

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Needlestick injuries (NSIs) expose healthcare workers (HCWs) to the risk of important blood-borne infectious diseases. NSIs can also cause severe psychological distress even when infections do not occur and may lead to a cost burden of medical care and lost working time [123]. World Health Organization (WHO) reported in 2003 that there were 3 million accidental NSIs, leading to 37% of all new hepatitis B virus (HBV) cases in HCWs, 39% of new hepatitis C virus (HCV) cases and 5.5% of new human immunodeficiency virus (HIV) cases [4]. To counteract the complications of NSIs, several countries have enacted legislation regarding NSIs and safety-engineered devices (SEDs) [5]. WHO guideline in 2016 recommended the use of injection devices with sharp injury protection and reuse prevention features by HCWs who deliver intramuscular, subcutaneous or intradermal injectable medications to patients [6]. In the USA, a significant decrease (38%) in the hospital NSIs rates occurred only after the Needlestick Safety Prevention Act was enacted and when safety devices became the predominant technology in healthcare settings [78]. The introduction of safety needle devices into the clinical setting combined with appropriate training may significantly reduce the number of occupationally acquired NSIs [9].
However, a wide range of NSIs among HCWs from 14.9% to 69.4% has been reported. The NSI rates differed by country, use of safety devices and reporting systems [5]. Cost may be a practically important barrier to the full access of SEDs, but the absence of well-coordinated regulation may underlie the failure. The feasibility of enacting regulation for SEDs in healthcare facilities may depend on the situation of individual country. Researchers can narrow the gap by providing practical solutions to overcome the obstacles to planning and implementing the SEDs in healthcare settings.
In South Korea, the use of SEDs is not prevalent and there are few studies to guide the implementation of SEDs in the healthcare facilities and to deal with regulatory policy regarding the active introduction of the SEDs. In this study, we described an experience in a hospital to implement a SED lancet for glucometer replacing a conventional prick lancet under no obligatory regulation. We intended to eliminate the lancet-related NSIs to zero incidence using the SED lancet with sharp injury protection and reuse prevention features and to share our practical experience during the intervention with the hospitals considering the SEDs.
Materials and Methods
1. Setting
This study was conducted in a 767-bed referral teaching hospital having one emergency room (ER), three intensive care units (ICUs) and 17 general wards. There were approximately 1,500 workers in the hospital. The infection control office (ICO) consisted of one infectious diseases physician who concurrently served as a director of the ICO, one full-time and one part-time nurse.
The ICO had a NSI prevention program for over 10 years. We receive a structured report for NSIs from individual HCWs. An injured HCW is interviewed by an infectious diseases physician about the injury and tests or medications prescribed accordingly. Post-exposure immunization and serological follow-up are made according to general recommendations for free. The hospital has a free vaccination policy for employees including HBV according to their immune status. Compiled reports and interviews were analyzed quarterly a year. Possible solutions were discussed in the infection control committee presided by a hospital chief executive officer (Fig. 1). To minimize underreporting we do not impose a cost for medical care and impose a direct penalty for failure to maintain standard guidelines. However, focused education and departmental feedback concerning common failures and critical issues are performed (Fig. 1). A few SEDs were in use in limited places, including a vacuum tube venipuncture system for outpatient phlebotomy, and a safety syringe for isolated patients of infectious diseases. We were using a prick lancet for glucometer blood testing.

2. Study design
Primary goal of the study was to eliminate the lancet-related NSIs by replacing a conventional prick lancet with a safety-engineered lancet. Secondary goal was to check if the implementation of a SED was cost-effective. Among various SEDs, a lancet SED was selected for the intervention because the cost difference between conventional and SED lancets was most tolerable at the initial evaluation and the incidence of NSIs was steadily affecting various HCWs and departments, which could not be changed by only education.
The SED lancet product had both sharp injury protection and reuse prevention features (SafeLan; Bosung Meditech, Wonju-si, South Korea). The intervention was implemented in a step-by-step manner and depicted in Figure 1. A single armed uncontrolled hospital-wide intervention study was performed for 2 years. Before the intervention, a spot sample test of the SED lancet was performed for 1 month at an emergency room to test the applicability and acceptability of the SED lancet by HCWs. A post-use survey for all the nurses in the emergency room was conducted about the utility of safety lancet. The questionnaire included 5 items asking about ‘willing to use, easy to use, patient-friendly, preventative for reuse and preventative for needlestick injury’. The paper questionnaire was distributed and returned after 1 month of test use. Then, a pilot implementation of the SED lancet in two places, an emergency room and an infection-ward for contact and airborne isolations, for 12 months was conducted under a decision of the infection control committee. Based on the results of pilot implementation, all conventional prick lancets in all departments of the hospital were replaced with the SED lancet by an institutional policy. Education on use of the new SED lancet was performed at each working unit before the implementation using education materials. A small number of prick lancets was needed in limited practices such as microcapillary test and continued to be used.
We collected data for 5 years, including 2 years of pre-interventional baseline, 1 year of a pilot study and 2 years after the intervention. The incidence of all kinds of NSIs and lancet-related NSIs was monitored. The incidence of NSIs was calculated as the number of NSIs reported each year per 100 HCW-years and per 100 average yearly hospital bed number.
Overall direct cost of the intervention was estimated with regard to average values of 2-year period before the full intervention in terms of a device cost and a cost of post-exposure medical care. The amount of lancet devices used in each department of the hospital was monitored monthly in the logistics department. Post-exposure medical care included the testing of baseline and follow-up for HBV, HCV and HIV according to the individual risk factor, and the post-exposure prophylaxis for HBV and HIV as recommended [101112]. We did not analyze the individual cost related to each risk factor but calculated the mean cost per NSI. As there was not a NSI-related infection during the study period, treatment related cost was not included. Incremental cost-effectiveness ratio per injury avoided was calculated by comparing the cost of baseline and 2nd year of intervention.
3. Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Boramae Medical Center (No. 30-2018-4). Collection of informed consent was waived because this study was conducted as part of an institutional policy to improve internal safety. All personal identifiers were anonymized for confidentiality before data processing. This research was in compliance with the Helsinki Declaration.
4. Statistical analysis
The NSIs incidence rates before and after the intervention were analyzed by Poisson regression. All statistical tests were two-tailed, and P values <0.05 were considered significant. All statistical analyses were performed using SPSS (version 20.0, IBM Corporation, Armonk, NY, USA).
Results
1. Zero incidence of lancet-related NSIs
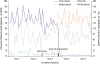
There were 29 cases of conventional prick lancet-related NSIs for 3 years before the full implementation of SED lancet. Six cases (20.7%) of the NSIs occurred during procedures, 4 cases (13.8%) shortly after procedures and 19 cases (65.5%) due to random spillage of used lancets. The proportion of prick lancet-related NSIs among yearly all kinds of NSIs during two years before the pilot study was average 11.7% (22/188) (Fig. 2).
Figure 2
Incidence of total needlestick injuries (NSIs) and lancet-related NSIs versus usage of conventional prick lancet and safety lancet for 5 years. Open arrow indicates the start of a pilot study for 1 year, and black arrow indicates the start of the full intervention replacing prick lancet (bold broken line) with safety lancet (bold dotted line). NSIs from all causes stayed unchanged for the entire period (gray light dotted line), but NSIs by lancet (solid line) was eliminated abruptly after the start of intervention (black arrow).
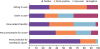
During the spot sample test at an emergency room, the return rate of the questionnaire was 83.7% (31/37). The proportion of negative responses to the safety lancet were low; 16.1% for ‘willing to use’, 3.2% for ‘patient-friendly’, 9.7% for ‘preventative for reuse’ and 0% for ‘preventative for needlestick injury’. However, 35.5% of the subjects responded negatively for ‘easy to use’ which reflected their unacquaintance with the new device and raised the need for education (Fig. 3). During the pilot study of 1 year, the number of all kinds of NSIs in the study places was 5 cases, and no case was related to lancet injury, compared with the number of all kinds of 19 NSIs and 5 prick lancet-related NSIs during previous pre-interventional 1 year.
Figure 3
Survey of the acceptability of a safety engineered lancet after 1 month of test use by nurses.
After the full implementation of SED lancets, the proportion of NSIs from lancets out of all kinds of NSIs was 4.8% (5/104) in the 1st year, but there was no lancet-related NSI among 96 cases of all kinds of NSIs in the 2nd year (P = 0.001) (Fig. 2). The 5 cases by lancet in the 1st year were all due to prick lancets from remaining stocks, and there was no case related to the SED lancet. The conventional prick lancet-related NSIs rate for 3 years before the full implementation was average 3.05 (range, 2.42-3.63) cases per 100,000 devices used. The rate soared to 70.58 cases per 100,000 devices in the 1st year of implementation. A small number of devices in remained stock during the washing period (denominator) made the rate abnormally high. It became zero in the 2nd year (Fig. 2).
The incidence of all kinds of NSIs was not influenced by the implementation of SED lancet. A total of 498 cases of NSIs from all kinds of devices in the hospital were reported during 5 years of total study period (Fig. 2). The overall incidence rate of NSIs was 6.87 cases per 100 HCW-years. The yearly incidence rate for the 3 years before the intervention was average 7.01 cases per 100 HCW-years (range, 5.78-7.64), and after the intervention they were 7.13 (1st year) and 6.17 (2nd year). A significant decrease of the incidence rates was not observed during the study period (P = 0.453). The overall incidence rate for 5 years by yearly bed number was 12.8 cases per 100 bed-years.
2. Cost-effectiveness of the SED lancet
Net direct costs related to the use of a prick lancet and post-exposure medical care from lancet-related NSIs during 2 years before the intervention was 18,393 US dollars (USD) in total (Table 1). The average unit cost for post-exposure medical care per person during the study period was 158.56 USD. The cost was only incurred from routine screening because there was no infected case from the NSIs. The unit price per piece of the SED lancet was 0.05 USD. The estimation for the direct cost for full replacement of prick lancets with a same amount of SED lancets was expected to be 20,093 USD, and for the post-exposure medical care to be zero cost.
Table 1
Cost analysis before and after the implementation of the safety-engineered lancet
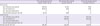
aThe values are average per year.
b‘Year-’ indicates study periods marked in the X-axis of Fig. 2.
$, US dollar; NSIs, needlestick injuries.
During the pilot study in the 2 units, the cost of SED lancet was tolerable. The cost expenditure was 1,320 USD for the SED lancet alone and there was no NSIs during the study period in contrast to 2,069 USD in total from the SED lancet and 5 NSIs by prick lancets in the pre-interventional year. Actual overall direct costs in the hospital during the 1st year after the complete implementation of SED lancets was 20,316 USD and rose to 20,701 USD in the 2nd year (Table 1). The incremental cost-effectiveness ratio was 210 USD per injury avoided.
Discussion
Our study showed that the replacement of a conventional prick lancet for glucometer with a SED lancet having sharp injury protection and reuse prevention features could eliminate the lancet-related NSIs. The effectiveness of medical safety devices as a key preventive measure for the NSIs is not something new [13]. However, there are many factors hindering the implementation of SEDs. Actual interventional studies describing how to implement a new individual SED may provide practical guidance for institutions considering the device. This kind of study was not known in South Korea yet and urgently needed. Our study may become one of the guides that can be followed.
Although the baseline frequency of lancet-related NSIs was relatively low (11.7%) in our study, our analysis indicated that the occurrence of injuries was steady, and the inappropriate disposal of the device caused injuries to various HCWs and housekeepers (65.5% of total lancet-related NSIs). One of the critical obstacles to implementation of safety devices was the unit price of the devices, especially if there was no obligatory regulation and the cost was not reimbursed. Overall direct cost expenditure in our study consisted of two components, device and post-exposure medical care. The unit prices of a prick and safety-engineered lancets were 0.05 USD and 0.06 USD per piece, respectively. The average cost of post-exposure medical care per injury was 158.56 USD in our hospital. The cost gap between the conventional device and SED is a complex function of technical innovation and reimbursement system. The cost of medical care is a function of the regional healthcare system and the occurrence of complicating infections. In this study, we found an appropriate SED at a tolerable price. The incremental cost-effectiveness ratio per injury avoided was 210 USD. In a country with higher medical costs, it may be more cost-effective to use this kind of SED [3]. We could persuade the board of management with the favorably estimated cost expenditure as in Table 1, and one year of pilot study in two wards showed that the SED lancet could eliminate the lancet-related NSIs at a tolerable cost. To ensure the user acceptability of the new safety device and the desired beneficial effect, we engaged healthcare workers in a field test of 1 month. We implemented the SED lancet to eliminate 11.7% of all kinds of NSIs. The proportion of lancet-related NSIs may differ by country or hospital. Taiwanese data showed that the incidence of lancet-related NSIs were 5.3% of the total NSIs [14].
In South Korea, there were several reports regarding the incidence of NSIs or occupational percutaneous blood/body fluid exposure in healthcare facilities, and the results variably ranged from 2.92 to 5.60 per 100 HCW-years [15161718]. The study periods were 1992 - 2007 or 2011 - 2015; one study was based on multiple-centers, and the others were all single-center studies. The incidence rate of injuries in the latest study was 5.60 per 100 HCW-years and 20.3 per 100 bed-years. The incidence rate in our study of 6.87 per 100 HCW-years and 12.8 per 100 bed-years was higher by a HCW-year unit but lower by a bed-year unit. Therefore, the rates of NSIs must be analyzed by several units to appropriately interpret the underlying causes. Global incidence rates of sharps injuries ranged from 1.4 to 9.5 per 100 HCW-years, resulting in a weighted mean of 3.7 per 100 HCW-years. The related costs were reported to be a mean of 272 euros per injury [19].
In South Korea, the Occupational Safety and Health Act [20] and the subsequent Enforcement Decree of the Occupational Safety and Health Act [21] contained general principles to protect employees from infectious diseases and exposure to blood-borne infections, but specific obligatory requirement for the safety-engineered devices was not included. The obligation for the use of SED will surely promote the safety of patients and HCWs. However, under our National Health Insurance Service which is operated by the government, the regulation needs to include the condition of how to reimburse the cost for devices.
Our study has several limitations. First, as the intervention was not a controlled study, other variables contributing to the successful elimination of lancet-related NSIs could not be identified. However, we could confirm that zero incidence could be reached with the SED lancet. Second, we did not analyze the details of post-exposure medical cost according to the pathogens and provided services. Small number of NSIs (n=16) was not eligible for further significant subgroup analysis. Third, single center study with 5-year duration may not be a solid base for reference. However, we demonstrated the steps to follow during the effective implementation of a SED and it can be a good example to follow.
In conclusion, our study showed that implementation of a SED lancet with sharp injury protection and reuse prevention features eliminated lancet-related NSIs. A sequential approach to assess major potential obstacles for the intervention as depicted in Fig. 1 was useful to convince all related stakeholders. The intervention was cost-tolerable, not substantially increasing the direct cost.
 XML Download
XML Download