

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Influenza is a serious viral disease [1] that can cause significant morbidity, particularly in older adults (aged ≥65 years) [2]. This age group is at high risk of influenza-related complications and hospitalization and can experience functional impairment and significant disability [34]. Influenza can also be fatal, and in adults aged ≥65 years, the risk of mortality due to influenza is higher than in younger adults aged <65 years [12]. Results from a study of the burden of influenza in England showed that over 90% of annual deaths from influenza occurred in older adults [5], and a similar rate of annual influenza-associated deaths has been reported for those aged ≥65 years in the USA [6].The impact of influenza on older adults is of particular concern in South Korea, where the proportion of the population ≥65 years is greater than in most other countries, and longevity continues to increase [7].
Vaccination is the most effective method for preventing influenza infection and is recommended for high-risk groups such as older adults [18–10]. This prevention of influenza infection in older adults is also associated with a reduction in exacerbations of heart failure, heart attacks, and strokes [2]. However, the effectiveness of influenza vaccination is lower in older adults (aged ≥65 years) than in younger adults, as the immune system wanes with age. This immunosenescence leads to defects in antigen presentation and decreased antibody responses [11–14].
Several strategies to improve the response to influenza vaccines in older adults are being investigated [13]. The addition of adjuvants, such as MF59, has been shown to enhance both humoral and cell-mediated responses to influenza vaccines in older adults. Adjuvants are thought to elicit these effects by enhancing antigen presentation, activation and maturation of dendritic cells, and production of inflammatory cytokines [13].
FLUAD® is an MF59-adjuvanted influenza vaccine, which was first approved for use in adults aged 65 years or older in Europe in 1997 [7]. It is currently approved in 38 countries including the US and many European countries [1516]. It has been approved in South Korea since 2009 and is marketed under two Tradenames (FLUAD® (Novartis) and VANTAFLU® (Sandoz), both manufactured by Novartis Vaccines and Diagnostics S.r.L., Siena, Italy).
The efficacy and safety of FLUAD® has been demonstrated in several clinical trials [1718]. Results from a phase III trial comparing the safety and immunogenicity of an MF59-adjuvanted vaccine with a non-adjuvanted vaccine in subjects aged ≥65 years showed that immune responses were higher in response to MF59-adjuvanted vaccine than the non-adjuvanted vaccine [19]. The MF59-adjuvanted vaccine was associated with higher levels of reactogenicity than the non-adjuvanted vaccine, however, events were generally transient and mild to moderate in severity. A meta-analysis of data from clinical trials in older adults has also shown that FLUAD® is well tolerated and more immunogenic than non-adjuvanted vaccines in those who have underlying diseases [20]. These findings are supported by results from a pooled analysis of safety data from 64 clinical trials, which showed that MF59-adjuvanted vaccines were well tolerated and offered clinical benefit compared with non-adjuvanted vaccines, including in older adults [17]. Results from a case-controlled study indicate the potential real-world benefits of vaccination, as FLUAD® significantly decreased the probability of older adults being hospitalized with pneumonia [21].
The post-marketing surveillance study reported here was mandated by the South Korean Food and Drug Administration (KFDA) guidelines for the re-examination of the safety of new drugs [22], and aimed to assess the safety of FLUAD® / VANTAFLU® in South Korean subjects aged ≥65 years.
Materials and Methods
1. Study design
This was an open-label, multicenter, post-marketing surveillance study that evaluated the safety of vaccination with the MF59-adjuvanted trivalent inactivated subunit influenza vaccine, marketed as either FLUAD® or VANTAFLU®, in South Korean subjects aged ≥65 years. The study was conducted across 24 sites, which included clinics and hospitals in the cities of Anyang, Daejeon, Gimpo, Goyang, Incheon, Jeongeup, Mokpo, Seoul, and Yangjoo, South Korea. Data were collected between October 16, 2010 and October 25, 2014.
2. Subjects
Male and female individuals aged ≥65 years, who were eligible to receive seasonal influenza vaccination according to the South Korean prescribing information and who provided informed consent, were included in the study. Individuals who had any history of anaphylaxis, serious reactions to a vaccine, or hypersensitivity to influenza viral proteins, any excipients, eggs (including ovalbumin), or chicken protein were not eligible to enter the study. In addition, individuals with any condition that in the investigator's opinion may have interfered with evaluation of the study objective were also excluded from the study. This study was conducted according to the Declaration of Helsinki, the International Conference on Harmonization good clinical practice (GCP), and relevant regulatory and GCP requirements. All subjects provided written informed consent.
3. Vaccines
FLUAD® (Novartis) and VANTAFLU® (Sandoz) are identical and differ only in their trade names. The vaccines, which were administered according to the South Korean prescribing information, contained 15 µg hemagglutinin of the A/H1N1, A/H3N2, and B influenza strains as recommended by the World Health Organization for the respective Northern Hemisphere influenza season. Subjects received a single 0.5 mL dose of vaccine intramuscularly in the deltoid muscle of (preferably) the non-dominant arm.
4. Study endpoints
Solicited local and systemic adverse events (AEs) were collected from day 1 to 4 of the study. The local solicited AEs included tenderness, erythema, induration, swelling, and pain at the injection site, and the systemic solicited AEs included chills, myalgia, arthralgia, headache, sweating, fatigue, and fever (e.g., axillary temperature ≥38°C). Subjects were observed for the first 30 minutes following vaccination for identification of any AEs that occurred immediately. Following this initial observation, subjects were instructed to complete a diary card to record any AEs that occurred during days 1 to 4.
All unsolicited AEs and serious AEs (SAEs) were recorded from day 1 until study termination (day 29) using a diary card. On day 29, a follow-up call was made to every subject individually to review the diary card, determine the subject's clinical status, and finish the subject's participation in the study. The intensity of AEs was classified as mild (transient, with no limitation on normal daily activities), moderate (some limitation on normal daily activities), or severe (unable to perform normal daily activities) by the investigator. The relationship of an AE to the study treatment was defined by the investigator as unrelated, possibly related, or probably related. SAE data were collected by the investigator and assessed for the relationship to the vaccine.
5. Statistical analyses
The enrolled set included all screened subjects and was used for the reporting of demographic and baseline characteristics. The safety set included all subjects who were screened, who received study vaccination and who provided post-vaccination safety data. This data set was used for the analysis of solicited and unsolicited AEs.
The demographic and baseline characteristic data were presented descriptively, and AE data were reported by vaccine group. The proportion of subjects reporting solicited local and systemic AEs from day 1 to 4 following vaccination and the proportion of subjects reporting unsolicited AEs from day 1 to 29 were assessed.
A total of 750 individuals aged ≥65 years was planned for enrollment into this study over a maximum period of 6 years, which complied with KFDA regulations [22].
Results
1. Subject disposition
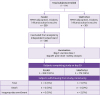
Of the 770 subjects enrolled in this study, 389 received FLUAD® and 381 received VANTAFLU®. Of those enrolled, 765 subjects completed the study (Fig. 1). Two subjects were withdrawn from the study as they did not meet the age criteria and had been enrolled in error, and three subjects were excluded from analysis because of a consent form issue. Protocol deviations were reported in a total of five subjects.
2. Demographic and baseline characteristics
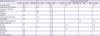
No differences in baseline characteristics were observed between the groups of subjects receiving FLUAD® and VANTAFLU® (Table 1). The mean age for the enrolled set was 73.4 years and there was a higher proportion of females (60%) than males (40%), 74% of subjects had previously been vaccinated, and 56% received concomitant medication. All subjects were of South Korean ethnicity.
Table 1
Subject demographics at baseline

3. Safety
As expected, there were no differences in safety findings with the two different brand names for the same vaccine. Overall, 39% of subjects experienced any solicited AE (Table 2). Local AEs were reported by 33% of subjects with the most common solicited local AEs being injection-site pain (30%) and tenderness (27%) (Fig. 2). The majority were of mild or moderate intensity and resolved by day 4 (Table 2). One subject reported severe pain and tenderness (Table 2), with neither symptom continuing beyond day 2. Systemic AEs were reported by 19% of subjects with the most common solicited systemic AEs being myalgia (11%) and fatigue (8%). Most of the events were mild or moderate in severity (Fig. 3, Table 2). Severe fatigue was reported by two subjects and fever by one subject (Table 2).
Table 2
Subjects with any solicited adverse event and severity from 6 hours until day 4 after vaccination (safety set)

Figure 2
Solicited local adverse events (AEs) reported by subjects between 6 hours and day 4 after vaccination (safety set).
aSevere tenderness and pain were reported by a single subject in FLUAD® group.

Figure 3
Solicited systemic adverse events (AEs) reported by subjects between 6 hours and day 4 after vaccination (safety set).
aSevere fatigue was reported by two subjects in FLUAD® group.

In total, 4% of subjects reported unsolicited AEs (Table 3). Nasopharyngitis was the most common unsolicited AE followed by respiratory tract infection (Table 4). Four subjects reported unsolicited AEs (nasopharyngitis, pruritus, dizziness, and injection-site dysesthesia) that were judged to be possibly or probably related to the study vaccine (Table 4). No deaths occurred during the course of this study, no SAEs were reported, and no AEs led to interruption or delay in vaccination, premature withdrawal, hospitalization, or death (Table 3).
Table 3
Subjects with an unsolicited adverse event from 6 hours until day 4 after vaccination (safety set)

Table 4
All and possibly or probably related unsolicited adverse eventsa
Discussion
Influenza is a particular public health concern in South Korea, where life expectancy is increasing and the proportion of the population that is aged ≥65 years is greater than in most other countries [7]. The results from this study show that FLUAD® / VANTAFLU® was well tolerated in older adults (aged ≥65 years) in South Korea. As of April 30, 2015, FLUAD® has been given to 81.5 million individuals worldwide and has favorable overall safety and tolerability profiles. The results presented here add to this large body of safety data for MF59-adjuvanted influenza vaccines.
The safety results for FLUAD® / VANTAFLU® in older South Korean adults (aged ≥65 years) presented here are consistent with earlier reports for the MF59-adjuvanted trivalent influenza vaccine. In two studies assessing the administration of FLUAD® in older adults over three consecutive influenza seasons, the most commonly reported reactions were mild and local [2324], and were generally transient, lasting only 2 to 3 days post-vaccination [24]. Injection-site pain was the most commonly reported local solicited reaction in a study assessing the formulation of FLUAD® in older adults [23], as it was in the study presented here. A randomized trial that compared the safety, immunogenicity, and tolerability of FLUAD®, Intanza® (an intradermal influenza vaccine manufactured by Sanofi Pasteur, Lyon, France), and AGRIFLU® (Novartis Vaccines and Diagnostics S.r.L., Siena, Italy), reported results comparable with those presented here: The most frequently reported local reaction and solicited systemic AE for FLUAD® were injection-site pain and myalgia, respectively, and, these events were generally mild or moderate in severity [25] Similarly, results from an analysis of safety data pooled from 64 clinical trials assessing the safety of MF59-adjuvanted vaccines [17] also reported findings comparable with the present study. Injection-site pain and myalgia were found in this analysis to be among the most common solicited local and systemic reactions, respectively, and nasopharyngitis was the most common unsolicited AE reported [17]
Influenza is a serious disease, especially in older adults as it can lead to excess morbidity, hospitalization, and mortality in this age group [13] Therefore, vaccination against influenza is recommended for this population as it can reduce mortality, the incidence of hospitalizations, and associated complications such as heart failure [2627]. However, the waning immune system of older adults can mean the response to conventional influenza vaccines is poor, illustrating the need for improved vaccines for this population [1328]. Vaccines that contain an adjuvant, such as MF59, have been shown to overcome immunosenescence in older adults, increasing the immune response and improving protection against influenza infection compared with conventional influenza vaccines [13]. The results from the study presented here add to the evidence demonstrating that MF59-adjuvanted influenza vaccines are well tolerated in older adults.
The main limitations of this study were that it did not include a non-adjuvanted comparator vaccine, and it was observational, thus not powered for robust or confirmatory statistical analyses. However, the real-world design of this study means that the results are reflective of daily clinical practice and therefore can be readily applied to the community setting in South Korea.
In conclusion, the overall safety and tolerability results of this post-marketing surveillance study show that the MF59-adjuvanted vaccine FLUAD® / VANTAFLU® was well tolerated and had an acceptable safety profile, and therefore can be used to vaccinate older adults (aged ≥65 years) in South Korea against influenza.
 XML Download
XML Download