

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Incisional hernia (IH) — a failure of the abdominal wall fascia to heal — is a common postoperative complication in abdominal surgery. Its incidence rate is 5%–50% after open abdominal surgery [1234], 20% after laparoscopic colorectal surgery [5], and 2.7% after laparoscopic sleeve gastrectomy [6]. However, long-term follow-up data regarding the incidence of IH after laparoscopic distal gastrectomy in patients with gastric cancer are unavailable.
Recently, laparoscopic gastrectomy has been recognized as a curative treatment for gastric cancer in East Asian countries. Several multicenter randomized controlled, short-term follow-up trials (Korean Laparoscopic Gastrointestinal Surgery Study trial [KLASS-01] [7], Chinese Laparoscopic Gastrointestinal Surgical trial [CLASS 01] [8], and Japan Clinical Oncology Group trial [JCOG0703] [9]) of laparoscopic distal gastrectomy in patients with gastric cancer have shown favorable results compared with open gastrectomy. Furthermore, laparoscopy-assisted distal gastrectomy (LADG) has been evolving into totally laparoscopic distal gastrectomy (TLDG). Thus, the location of the mini-laparotomy wound is moved from the right upper quadrant (RUQ) or upper midline for specimen extraction and reconstruction to the umbilical port site for specimen extraction alone [1011]. Recently, the authors of the present study encountered several cases of IH developing into mini-laparotomy wounds. The objective of this study was to determine the incidence and analyze the risk factors of IH following laparoscopic distal gastrectomy in patients with gastric cancer.
MATERIALS AND METHODS
This was a retrospective study using prospectively collected data. A total of 565 patients who underwent laparoscopic distal gastrectomy for gastric cancer (performed by Kim MC) at Dong-A University Hospital between June 2010 and December 2015 were enrolled. The inclusion criteria were as follows: 1) histologically confirmed gastric adenocarcinoma, 2) distal subtotal gastrectomy with more than D1+ lymphadenectomy, and 3) absence of combined resection except cholecystectomy. Patients with a history of gastric surgery or chemotherapy and/or radiotherapy were excluded. Our indication for laparoscopic distal gastrectomy in patients with gastric cancer involved clinical tumor staging below T3N1M0, without a bulky tumor or conglomerated metastatic lymph nodes. IH was diagnosed through physical examination or computed tomography (CT) imaging.
Mini-laparotomy wounds in LADG and TLDG
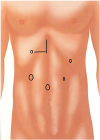
A mini-laparotomy wound (approximately 4–5 cm) in LADG was transversely or longitudinally located at the RUQ or upper midline. After intracorporeal stomach mobilization and lymph node dissection, gastric resection, specimen extraction, and reconstruction were sequentially performed through the mini-laparotomy wound. Stomach mobilization, lymph node dissection, and gastric resection were completed intracorporeally in TLDG. The specimen was extracted through the mini-laparotomy periumbilical wound. Subsequently, intracorporeal reconstruction was performed under the pneumoperitoneum (Figs. 1 and 2).

Closure of mini-laparotomy wound
Closure of the abdominal wall muscle and fascia in transverse incision was performed using layered closure with 5–6 No. 1 interrupted Vicryl® sutures (Ethicon, Somerville, NJ, USA). Non-layered closure was performed for the fascia in the midline incision using 5–6 No. 1 interrupted Vicryl® sutures. Skin closure was performed using Nylon suture or a skin stapler.
Follow-up
All patients were monitored postoperatively through a routine check, including physical examination, blood test, tumor marker test (alpha-fetoprotein, carcinoembryonic antigen, and carbohydrate antigen 19-9), chest radiography, endoscopy, and CT. For patients with pathologic stage I and II gastric cancer, follow-up examinations were performed every 6 months for the first 2 years and annually for the following 3 years. For those with pathologic stage III and IV gastric cancer, examinations were performed every 3 months for the first 2 years (only endoscopy every 6 months) and every 6 months for the following 3 years (only endoscopy every 12 months).
Statistics
Results are expressed as mean±standard deviation. Continuous variables were evaluated using the unpaired Student's t-test or Mann-Whitney U test. Categorical data were compared using the χ2 test or Fisher's exact test, as appropriate. Multivariate analysis for risk factors of IH was performed through logistic regression using SPSS Statistics 23.0 (SPSS Inc., Chicago, IL, USA). A P-value <0.05 denoted statistical significance.
Ethical statement
The study was approved by the Institutional Review Board (IRB) of Dong-A University Hospital (IRB No. DAUHIRB-18-114). The requirement for informed consent from patients was waived due to the retrospective nature of the study. This study was conducted according to the principles of the Declaration of Helsinki.
RESULTS
Of the 565 patients who underwent laparoscopic distal gastrectomy for gastric cancer, 16 developed IH in mini-laparotomy wounds (2.8%). The median duration of follow-up was 58 months (range, 25–90 months). IHs were diagnosed at a mean of 6.5 months (range, 3–15 months) postoperatively. Seven of these 16 patients (43%) underwent surgical repair.
Differences in clinicopathologic characteristics between the IH and non-IH groups
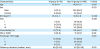
There was a significantly higher number of female patients and those with comorbidity in the IH group (P=0.013 and P=0.028, respectively) than that in the non-IH group. In addition, the body mass index (BMI) in the IH group was significantly higher than that observed in the non-IH group. Moreover, the follow-up duration was significantly different between the two groups (42 months vs. 60 months, P=0.031). The vast majority of IH cases developed in the TLDG group (15/16 patients, 93.7%). TLDG was performed since November 2012 (Table 1).
Table 1
Clinicopathologic characteristics between the IH and non-IH groups
Differences in surgical outcome between the IH and non-IH groups
Most surgical outcomes were not significantly different between the two groups. There was no significant difference in the incidence of postoperative complications (e.g., wound infection) between both groups. However, TLDG was more frequently performed in the IH group (P=0.001). Of note, 15/16 patients with IH had periumbilical wound hernia (Table 2).
Table 2
Surgical outcome between the IH and non-IH groups

Identification of risk factors for the development of IH in mini-laparotomy wounds using univariate and multivariate logistic regression analyses
A total of 16 independent clinical variables (6 preoperative and 10 surgical factors) were analyzed as potential risk factors of IH. Of these, the following seven were shown to be significant (P<0.2): female sex, higher BMI, presence of comorbidity, method of reconstruction, type of surgery, longer duration of postoperative hospitalization, and development of postoperative complications (Tables 1 and 2). Multivariate analysis using a logistic regression model showed that female sex (odds ratio [OR], 3.869; 95% confidence interval [CI], 1.325–11.296), higher BMI (OR, 1.229; 95% CI, 1.048–1.422), and presence of comorbidity (OR, 3.806; 95% CI, 1.212–11.948) were significant risk factors of IH (Table 3). However, the type of surgery (i.e., TLDG or LADG) did not significantly affect the development of IH (P=0.060) (Table 3).
Table 3
Risk factors for the development of IH in mini-laparotomy wounds using univariate and multivariate logistic regression analyses

DISCUSSION
The development of IH requires elective or emergency surgical treatment due to poor appearance and possible incarceration after abdominal surgery [2]. IH after laparoscopic surgery is linked to greater disappointment compared with that reported after open surgery in terms of postoperative patient satisfaction.
In the present study with a median follow-up of 58 months, the incidence of IH in mini-laparotomy wounds after laparoscopic gastrectomy in patients with gastric cancer was 2.8% (16/565 patients). This incidence was similar to that previously reported after laparoscopic sleeve gastrectomy [6] or laparoscopic staging surgery for endometrial cancer [12]. However, it was lower than that reported after laparoscopic colorectal surgery [5]. In laparoscopic colorectal surgery, specimen resection and anastomosis are performed simultaneously through a mini-laparotomy wound. The size of the mini-laparotomy wound in laparoscopic colorectal surgery is larger than that employed in laparoscopic gastrectomy.
According to a multivariate analysis of a large-scale study investigating the incidence of IH after open abdominal surgery [2], the following risk factors are independently associated with IH: wound classification III and IV, BMI ≥25 kg/m2, midline incision, incisional surgical site infection, preoperative chemotherapy, blood transfusion, increasing age by 10-year interval, female sex, and thickness of the subcutaneous tissue for every 1-cm increase. In other studies [1314], emergency surgery, malignant tumor, diabetes, collagen metabolic disorder, and chronic obstructive pulmonary disease were identified as independent risk factors of IH. In our study, female sex (OR, 4.55), high BMI (OR, 1.200), and presence of preoperative comorbidity (OR, 3.512) were independent risk factors of IH after laparoscopic gastrectomy. Due to the relatively small sample size of the present study, it was not possible to determine the roles of incisional surgical site infection, wound classification, and comorbidity classification as risk factors of IH. Unfortunately, the multivariate logistic regression analysis did not identify the type of surgery as an independent risk factor of IH. However, IH in mini-laparotomy wounds developed more frequently after TLDG than LADG.
In studies comparing LADG with TLDG [1011], identifying clinical advantages of TLDG over LADG is challenging. This is due to the lack of well-designed, randomized, controlled trials. However, clinical practice is evolving from LADG to TLDG because of the development of anastomotic skill and patient satisfaction with postoperative scarring and pain [15]. In the present study, almost all IH cases developed in the TLDG group, and the location of the IH in this group was the periumbilical site. Of note, the fascia of the periumbilical site is thinner and weaker than that of the upper abdominal wound.
Among the 16 patients with IH, 15 (93.7%) were diagnosed within 12 months postoperatively. Surgical treatment was performed in seven patients with IH (43.7%). Mesh repairs have been shown to be superior to primary repairs, with a recurrence rate of 11%–21% compared with 25%–52% reported for simple closure [16]. However, in our study, simple primary closure was performed in all seven patients because of the relatively small size of their IH. In this study, there was no recurrence.
A recent systematic review [17] assessed the closure methods for laparotomy incisions to prevent the development of IH and other wound complications. According to this review, monofilament sutures may be considered as the first choice for the closure of the abdominal wall. Absorbable suture materials may reduce the risk of chronic drainage from the wound. At Dong-A University Hospital, we traditionally used absorbable multifilament sutures for closure of mini-laparotomy wounds. The use of absorbable monofilament sutures for closure of mini-laparotomy wounds may be considered during TLDG for gastric cancer to reduce the risk of IH or chronic wound.
The limitations of this study are inherent to its retrospective design, including documentation error and bias in data review. However, this study involved sufficient follow-up duration to examine the incidence of IH.
In this study with median follow-up of 58 months, we found that the overall incidence of IH in mini-laparotomy wounds was 2.8%. The identified risk factors of IH after laparoscopic distal gastrectomy were female sex, high BMI, and presence of comorbidity. Surgical site infection, preoperative lung disease, or diabetes were not identified as independent risk factors because of the low surgical site infection rate (6/565 patients, 1%) and low IH rate. In conclusion, surgeons should monitor the closure of mini-laparotomy wounds in patients with risk factors of IH undergoing laparoscopic distal gastrectomy.
 XML Download
XML Download