

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As esthetic demands increase in society, patients are more frequently visiting dental clinics to be treated for gingival recession. Gingival recession is defined as exposure of the root surface due to an apical shift of the gingiva. It can be caused by many factors, including improper tooth brushing, recurrent inflammation, laceration, and iatrogenic factors such as subgingival restoration or placement of a dam clamp [12]. In addition, trauma from occlusion [3], a malpositioned tooth [4], improper frenal pull, and complications following periodontal treatment or orthodontic treatment [56] are often related to its occurrence. In addition to esthetic issues, gingival recession can cause problems including potential root caries or cervical abrasion, dentin hypersensitivity, and the disturbance of routine oral hygiene behaviors [78].
Various periodontal plastic surgery procedures have been introduced and applied to produce better esthetic treatment outcomes on areas of gingival recession for several decades [91011]. Procedures in which no tissue grafts or tissue substitutes are used include the coronally advanced flap (CAF), semilunar coronally repositioned flap, laterally positioned flap, and double papilla flap [1213]. However, the long-term results of these techniques demonstrated less predictability than procedures using grafts. Several studies have demonstrated that the combination of a subepithelial connective tissue graft (CTG) with CAF led to a greater reduction of the recession area and a greater increase in the width of keratinized gingiva than other combined treatments [1415]. However, this technique has some drawbacks, because subepithelial CTG is usually obtained from the palatal area, causing the patient to experience severe discomfort. Furthermore, the amount of palatal donor tissue is sometimes very limited. Alternative techniques using tissue substitutes have important advantages, such as the absence of limitations in the amount of graft material and the lack of morbidity caused by a donor site operation. However, significant resorption of the graft material has been reported if the graft material is exposed. Resorption can reduce the possibility of complete root coverage because the main target area for coverage is always the coronal portion, which is the same as the exposed area of the graft materials. Furthermore, evidence is lacking whether the coronal portion of tissue substitutes remains stable in the long term. As these grafts or tissue substitutes are usually located at the coronal portion to cover the exposed root surface, the outline and tissue thickness of the apical base is often neglected. Here, periodontal biotypes need to be considered.
The term “periodontal biotype” was first introduced by Seibert and Lindhe [16] in 1989. Unlike the term “gingival biotype,” it includes several related morphologic characteristics of the bone, teeth, and periodontium, as well as gingival thickness [17]. These biotypes are thought to influence the outcomes of periodontal therapy, prosthodontic work, implant therapy, and root coverage procedures [18]. A higher risk of gingival recession was reported after the same periodontal therapy or implant therapy in patients with the thin periodontal biotype than in those with the thick biotype [19]. Most clinicians who scrutinize patients' periodontal areas will agree that a large portion of gingival recession patients have a thin periodontal biotype. Therefore, the ability to change this delicate and thin biotype into a more durable biotype would be of paramount importance, not only for the outcomes of exposed root coverage procedures, but also for long-term stability and the prevention of recurrence.
The aim of this case series was to suggest a technique for periodontal biotype modification through thickening of the entire facial aspect using a volume-stable collagen matrix and autogenous subepithelial CTG for the treatment of gingival recession.
CASE DESCRIPTION
Study design
Four systemically healthy patients (all female patients) aged between 25 and 60 years (mean age, 36.8±17.7 years) with localized or multiple areas of gingival recession were included in this study. All subjects were referred to the Department of Periodontics, Seoul National University Dental Hospital and were included in the study after providing informed consent following a detailed explanation of the entire procedure. The study protocol was approved by the Institutional Review Board of Seoul National University Dental Hospital (approval No. CDE16002 and CDE18004).
Patient selection
The patient selection criteria were as follows: 1) Miller class I or class II gingival recession, with the deepest gingival recession ≥1 mm on the facial aspect of the mandibular incisors, 2) a probing depth ≤3 mm, 3) tooth vitality, 4) absence of dental caries or restorations in the area to be treated, 5) systemically healthy status, and 6) nonsmoking. The demographic characteristics of all subjects and information related to the teeth with gingival recession are shown in Table 1.
Table 1
Demographic characteristics of all subjects and information related to the teeth with gingival recession

| Case No. | Age/sex | Tooth No. (FDI) | MC | REC (mm) |
|---|---|---|---|---|
| Case 1 | 41/F | #31 | Class II | 6 |
| Case 2 | 60/F | #31, #32, #41 | All class I | 2.5, 2, 1 |
| Case 3 | 25/F | #41 | Class I | 1.5 |
| Case 4 | 21/F | #31 | Class II | 3 |
FDI: Federation Dentaire Internationale, MC: Miller classification, REC: recession depth of each tooth, F: female.
![]()
Presurgical therapy
All patients were given instructions for proper oral hygiene. Full-mouth scaling and root planing (SRP) procedures were performed at least 4 weeks prior to periodontal plastic surgery. A periodontal examination was performed 4 weeks after SRP, and adequate plaque control (full-mouth plaque score ≤20%) and absence of gingival inflammation (full-mouth bleeding score ≤20%) at the time of the surgery were ensured in all patients.
Surgical procedures
The periodontal biotype modification procedures in cases 1–3 were performed by a single experienced operator (KS) using an identical technique. After rinsing with 0.1% chlorhexidine gluconate (Hexamedine Solution, Bukwang Pharm Co., Seoul, Korea) for 1 minute, the surgical field (the mandibular incisor area, including the ipsilateral palate) was anesthetized by 2% lidocaine with 1:100,000 epinephrine (Lidocaine, Huons, Seongnam, Korea). A horizontal intrasulcular incision extending to both mandibular canines was made on the labial side, followed by 2 vertical incisions placed at the mesial line angles of the canines. A split-thickness flap was elevated beyond the mucogingival junction to the apical aspect around the tooth with recession and the adjacent teeth. All exposed root surfaces were debrided thoroughly and the papillae were de-epithelized. A double-layered volume-stable collagen matrix (Collagen graft, Dentium, Seoul, Korea) was placed on the apical part of the recession area broadly and stabilized by a cross-sling suture and interrupted suture using 5-0 resorbable suture material (Vicryl Rapide, Ethicon, Somerville, NJ, USA). A subepithelial CTG was harvested from the palatal area using the technique suggested by Hürzeler and Weng [20]. The CTG was placed on the coronal part of the recession area, properly covering the denuded root surface, and was firmly sutured using the same suture technique and materials that were used for the stabilizing collagen matrix. The flap was allowed to cover the grafts, with coronal advancement to 1 mm above the cementoenamel junction, and stabilized by an interrupted suture along the vertical releasing incision and a double-sling suture anchored to the lingual cingulum on the interdental papilla area, using 6-0 non-resorbable monofilament suture material (Ethilon). Surgical dressing materials were not used in any cases.
In case 4, a slightly modified surgical procedure was applied by the same operator (KS). Unlike the previous consecutive cases, all intrasulcular incisions were made independently, and the vertical incisions were not extended to the gingival margin area. Facial soft tissue was then subperiosteally dissected through the incomplete vertical incisions, keeping the interdental papillae intact. These papillae were also elevated for coronal mobilization of the mucogingival complex. Once the recipient bed was prepared, volume-stable collagen matrix was inserted into the apical part of the prepared tunnel through the vertical incisions, followed by CTG placement into the coronal part of the tunnel. The coronal CTG was completely covered by advancing the entire facial mucogingival complex, using interrupted sutures along the vertical incisions and double-sling sutures on the interdental papilla with 5-0 resorbable suture material (Vicryl Rapide, Ethicon). As in the previous cases, no surgical dressing materials were used.
Postsurgical care
Patients were advised not to brush the surgical site and to rinse with 0.1% chlorhexidine digluconate twice a day for 2 weeks. Antibiotics and analgesics were prescribed postoperatively for 3 days. Sutures were removed after 2 weeks. Patients were instructed to resume mechanical tooth cleaning with a soft toothbrush at 2 weeks after surgery. The patients were followed up at 2 weeks, 3 weeks, and 3 months after surgery. At each follow-up visit, oral hygiene instructions were given and a professional cleaning was performed.
Assessment of volumetric changes
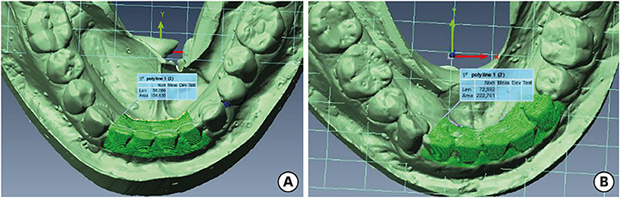
In cases 1 and 2, the facio-lingual volumetric changes between the preoperative and 3-month postoperative time points were analyzed. Master casts were fabricated with dental stone (GC Fujirock EP, GC Co., Tokyo, Japan) utilizing irreversible hydrocolloid impression materials (Alginate GC Aroma Fine Plus, GC Co.). The casts were optically scanned using computer-aided design software (DentalCAD, EGS, Bologna, Italy) and a 3-dimensional (3D) optical scanner (DScan version 1.1, EGS), and then captured as stereolithographic (STL) files. After the STL files were imported into a 3D measurement software program (Polyworks, Innovmetric, Quebec, QC, Canada), the images from the 2 times points were superimposed and matched using the adjacent teeth as references. The region of interest was defined as extending from the top of the tooth structure to the vestibular area of 4 mandibular incisors in cases of localized single recession (Figure 1A) and the area of the tooth with recession and the adjacent tooth on both ends in cases of multiple recession (Figure 1B).
 | Figure 1Assessment of volumetric changes using stereolithographic files imported into a 3-dimensional measurement software program. (A) The ROI of case 1 showing localized gingival recession, defined as the area extending from the top of the tooth structure to the vestibular area of 4 mandibular incisors. (B) The ROI of case 2 showing multiple recession, defined as the tooth with recession and the adjacent tooth on both ends.ROI: region of interest.
|
Case 1
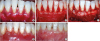
A 41-year-old female patient presented to the Department of Periodontics for the treatment of a recession defect for esthetic reasons. A gingival recession defect was shown in the Federation Dentaire Internationale (FDI) tooth #31 area with a clinical attachment loss (CAL) of 6 mm, corresponding to Miller class II recession. After completion of the initial periodontal therapy, the periodontal biotype modification technique using a volume-stable collagen matrix and autogenous subepithelial CTG combined with CAF was performed as described above. Healing was uneventful and complete coverage of the defect was maintained for 3 months (Figure 2). At a 3-month follow-up, the analysis of STL files showed that the patient's facio-lingual volume had increased after the operation (Table 2).
 | Figure 2Clinical photographs of case 1. (A) Presurgical view of the recession. A gingival recession defect was observed in the FDI tooth #31 area with CAL of 6 mm, corresponding to Miller class II recession. (B) The exposed root at the time of surgery. (C) Collagen matrix placement on the apical part and CTG placement on the coronal part of the recession area. (D) Three weeks after surgery. (E) Three months after surgery.FDI: Federation Dentaire Internationale, CAL: clinical attachment loss, CTG: connective tissue graft.
|
Table 2
Assessment of the volumetric changes of the matched ROI between preoperative and 3-month postoperative time points

ROI: region of interest, M: months, FDI: Federation Dentaire Internationale.
a)The ROI was determined based on included tooth number (FDI); b)Positive values indicate an increase of the dimension.
![]()
Case 2
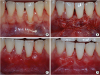
A 60-year-old female patient complaining of exposed roots of the mandibular incisors presented to the Department of Periodontics for the treatment of gingival recession. Miller class I gingival recession was found in the FDI teeth #31, #32, and #41 areas, with CALs of 2.5, 2, and 1 mm, respectively. The same periodontal biotype modification technique was performed and healing was uneventful. Complete coverage of the gingival recession areas was achieved and maintained for 3 months (Figure 3). At a 3-month follow-up, volumetric measurements showed that the facio-lingual volume of the ROI had increased compared to the matched ROI from before the operation (Table 2).
 | Figure 3Clinical photographs of case 2. (A) Presurgical view of the recession. Miller class I gingival recession was observed in the FDI teeth #31, #32, and #41 areas, with CAL of 2.5, 2, and 1 mm, respectively. (B) Collagen matrix placement on the apical part of the recession area. (C) CTG placement on the coronal part of the recession area. (D) Three weeks after surgery. (E) Three months after surgery.FDI: Federation Dentaire Internationale, CAL: clinical attachment loss, CTG: connective tissue graft.
|
Case 3
A 25-year-old female patient presented with a tooth that showed a Miller class I gingival recession defect in the FDI tooth #41 area with a CAL of 1.5 mm. After undergoing the periodontal biotype modification technique described above, complete coverage of the defect was achieved and well maintained for 3 months (Figure 4).
 | Figure 4Clinical photographs of case 3. (A) Presurgical view of the recession. Miller class I gingival recession defect in the FDI tooth #41 area with CAL of 1.5 mm. (B) Collagen matrix placement on the apical part of the recession area. (C) CTG placement on the coronal part of the recession area. (D) Three weeks after surgery. (E) Three months after surgery.FDI: Federation Dentaire Internationale, CAL: clinical attachment loss, CTG: connective tissue graft.
|
Case 4
A 21-year-old female patient had a chief complaint of receding gums in the mandibular incisor area. On examination, Miller class II gingival recession was found in the FDI tooth #31 area with a CAL of 3 mm. After treatment with the periodontal biotype modification technique using a slightly modified surgical procedure as described above, reduction of the gingival recession area was observed at 3 months after surgery (Figure 5).
 | Figure 5Clinical photographs of case 4. (A) Presurgical view of the recession. Miller class II gingival recession was shown in the FDI tooth #31 area with CAL of 3 mm. (B) Collagen matrix and a CTG were placed through the incomplete vertical incisions in the apical part and in the coronal part of the recession area, respectively. (C) Three weeks after surgery. (D) Three months after surgery. Reduction of the gingival recession was observed.FDI: Federation Dentaire Internationale, CAL: clinical attachment loss, CTG: connective tissue graft.
|
DISCUSSION
The aim of this case series was to suggest a technique for periodontal biotype modification through thickening of the entire facial aspect using a volume-stable collagen matrix and autogenous subepithelial CTG for the treatment of gingival recession. Three cases using the same surgical technique and 1 case using a slight modification of that technique were presented in this study to establish this technique as an effective method for periodontal biotype modification. Complete root coverage was accomplished in the first 3 cases, and an increase of the entire facio-lingual volume was demonstrated by comparing STL files from before the operation and 3 months after the operation in 2 cases, suggesting that periodontal biotype modification was successfully achieved.
The periodontal biotype of periodontal plastic surgery patients has been regarded as an important factor in making decisions about treatment plans and for predicting treatment outcomes. Although there are no specific criteria for determining the periodontal biotype, modification of the thin and vulnerable biotype to the thick and durable one can optimize the outcomes of periodontal plastic surgery and potentially reduce the risk of relapse of mucogingival problems. As the periodontal biotype may vary according to dental arch location or tooth position even in a single person [21], we limited the cases to mandibular incisors in the present study. To determine that the periodontal biotype had been modified, we analyzed facio-lingual volume changes in cases 1 and 2 using a 3D measurement software program. The assessment of volume changes using STL models and 3D measurement software is a very promising technique in the field of dental research. Once the digitized data are properly positioned and oriented in 3D, the dimensions of interest can be easily extracted from the measured polygonal models built from probed points, facilitating the volumetric analysis of the specific area. As the lingual side was barely modified, the increase in volume was related to the entire facial aspect. The CTG on the coronal part showed a high survival rate of graft tissue. Moreover, the placement of a volume-stable collagen matrix on the apical part can support the apical base, giving more physiologic morphology and less possibility for exposure than using a CTG alone. These thickened and physiologically contoured facial aspects can facilitate oral hygiene behaviors and act as a durable barrier against various types of trauma that could cause the relapse of mucogingival problems.
The technique used in cases 1–3 enabled better visualization of the denuded root surface with less tension, and provided more information about it, because it involved 2 conventional vertical incisions on both ends. The CAF was introduced by Allen and Miller [22] and became popular after several combined techniques were suggested using tissue grafts, tissue substitutes, or bioactive agents [23]. It has been reported that the use of a CAF combined with CTG or collagen matrix grafting led to a higher probability of achieving complete root coverage compared to other different flap designs or other combinations [24].
However, the CAF technique also demonstrated some limitations, including the formation of unaesthetic scars, decreased papillary gingival volume, and recession of the adjacent tooth. To overcome these drawbacks, a slightly modified surgical protocol was applied in case 4. In this case, recipient bed preparation was based on the tunnel technique introduced by Allen [25]. Instead of a supraperiosteal envelope, multiple incomplete vertical incisions were made to facilitate undisturbed subperiosteal dissection and the insertion of graft materials. Preserving the anatomical integrity of the interdental papillae could minimize papilla loss and tooth recession in response to conventional vertical incisions.
In every periodontal plastic surgical procedure, the importance of good oral hygiene cannot be overemphasized. Favorable oral hygiene enables precise incisions, flap management, and clean closure, minimizing the risk of infection [2627]. In this study, periodontal examinations were performed 4 weeks after SRP, and adequate plaque control (full mouth plaque score ≤20%) and absence of gingival inflammation (full mouth bleeding score ≤20%) at the time of periodontal plastic surgery were ensured in all patients, as suggested by Lang et al. [28].
There were some limitations in this study. The small number of subjects and short follow-up period should be addressed by conducting a well-designed randomized prospective clinical study. Moreover, the number of STL models should be large enough to conduct a statistical analysis. Although much remains to be done, the present study underscores the importance of periodontal biotypes for periodontal plastic surgery patients. The surgical technique proposed in this study using a volume-stable collagen matrix and autogenous subepithelial CTG may be an effective method for periodontal biotype modification through thickening of the entire facial aspect for the treatment of gingival recession.
 XML Download
XML Download