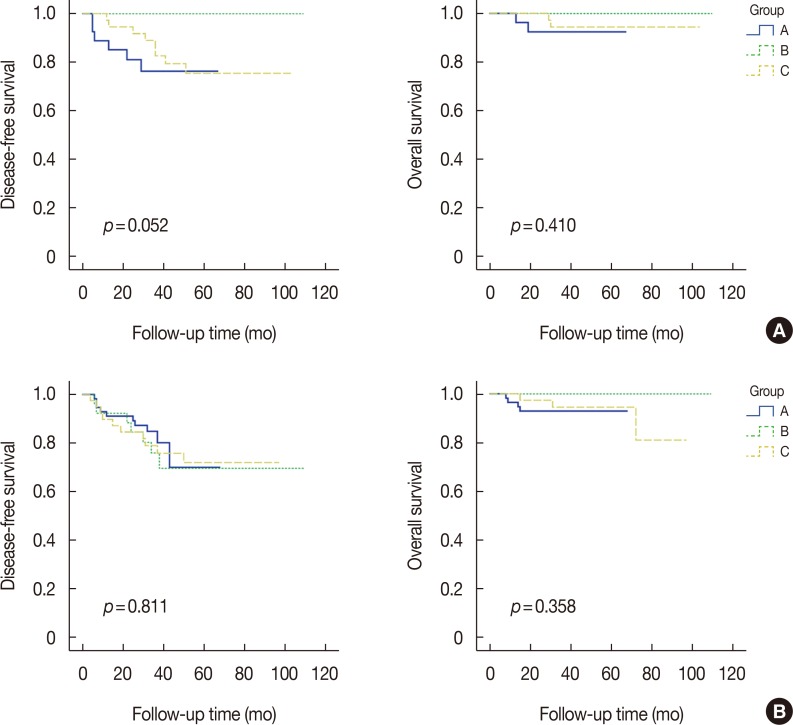
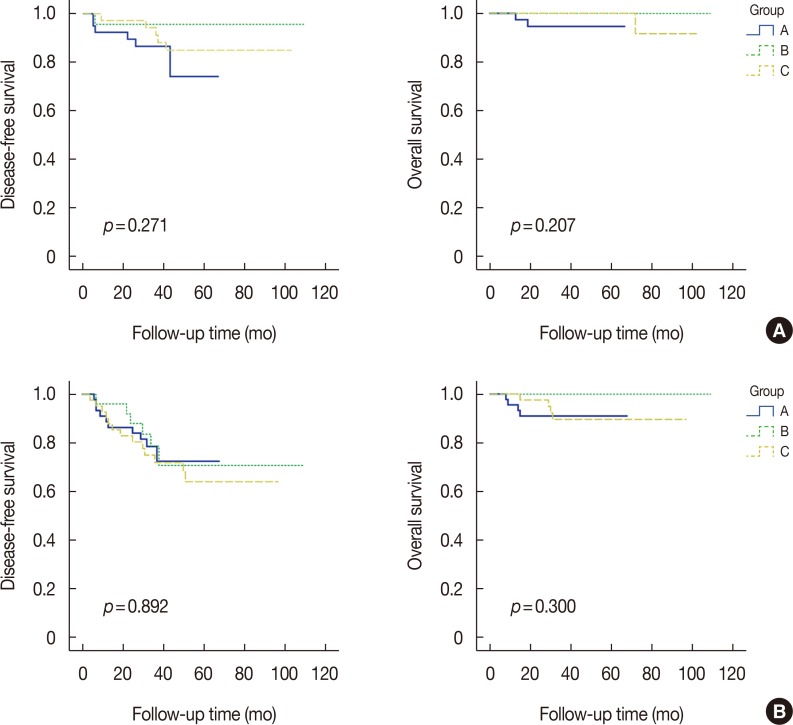
In the subgroup analysis by HR status, there was no significant difference in DFS (p=0.767) or OS (p=0.428) among groups A, B, and C in the HR-positive subgroup. There was also no difference in DFS (p=0.581) or OS (p=0.333) in the HR-negative subgroup (Figure 4). Similarly, there was no significant difference in DFS (p=0.052) or OS (p=0.410) among groups A, B, and C in the HER2-positive subgroup and no significant difference in DFS (p=0.811) or OS (p=0.358) in the HER2-negative subgroup (Figure 5). In the subgroup analysis of breast pCR status, there was no significant difference in DFS (85.0% vs. 95.8% vs. 86.5%, p=0.271) or OS (95.0% vs. 100% vs. 97.3%, p=0.207) among groups A, B, and C in the breast pCR subgroup and no significant difference in DFS (77.8% vs. 76.0% vs. 69.0%, p=0.892) or OS (91.1% vs. 100% vs. 90.5%, p=0.300) in the breast non-pCR subgroup (Figure 6).
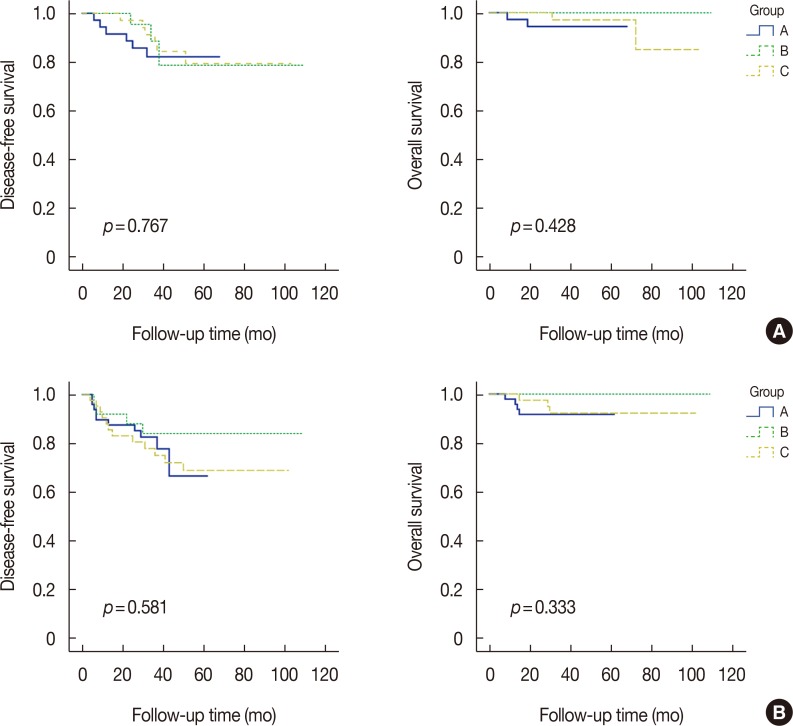 | Figure 4Kaplan-Meier curves for disease-free survival and overall survival among groups A, B, and C in hormone receptor (HR)-positive (A) and HR-negative (B) patients.
|
Go to :
DISCUSSION
Several studies have been published on the effectiveness and role of SLNB after NAC. The results of these studies showed that SLNB with NAC may be feasible and acceptable option [11121314]. ALN metastases can be extirpated by NAC in some patients, and consequently, ALND may be avoided in these. However, SLNB after NAC might not be accurate because anatomical alterations of the lymphatic drainage by chemotherapy can destroy lymphatic vessels or lymphatic channels due to inflammation or fibrosis. Previous studies showed that for patients with clinically positive nodes, the identification rate for the SLNB after NAC is 89.0% to 98.0% [9101516]. Our study showed an identification rate of 98.3% for SLNB, which falls within the published range [17]. Because this study defined suspicious palpable lymph nodes as SLNs, the high SLN number could have affected the identification rate. We have previously studied the feasibility and prognostic effect of SLNB after NAC [4]. However, the median follow-up time was as short at 37 months, and only 329 patients were surveyed. Therefore a study with a longer follow-up and a larger sample size was needed.
In several studies, the FNR of SLNB was 14% in node-positive patients treated with NAC. This was more than about 4% FNR of SLNB for node-negative patients who did not receive NAC treatment [1819]. Also, this study did not use targeted axillary dissection (TAD), which ensures resection of the clipped lymph node at the time of SLNB. TAD could potentially lead to an even lower FNR of 4.2% and allow for a more precise way of performing SLNB [20]. We did not use TAD at SLNB after NAC, however, in our study, the median number of retrieved SLNs was five and the overall FNR was 7.5%. The overall FNR of this study was a rate less than the pre-specified rate of ≤10%, although we performed SLNB in breast cancer patients with cytologically-determined node metastasis.
Many studies have demonstrated the use of SLNB with NAC in breast cancer patients with node metastasis [32122]. In our study, the patient population included biopsy-determined, node metastasis patients. In contrast, in the Sentinel Neoadjuvant (SENTINA) study, the node metastasis was clinically diagnosed; in that study, the diagnosis of 592 patients with clinically node-metastasis cancer was changed to negative SLN after NAC, with a 14.2% FNR. The overall FNR was 12.6% for the American College of Surgeons Oncology Group (ACOSOG) Z1071 trial and 8.4% for the Sentinel Node Biopsy Following Neoadjuvant Chemotherapy in Biopsy Proven Node-Positive Breast Cancer (SN-FNAC) trial. However, the FNR was 7.3% in the SENTINA trial and 9.1% in the ACOSOG Z1071 trial when three or more SLNs were retrieved. Similarly, in this study, the FNR was 7.5% and the median number of removed SLNs was five.
A recent study showed no statistical difference in DFS among subgroups according to HR status [15]. Similarly, we also found that the OS and DFS rates did not differ significantly between subgroups according to HR, HER2, or pCR status. Furthermore, our study included a longer follow-up than the previous studies. A meta-analysis suggested that more than 20% of patients treated with breast surgery would develop lymphedema [2324]. Lymphedema following breast cancer treatment can be an irreversible condition with negative effects on quality of life. The data from several studies have shown that patients with NAC treatment had more lymphedema [24]. In our study, lymphedema and arm motion morbidity were observed in 7.1% (6/85) of the SLNB-alone group and in 27.3% (35/128) of the ALND group. Radiation therapy was administered to 82.4% (70/84) in the SLNB-alone group and to 80.5% (103/128) in the ALND group. Therefore, SLNB may be associated with less lymphedema and arm motion morbidity than is ALND after NAC.
Although this study was performed in a single comprehensive cancer institution in Korea and the number of patients was relatively small, it did not investigate clinically suspected node-positive patients but instead investigated node-positive patients confirmed by cytology. Therefore, the results obtained from the analysis of the small sample population are still meaningful. Additionally, this study was not a prospective randomized clinical trial; group C was higher than group A and B in clinical tumor stage and node stage. Thus, the distribution of patients may have had some effect on the results of regional control. Also, we began performing SLNB alone after NAC since 2011, so the median follow-up period for group A was less than that for group B and group C. The longest follow-up time was 73 months in group A and 113 months in group B. However, this study had a median follow-up time of 51 months, and the results reveal clinical effect and provide important insights regarding feasibility of SLNB after NAC.
In conclusion, our study of breast cancer patients who had ALN conversion from cytology-determined positive to negative following NAC indicated that SLNB and ALND without SLNB had similar rates of axillary recurrence, DFS and OS. Therefore, SLNB may be acceptable after NAC for patients with cytology-determined, node-metastasis-positive breast cancer with a reasonable identification rate. Also, in some patients, SLNB can help identify possible downstaging to a negative nodal stage, and since ALND is avoided, this may reduce arm motion morbidity and lymphedema. We suggest the use of SLN surgery as an alternative to ALND after NAC in patients with cytology-determined axillary node metastasis-positive breast cancer.
Go to :
 XML Download
XML Download