

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Functional dyspepsia (FD) has been defined as a medical condition that significantly influences daily life, and is characterized by one or more upper abdominal symptoms, postprandial fullness, early satiation, epigastric pain, and epigastric burning in the absence of any explanatory organic or metabolic disease.12 Large-scale studies have shown the prevalence of FD lies between 10 and 30% worldwide3 and between 8.1% and 37% in the Korean population.45 FD reduces qualities of life and its symptoms cause emotional distress, and thus, FD imposes financial burdens due to direct medical costs and productivity losses.
A number of studies have been conducted to identify factors associated with FD and its response to treatments, but these factors have not been well demonstrated to date. For example, in patients with dyspepsia, the prevalence of Helicobacter pylori (H. pylori) infection has been shown to be between 40% and 70%,6 and the H. pylori infection rate has been reported to be 2.3 times higher than in healthy controls,7 which suggest H. pylori might be a risk factor of FD. However, the results of studies on the effects of H. pylori eradication on FD symptom improvements differ.89 In addition, various predictive factors of poor symptom responses have been proposed, such as female gender, lower BMI, H. pylori infection, or delayed gastric emptying.1011 Unfortunately, few studies have evaluated relations between other clinical factors and symptom response in patients with FD, and even in these studies cohorts were not composed of H. pylori-eradicated patients.101112 Accordingly, we undertook to identify predictors of symptom response in FD patients.
SUBJECTS AND METHODS
1. Study design and patients
This prospective, multi-center clinical trial was performed between July 2014 and May 2016 in 14 tertiary hospitals distributed throughout Korea.13 All patients underwent screening gastroscopy for the identification of organic disease and completed a questionnaire prior to treatment commencement. Inclusion criteria were age ≥18 years, a diagnosis of FD in accordance with the Rome III criteria, and H. pylori-positivity as determined one of the following three methods: 1) the rapid urease test (CLOtest®; Delta West, Bentley, Australia); 2) the 13C-urea breath test (13C-UBT, UBiTkit; Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan); or 3) histologic confirmation of H. pylori by modified Giemsa staining. The exclusion criteria applied were: 1) an age of <18 years; 2) endoscopically confirmed structural disease (e.g., erosive esophagitis, peptic ulcer, mucosa-associated lymphoid tissue lymphoma, or dysplasia) but no gastritis or intestinal metaplasia; 3) history of gastric surgery; 4) gastric cancer or another malignancy; 5) previous H. pylori eradication therapy; 6) abnormal liver or renal function; 7) liver cirrhosis or chronic kidney disease or another uncontrolled concurrent disease; 8) pregnancy, lactation, or refusal to use contraception during the study period; 9) a drug history that might have affected eradication results, such as proton pump inhibitor (PPI), H2 receptor antagonist, mucosal protective agent, or antibiotics during the prior four weeks prior to study commencement; 10) a genetic or mental disorder or alcohol or drug addiction; 11) history of drug allergy or any specific contraindication for study drugs; or 12) any condition that might influence clinical results (as determined by the principal investigator), such as a well-controlled underlying cardiological, respiratory, or gynecological disease.
This study protocol was approved beforehand by the Korean Food and Drug Administration (KFDA No. 30157) and by the Institutional Review Boards and Ethics Committees of all hospitals involved, which included Seoul National University Bundang Hospital (IRB number: B-1403/234-003). Written informed consent was obtained from all patients prior to enrollment, and the study was conducted according to Good Clinical Practices and the Declaration of Helsinki. The study protocol was registered at ClinicalTrials.gov and the Clinical Research Information Service as a secondary outcome measure of NCT02159976 and KCT0001176.
2. Questionnaire and symptom assessment
The questionnaire requested demographic data, BMI, smoking (never smoker/ex-smoker/current smoker) and alcohol (never drinker/ex-drinker/current drinker) habits, and details of comorbidities and of the Rome III criteria of FD.1 The Korean version of the questionnaire used was derived by translation from the original Rome III FD module and has been validated.14 Briefly, the questionnaire consisted of 11 questions, which addressed the presence of FD and the severities of symptoms using symptom frequencies. FD was defined as the existence of one or more of the following symptoms: 1) bothersome postprandial fullness; 2) early satiation; 3) epigastric pain; or 4) epigastric burning for at least the previous three months with a symptom onset at least six months prior to diagnosis based on Rome III criteria. In the questionnaire, FD was classified as postprandial distress syndrome (PDS) or epigastric pain syndrome (EPS). PDS was defined as the existence of one or both of the following symptoms: 1) bothersome postprandial fullness occurring after ordinary sized meals at least several times per week or 2) early satiation preventing complete consumption of a regular meal at least several times per week. EPS was defined as the existence of all of the following symptoms: 1) pain or burning of at least moderate severity localized to epigastrium at least once per week; 2) pain not relieved during the same day; and 3) pain not relieved by defecation or flatus. In addition, patients that met the criteria for PDS and EPS were assigned to a PDS/EPS group. Patients were also required to rate baseline symptom severity using a 5-point Likert scale: 1. minimal discomfort, 2. mild discomfort, 3. moderate discomfort, 4. severe discomfort, 5. very severe discomfort.
Patients were requested to revisit one year after H. pylori eradication commencement when patients completed the same questionnaire and were evaluated to assess symptom improvements. When a patient was unable to visit hospital, the questionnaire was completed by phone. Dyspeptic symptom responses were classified as; complete response (>75% symptom resolution), satisfactory response (≥50% but <75%), partial response (≥25% but <50%), and refractory response (<25% symptom resolution). Patients with ‘complete’ or ‘satisfactory’ response were defined as responders, and those with ‘partial’ or ‘refractory’ response were defined as poor responders.11 During the follow-up period, the patients were allowed to take prescribed drugs for symptom control after completing H. pylori eradication therapy, but these medication histories were recorded.
3. Assessment of H. pylori infection
H. pylori infection statuses were determined by Giemsa staining or by using the rapid urease test (CLOtest®) or the 13C-urea breath test (13C-UBT, UBiTkit). Four gastric mucosal tissues (from the greater and lesser curvatures of antrum and corpus) were acquired from each patient by forceps biopsy during endoscopy and fixed in formalin for Giemsa staining. Two additional gastric mucosal tissues from the lesser curvature of antrum and corpus were used for rapid urease testing (CLOtest®).
Patients fasted for at least four hours prior to the 13C-urea breath test (13C-UBT, UBiTkit). Briefly, after obtaining an initial breath sample, patients drank 100 mL water containing 100 mg of 13C-urea powder (UBiTkit™; Otsuka Pharmaceutical Co., Ltd.), and 20 minutes later a second breath was obtained. H. pylori infection status was determined using an isotope ratio mass spectrometer (UBiT-IR300; Otsuka Electronics, Osaka, Japan) using the obtained breath samples. The cut-off value of the procedure was 2.5%.
4. H. pylori eradication therapy and follow-up
Initially, patients were randomized to receive sequential therapy for 10 days or modified bismuth quadruple therapy for 14 days.13 If a patient failed to achieve eradication after 10 days on sequential therapy or 14 days on modified bismuth quadruple therapy and requested a second-line eradication therapy, quinolone-based triple therapy or traditional bismuth quadruple therapy was recommended. 13C-urea breath testing (13C-UBT, UBiTkit) was conducted to determine H. pylori eradication status four weeks after treatment completion.
5. Statistical analyses
The statistical analysis was performed using the SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were analyzed using Pearson's chi-square (χ2) test or Fisher's exact test and results are presented as numbers (percentages). Continuous variables were analyzed using the Student's t-test and results are presented as means±standard deviations. Univariate and multivariate logistic regression analyses were used to identify risk factors; results are expressed as ORs and 95% CIs. Statistical significance was accepted for p-values <0.05.
RESULTS
1. Patients characteristics
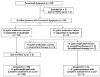
Sixty-five H. pylori-infected treatment-naïve patients with FD were enrolled in the present study (Fig. 1). Mean age of the 65 patients was 51.9 years (range, 23-76 years), and 33 (50.8%) were women. Numbers of patients with PDS, EPS, or overlapping PDS/EPS were 53 (81.5%), 43 (66.2%), and 31 (47.7%), respectively. Other clinical data and personal health habits are detailed in Table 1.
2. Responses to H. pylori eradication treatment
One patient of the 65 patients was lost to follow-up. Of the remaining 64 patients, 56 (87.5%) achieved eradication success, and of the eight patients in whom eradication therapy failed, six received second-line eradication therapy and two refused further treatment. Of these six patients, five (83.3%) achieved eradicated success after second-line eradication therapy. Therefore, 61 patients (95.3%) were allocated to the H. pylori-eradicated group and three (4.3%) to the H. pylori-persistent group. However, one patient in the H. pylori-eradicated group could not be contacted for the one-year symptom assessment (Fig. 1).
FD response rates at one year in the H. pylori-eradicated (n=60) group were 75% for responders (complete or satisfactory FD response) and 25% for poor responders (partial and refractory FD response) and in the H. pylori-persistent (n=3) group were 0.0% and 100.0%, respectively (p=0.021) (Table 2).
3. Medication received during follow-up
Of the 64 patients, 10 (15.6%) received medication during follow-up. Mean prescription period was 2.3 months (range, one to 9.5 months). More specifically, four patients (6.3%) received a prescription for one month, five (7.8%) for two months, and one (1.6%) received a prescription for 9.5 months. None of these patients had taken a prescribed drug during the two weeks before one-year assessments. Regarding types of drugs taken, two patients took PPIs, two PPIs and antacids, two PPIs, antacids, and prokinetic agents, one took a prokinetic agent, and other three took antacids and prokinetic agents.
4. Predictive factors of poor response of functional dyspepsia at one year
The predictive factors for poor FD response at one year are presented in Table 3. Univariate analysis showed H. pylori persistence (p=0.021), a female gender (p=0.025), and receipt of medication (p=0.013) were significantly associated with poor response, and that age, smoking, alcohol consumption, the presence of an underlying disease (e.g., diabetes mellitus and hypertension), type of eradication therapy, FD subtype, and baseline symptom severity were not associated with poor FD response. Multivariate analysis with respect to age, gender, BMI, diabetes mellitus, hypertension, and overlapping PDS/EPS showed only a female gender (OR, 4.70; 95% CI, 1.17-18.88) was independently related with poor FD response at one year. Unfortunately, multivariate analysis computation of the OR for H. pylori eradication was not possible because there was no H. pylori-persistent patient in the responder group.
DISCUSSION
A previous randomized, double-blind, placebo-controlled study failed to evaluate the efficacy of H. pylori eradication in H. pylori-infected Korean patients with FD, because most patients diagnosed with FD using the Rome III criteria would not agree with the suggestion that they should not use rescue medications during the study period.15 Given this experience, we focused on identifying predictors of FD among several factors, including H. pylori eradication, at one year after commencing eradication treatment. Our multivariate analysis results showed a female gender predicted the presence of dyspeptic symptoms at this time. The natural history of FD has not been well characterized, although the limited data available suggest that approximately 50% of patients remain symptomatic over five years of follow-up.1617 In the present study, it is difficult to conclude anything regarding the benefit of H. pylori eradication because eradication failed in only three patients. However, 73.3% of the eradicated group achieved complete FD response (≥75%) and 1.7% achieved satisfactory FD response (50-74%), which suggests successful H. pylori eradication is associated with FD improvement.
FD is regarded a multifactorial disease that may involve the brain-gut axis, gastroduodenal motility, visceral hypersensitivity, psychosocial factors, high gastric acid levels, the presence of H. pylori, genetic factors, dietary factors, and post-infectious conditions.18192021 Of these, H. pylori has been suggested to be a potent risk factor of FD, because several of the factors of FD are also affected by H. pylori infection. Involvement of the brain-gut axis in FD pathophysiology is an area of active research. In a recent Kyoto global consensus, it was suggested dyspeptic symptoms in patients with H. pylori infection be viewed as a disease entity distinct from FD and recommended that H. pylori eradication be adopted as a first-line therapy for H. pylori-infected patients with dyspepsia.22 Although this recommendation was controversial with respect to costs and adverse effects of H. pylori eradication in patients with FD,2324 we suggest H. pylori eradication therapy might be a reasonable option for some FD patients with H. pylori infection.
Despite the limitations of the present study, our results concur with those of randomized controlled trials and meta-analyses studies in terms of symptom response in FD patients after H. pylori eradication.8252627 A recent meta-analysis of 23 randomized controlled trials also demonstrated the benefits of H. pylori eradication on FD symptoms (pooled risk ratio [RR], 1.23 [95% CI, 1.12–1.36]).8 Interestingly, when subgroup analysis was performed with respect to follow-up period, H. pylori eradication was found to result in FD symptom improvements after follow-up for more than one year (RR, 1.24; 95% CI, 1.12–1.37) but not in the short-term (<1 year; RR, 1.26; 95% CI, 0.83–1.92).8 The authors considered long-term elimination of H. pylori improved symptoms by reducing inflammation and allowing gastric hormone levels to normalize. Interestingly, in another study, FD symptom improvement by H. pylori eradication was found to be more effective in Asian (OR, 1.54; 95% CI, 1.07–2.21) than in European (OR, 1.49; 95% CI, 1.10–2.02) or American populations (OR, 1.43; 95% CI, 1.12–1.83).25
In terms of factors that predict FD symptom response after H. pylori eradication, we found a female gender was significantly associated with poor response by multivariate analysis. Despite this finding, we do not suggest that physicians dispense with H. pylori eradication treatment in women with dyspepsia. Rather we suggest that physicians and female patients understand the lower likelihood of an improvement of dyspepsia by H. pylori eradication. In a study on a young healthy population, it was found dyspeptic symptoms were more frequent in females than males (p<0.05),28 and in another, female patients with FD were found to have significantly longer gastric emptying times than male patients and female controls.29
Higher prevalences of psychological co-morbidities in women may have influenced symptom response.3031 We recently suggested gender-related differences of ghrelin and nociception-related genes and psychological factors in males and females underlie FD symptoms,32 and recommended more attention be paid to psychological or emotional status, especially in female FD patients.32
Furthermore, the drug prescription rate was significantly higher in the poor responder group, indicating patients with poor symptom responses need more drug prescriptions. Lacy et al.33 conducted an interesting study that identified medication risk-taking behavior among FD patients. When asked whether they would take a hypothetical medication that might cure their FD symptoms, 49% of FD patients replied they would accept a mean 12.7% risk of sudden death (range 1-90%) for a 99% chance of cure.33
Regarding psychopathologic aspects, Hsu et al.34 studied 187 FD patients diagnosed using the Rome III criteria and found patients exhibiting PDS and EPS overlap had more severe psychopathological distress symptoms than those without overlapping symptoms. In the current study, the proportion of the overlapping PDS/EPS type was higher in the poor responders group (66.7%) than in the responders group (37.8%), but low numbers prevented analysis. Therefore, we suggest further studies be conducted to evaluate the association between symptom response and PDS/EPS overlap in FD patients.
Some limitations in this study warrant mention. First, the H. pylori-persistent group was very small. Furthermore, patients who failed first eradication therapy requested second-line eradication during follow-up, particularly those with FD symptoms, and these requests could not be denied. A similar situation arose in a previous randomized, prospective multi-center study that sought to evaluate the effect of H. pylori eradication on H. pylori-infected Korean patients with FD. The study was abandoned because only four patients satisfied the study criteria after one year.15 Second, we did not evaluate whether oral contraception had been used at one-year follow-up visits. However, in terms of oral contraceptive use, the current rate was found to be less than 1% in a Korean Health Examinee cohort study,35 and thus, its effect is likely to have been negligible in the present study. Third, we did not evaluate gastrointestinal symptoms, anxiety, or depression using a validated scoring system such as the Gastrointestinal Symptom Rating Scale, gastrointestinal symptom scores, or the Hospital Anxiety and Depression Scale. Finally, second-line eradication therapy was not preselected. However, we believe it had little impact on eradication rates, because the eradication rates of second-line eradication therapy in the present study were similar to those observed in recent Korean studies that investigated the eradication rates of second-line H. pylori eradication therapies.3637
In conclusion, the study shows female gender predicts poor FD response to H. pylori eradication in H. pylori-infected patients with FD. Successful H. pylori eradication appeared to be associated with the FD improvement, but the number of non-eradicated patients was too small to permit analysis.



 XML Download
XML Download