

 PDF
PDF ePub
ePub Citation
Citation Print
Print



The epidemiology of human immunodeficiency virus (HIV) infection in Korea is characterized by an increasing number of newly diagnosed HIV cases and proportion of late-presentation diagnoses [12]. Early diagnosis is important to decrease the opportunity for onward HIV transmission [3], and voluntary HIV testing is considered an effective strategy to enhance early detection of HIV infection [4]. Offering rapid HIV tests may encourage voluntary HIV testing [56]. In this context, in 2014, use of rapid HIV test was encouraged in place of conventional enzyme immunoassay (EIA) method, anonymous HIV testing in four public health centers in Seoul [7]. As a result of the implementing of rapid HIV tests, the average monthly numbers of HIV tests provided and HIV-positive diagnoses were approximately ninefold and sixfold greater, respectively, after adoption of the rapid HIV test. Based on these observations, rapid HIV testing was implemented in all 25 public health centers in Seoul in March 2015.
All of the 25 public health centers received additional funding to support their transition to rapid HIV testing, together with one or two additional laboratory technician(s). Rapid HIV testing and counseling are performed at isolated area for privacy of examinees. The public health center staff members were trained in this testing and discussion of the test results, and were educated about its advantages and disadvantages and the differences between rapid and conventional tests. Educative materials regarding rapid HIV testing for examinees were provided in the form of a brochure and booklet. To evaluate the frequency of HIV tests before and after adoption of rapid testing, the public health centers provided a monthly report on the total number of such tests performed, and their results.
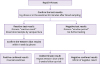
The HIV testing algorithm was developed and revised after conducting a pilot project in 2014, and was included in the written protocol (Fig. 1). Trained examiners offered the rapid test by finger-stick using the SD BIOLINE HIV-1/2 3.0 (Standard Diagnostics, Inc., Yongin-si, Korea) kit, which has high sensitivity and specificity, 100% and 99.3%, respectively [8]. The EIA test was offered to examinees if they preferred it. Examinees were informed that the result of rapid HIV tests might be negative during the window period, which is longer than that of the fourth-generation EIA test, and they should be tested again if they might have been exposed to HIV recently. The results of the tests were confirmed by phone or by the staff member who performed the test 20 min after blood sampling. Examinees with positive test results were taken a further blood sample to confirm HIV infection by Western blot assay, performed by the Seoul Research Institute of Public Health and Environment or the Korea Centers for Disease Control and Prevention. The results were confirmed within 1 week by telephone, and those confirmed to have HIV infection were referred to staff for further counseling in the public health centers. This is a report of outcome of a public health strategy which have run by Seoul Metropolitan Government for public interest.
During March and December 2015, 20,987 rapid HIV tests were performed, of which 233 were positive; of these, 166 accepted confirmatory tests and 67 refused; 116 were confirmed to have HIV infection and 9 were indeterminate by Western blot. During 2012 and 2013, prior to adopting rapid HIV tests at the 25 district public health centers in Seoul, 4,267 and 3,654 conventional HIV tests were performed, of which 69 and 93 were positive (Table 1). Compared to those in 2012 and 2013, the number of HIV tests performed and the number of positive results increased by sevenfold and twofold, respectively, during the study period.
Adoption of rapid HIV tests in public health centers was subject to several limitations. First, we could not determine the number of repeat tests in a single individual or whether known HIV-infected persons underwent rapid testing. Because rapid testing in public health centers is performed anonymously without personal information (as was the EIA test) to minimize the stigmatization issue. Thus, some examinees might have undergone multiple rapid tests. Second, the sensitivity of the rapid HIV test for detecting early-stage HIV infection is lower (22-33% vs. 76-88%) than that of EIA tests [9]. To minimize the problems due to the longer window period, examinees were provided information through educative materials and by trained staff members. In addition, the above information was offered to people who should be tested via the websites of public health centers and communities of men who have sex with other men. Anonymous HIV testing should be encouraged in groups at high risk for HIV infection [10], thus, increasing the overall volume of voluntary HIV testing would benefit early detection of HIV infection and reduction of the risk of onward HIV transmission [11].
In conclusion, expansion of the provision of rapid HIV tests in public health centers increased the number of voluntary HIV tests.

 XML Download
XML Download