

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
METHODS
Study population and clinicopathologic data
Immunohistochemistry and molecular tests
Statistical analysis
RESULTS
Patient clinicopathologic characteristics according to PIK3CA mutation status
Table 1
Clinicopathologic parameters according to PIK3CA mutation status
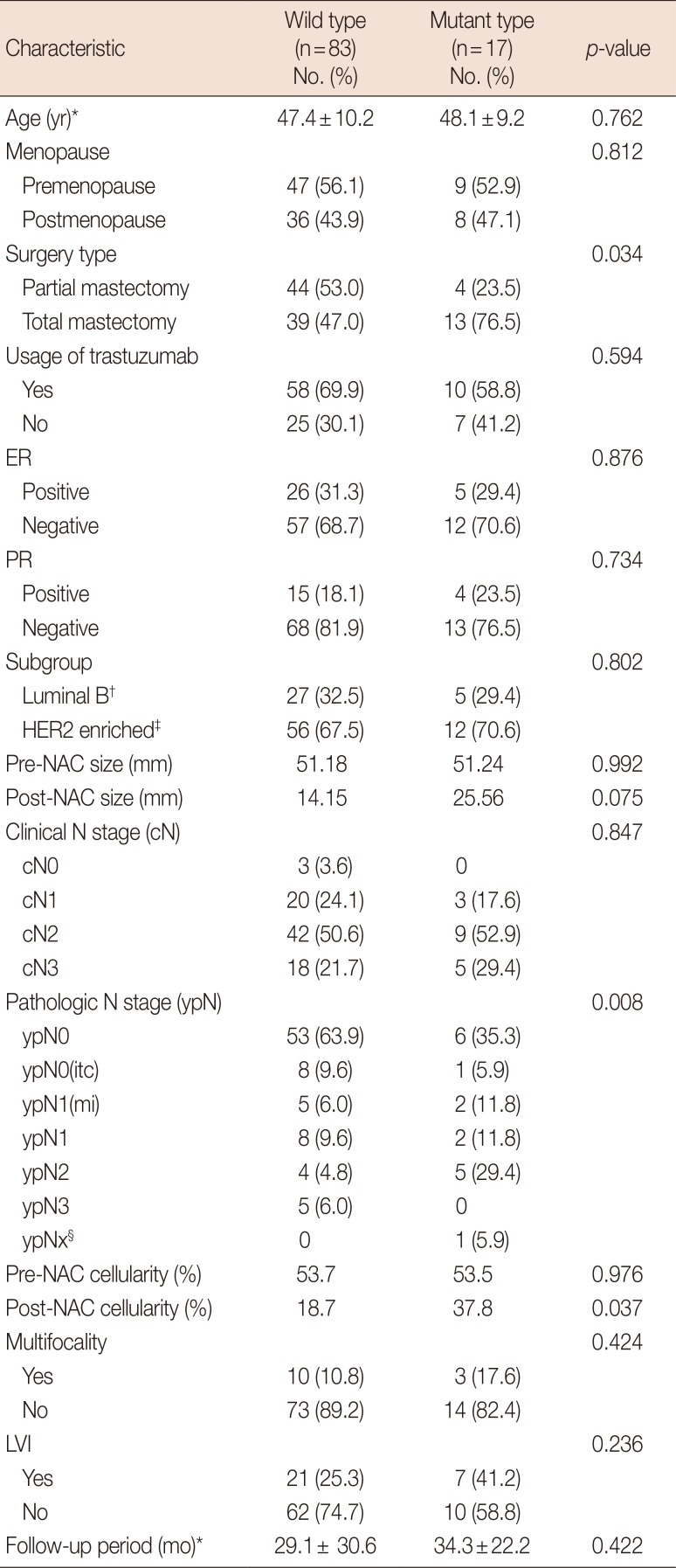
ER=estrogen receptor; PR=progesterone receptor; HER2=human epidermal growth factor receptor 2; NAC=neoadjuvant chemotherapy; itc=isolated tumor cells; mi=microinvasion; LVI=lymphovascular invasion.
*Mean±SD; †Luminal B: immunonistochemical stain for estrogen receptor or progesterone receptor (+); ‡HER2 enriched: immunonistochemical stain for estrogen receptor and progesterone receptor (−); §The one of the ypNx case did not undergo node dissection.
![]()
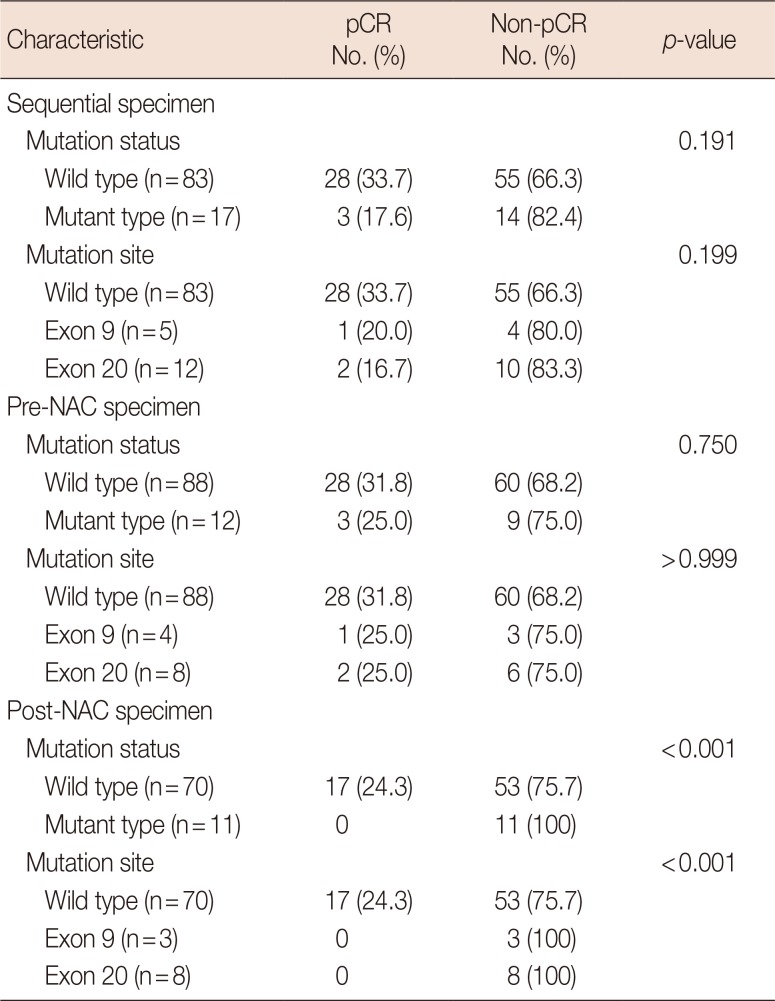
Pathologic response with neoadjuvant chemotherapy and PIK3CA mutation status in sequential specimens
Survival analysis
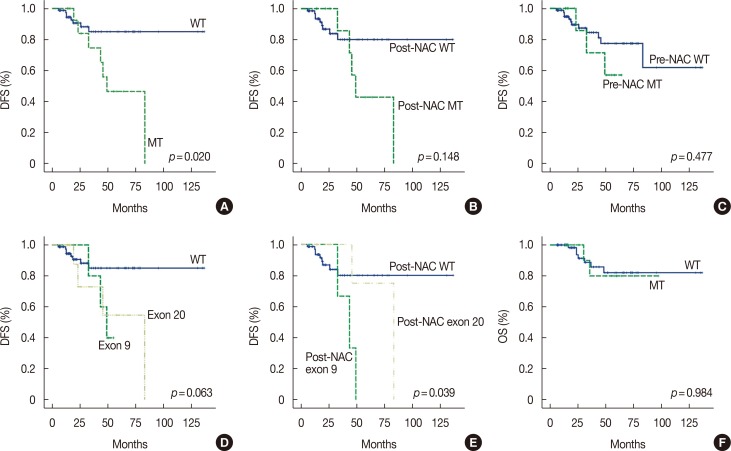
Figure 1
Survival curves for disease-free survival (DFS) and overall survival (OS). (A) PIK3CA mutant group (MT) in any sequential specimen had a shorter median DFS than the purely wild-type group (WT) in sequential specimens (58.3 months vs. 119.3 months, p=0.020). (B) In post-neoadjuvant chemotherapy (NAC) specimens, MT showed a shorter median DFS tendency than WT (60.2 months vs. 113.5 months, p=0.148). (C) Median DFS was not significantly different in pre-NAC WT and pre-NAC MT (51.8 months vs. 103.9 months, p=0.477). (D) There was no difference in median DFS depending on mutation site in sequential analysis (119.3 months vs. 47.2 months vs. 59.8 months, p=0.063). (E) Mutation site was associated with different median DFS in post-NAC specimens (post-NAC WT: 113.5 months vs. post-NAC exon 9: 41.8 months vs. post-NAC exon 20: 74.0 months, p=0.039). In subgroup analysis, post-NAC exon 9 mutation was found to have significantly shorter DFS than other groups (vs. post-NAC WT: p=0.017 vs. post-NAC exon 20: p=0.048). (F) OS was not correlated with PIK3CA mutation status (84.5 months vs. 118.0 months, p=0.984).
![]()
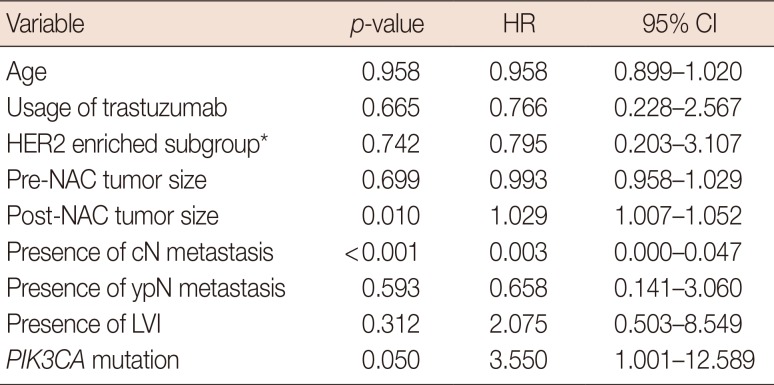
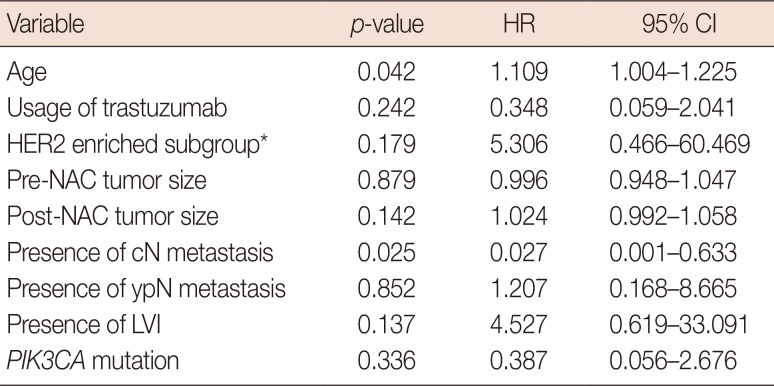
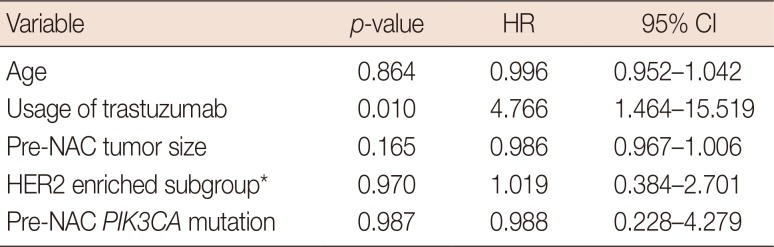
Prognostic or predictive effectiveness of PIK3CA mutation
Change of PIK3CA mutation status in sequential specimens
Table 6
Clinicopathologic characteristics of cases with mutation change in sequential analysis
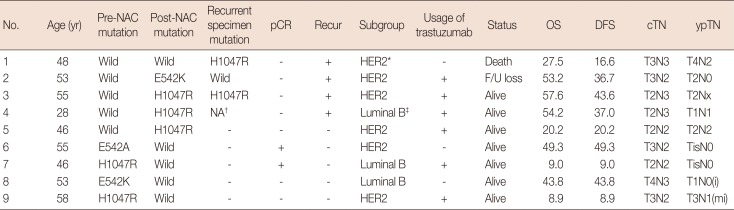
NAC=neoadjuvant chemotherapy; pCR=pathologic complete response; OS=overall survival; DFS=disease-free survival; cTN=clinical T&N stage; ypTN=post-NAC pathological T&N stage; HER2=human epidermal growth factor receptor 2; F/U=follow-up; i=isolated tumor cell; mi=microinvasion.
*HER2 enriched: immunonistochemical stain for estrogen receptor and progesterone receptor (−); †NA: multiple distant metastases were found in the brain in this case, but further tests could not be performed because no samples were obtained; ‡Luminal B: immunonistochemical stain for estrogen receptor or progesterone receptor (+).
![]()
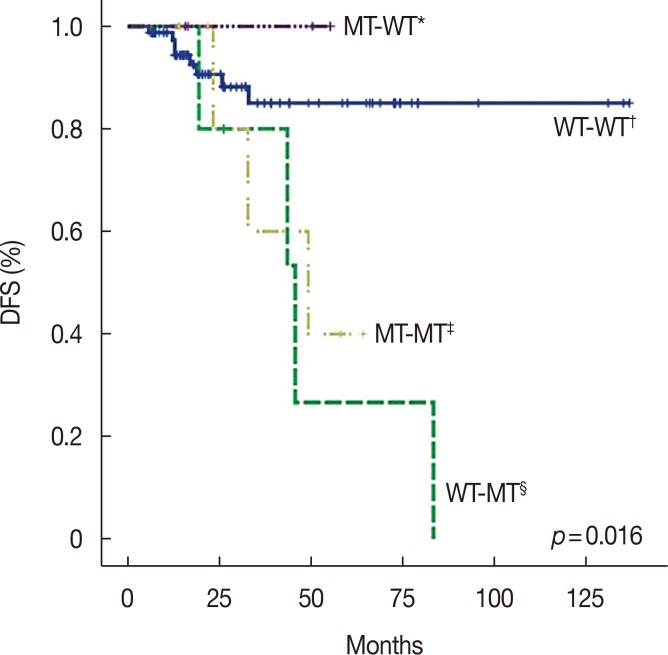
Figure 2
Survival curve for disease-free survival (DFS) according to mutation change status. There are four groups of mutation change status in sequential analysis. Due to lack of recurrence in the mutant-wild (MT-WT) group, Kaplan-Meier methods could not be utilized. The log-rank test was used to reveal significantly different survival curves for DFS (p=0.016). Subgroup analysis determined a significant DFS difference between the WT-WT group and WT-MT groups (p=0.005).
![]()
 XML Download
XML Download