

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The clinical significance of bone regeneration is rapidly expanding with the recent increase in patients requesting dental implant treatment. To assess regenerative materials such as bone graft materials and barrier membranes after ex vivo testing, animal studies are usually performed [1]. Preclinical studies in animals can reproduce various conditions, including systemic diseases [2]. However, the exact protocol of such animal studies for systemic diseases such as diabetes mellitus (DM) has not yet been established.
DM is a chronic metabolic disorder that has been found to impair osseointegration and bone regeneration. It is characterized by hyperglycemia, resulting from defects in insulin secretion, insulin action, or both [3]. Type 1 DM is an absolute deficiency of insulin secretion, caused by autoimmune destruction of the insulin-producing β-cells of the pancreas. Type 2 DM involves impaired insulin function, such as resistance to insulin action, along with an insufficient compensatory insulin secretion response. In 2013, approximately 2.7 million Korean adults (8.03%) aged 30 years or more were found to have type 2 diabetes, and 25.0% of adults had prediabetes [4]. In addition, the prevalence of type 2 diabetes in people aged 60 years or older has been steadily increasing.
The complications of DM include problems associated with bone metabolism. Alteration of mineral homeostasis, osteoid production, and bone formation has been demonstrated in previous experimental diabetic models [567]. Goodman and Hori [5] described decreased osteoid formation in diabetic rats. Moreover, diabetic rats showed a longer osteoid mineralization lag time than control rats. The biological effects of DM on osseointegration have been evaluated in clinical studies [89]. In a prospective study to determine whether type 2 DM was a risk factor affecting the long-term clinical outcomes of dental implants [8], 255 implants were placed in type 2 DM patients, and a significantly high failure rate was found. Moy et al. [9] performed a retrospective cohort study to evaluate the hypothesis that coexisting conditions such as smoking, DM, and radiation therapy lead to increased rates of implant failure. Among 1,140 patients with 4,680 implants placed, 48 patients had DM, and they showed a failure rate of 31.25%. Thus, DM patients presented a higher relative risk of failure than healthy controls. In a preclinical study, Nevins et al. [10] observed less bone–implant contact in rats with chemically-induced diabetes than in the control group. Giglio et al. [11] reported retarded peri-implant bone healing in rats with chemically induced diabetes. Retrospective human studies also showed that DM affected implant osseointegration by impairing osseous wound and bone healing, decreasing bone density, and increasing fracture risk and susceptibility to periodontal disease [1213].
The mechanism through which DM results in impaired osseous healing is not yet clear; however, some possible pathogenic pathways have been suggested, including hyperglycemia. In ex vivo studies, osteoblastic cells subjected to elevated glucose concentrations exhibited irregular bone mineral nodule formation and a suppressed cell-growth rate [1415]. Non-enzymatic protein glycation occurs in diabetes, leading to the formation of various chemically modified proteins known as advanced glycation end products (AGEs) [16]. Santana et al. [17] found that the accumulation of AGEs in bone contributed to diminished bone healing in type 1 diabetes, possibly mediated by receptor for advanced glycation end products (RAGE). A plausible mechanism is that AGE–RAGE interactions may result in the activation of nuclear factor-kappa B (NF-κB) in osteoblastic cells [18].
Many complications of diabetes, such as neuropathy and vascular diseases, are associated with the duration of DM [19202122]. Although a few animal studies on the effects of chemically-induced diabetes on bone defect healing have shown impaired healing of bone defects in diabetic animals [172324], to our knowledge, none of those studies established a protocol for assessing the association between the duration of diabetes and the extent of impairment of bone-healing capacity. Therefore, the purpose of this study was to examine the association between the duration of diabetes and its effect on bone-healing capacity in rabbits, and to establish an optimal experimental protocol for evaluating the bone-healing capacity of diabetic animals using cone-beam computed tomography (CBCT), histologic analysis, and immunofluorescence analysis.
MATERIALS AND METHODS
Experimental animals
Male New Zealand white rabbits (10–14 weeks, 2–3 kg) were purchased from Samtako (Osan, Korea). The animals were housed in conventional conditions, including room temperature (23°C), controlled humidity (60%), a 12-hour light/12-hour dark cycle, and ad libitum access to food and water. Twenty-four young male New Zealand white rabbits were divided into 4 groups, including a control group. Before any experimental manipulations, the rabbits were allowed to acclimate for at least 7 days. The study was conducted with approval of the Institutional Animal Care and Use Committee of Gangneung-Wonju National University (approval No. GWNUA-2015-37). All experiments were performed in a way that minimized the number of animals used and the distress caused by the procedures used in this study.
Study design
To evaluate the association between the duration of diabetes and bone-healing capacity, the experimental groups (groups 1, 2, 3) were organized according to the duration of diabetes. Bone defects were introduced at 1, 2, and 4 weeks after DM induction in groups 1, 2, and 3, respectively. The rabbits in the control group underwent bone defect surgery without DM induction. CBCT (Alphard Vega 3030, Asahi, Fukuoka, Japan) was performed in all groups on the day of surgery, 2 weeks after surgery, and 4 weeks after surgery. After the last CBCT scan, the rabbits were sacrificed.
Alloxan-induced diabetic rabbit model
For DM induction, alloxan monohydrate (ALX; Sigma Aldrich Co., St. Louis, MO, USA) was dissolved in 5 mL of sterile saline with a final concentration of 100 mg/kg, and was administered intravenously for 5 minutes via the marginal ear vein of rabbits in the experimental groups. The rabbits showing fasting blood sugar (FBS) levels higher than 200 mg/dL at 1 week after injection were classified as diabetic. FBS readings were taken 1 week later, using a blood glucose test meter (Roche, Basel, Switzerland) after 12 hours of fasting.
Surgical procedure
For bone defect induction, rabbits were anesthetized with isoflurane (Hana Pharm Co., Hwaseong, Korea). With a sharp blade and periosteal elevator, full dissection was done to expose the calvaria. Four circular bone defects with a diameter of 5 mm were created on frontal and parietal bone sites bilaterally in each rabbit using a trephine burr under saline irrigation. The surgical site was closed by bilayer suturing using 4-0 black silk (Ailee, Busan, Korea). All animals received an intramuscular injection of cefazolin (30 mg/kg) for 2 days to prevent postsurgical infection.
CBCT scanning and gray level unit (GLU) measurements
In the experimental and control groups, CBCT was performed under isoflurane anesthesia to evaluate the process of bone defect healing at 3-time points: just after surgery, 2 weeks later, and 4 weeks later. The exposure settings for the scans were as follows: voxel size,100 µm; tube current, 5 mA; tube voltage, 80 kV; and scan time, 17.0 seconds. To evaluate bone healing and mineralization, the GLUs of the bone defects were measured. The region of interest was set on the top of the bone defect margin in a circle with a diameter of 6 mm. The mean GLUs were recorded and statistically analyzed.
Tissue processing for histological analysis
Four weeks after surgery, the rabbits were sacrificed. For the histological analysis, the animals were anesthetized with isoflurane and perfused transcardially with 0.1 M phosphate-buffered saline (PBS; pH 7.4) followed by 4% paraformaldehyde in 0.1 M phosphate buffer (pH 7.4). The frontal and parietal bones were retrieved and postfixed in the same fixative for 6 hours. The fixed tissues were decalcified with Decalcifying Solution-Lite (Sigma Aldrich Co.) for 12 hours at room temperature. The decalcifying process was completed after confirming that the bone was cut with a blade. The decalcified tissues were washed with running tap water and dehydrated by immersion for 2 hours in 50%, 70%, 80%, 90%, 95%, and 100% ethanol baths in succession at room temperature. Next, the tissues were placed twice for an hour each in fresh pure xylene and then in molds containing melted paraffin (Histowax, Leica, Wetzlar, Germany). Serial 5-μm-thick transverse sections were cut and mounted on saline-coated microscopy slides.
Histological analysis
Masson trichrome stain
A trichrome stain kit (Abcam, Cambridge, UK) was used. Specimens were washed twice with xylene for 10 minutes to remove the paraffin. Deparaffinized sections were treated with Bouin's fluid for 60 minutes and cooled for 10 minutes, followed by treatment with Weigert's hematoxylin for 5 minutes. Sections were washed in running water for 2 minutes. Then, sections were stained in Biebrich scarlet-acid fuchsin solution for 15 minutes and rinsed in distilled water (DW). Finally, the slides were placed in phosphomolybdic-phosphotungstic acid solution for 10 minutes, transferred into aniline blue solution for 5 minutes, and placed in 1% acetic acid solution. The slides were washed, dehydrated, and sealed in Canada balsam (Kanto Chemical, Tokyo, Japan) and then observed under a light microscope (Leica).
Hematoxylin/eosin staining
Sections were deparaffinized and hydrated using the conventional process. After hydration, slides were washed in DW for 10 minutes. The slides were then stained with Harris hematoxylin for 8 minutes, washed in running water, and placed in 1% acid alcohol for 30 seconds. After washing, the slides were placed in 0.5% ammonia in water and washed in water. Then, the slides were stained with eosin for 1 minute and placed in 95% alcohol for 10 minutes. The slides were placed in 100% ethanol twice for 10 minutes each, and then in xylene twice for 10 minutes each. Finally, the slides were sealed with Canada balsam and observed under a light microscope (Axio Imager A2, Zeiss, Jena, Germany).
Immunofluorescence analysis and optical density measurements
An immunofluorescence analysis was performed to identify the appearance of osteoprotegerin (OPG) and receptor activator of NF-κB (RANKL). Sections were placed in xylene twice for 10 minutes each. After deparaffinization, sections were placed in 100% alcohol twice, and hydrated using the conventional hydration process. Sections were washed in PBS buffer thrice. Antigen retrieval was then performed by treating slides for 5 minutes in a microwave with citric acid buffer (pH 6.0). After sections were washed with PBS buffer, they were incubated at 4°C with goat anti-RANKL antibody (diluted 1:200) and mouse anti-OPG antibody (diluted 1:200) overnight. The slides were washed in PBS buffer and incubated in room temperature for 90 minutes with donkey anti-mouse 488 IgG for OPG and donkey anti-goat 546 IgG for RANKL. The slides were dried in an oven, placed in xylene for 1 minute, and sealed in the permount. The immunoreactions were observed under a light microscope (Axio Imager A2, Zeiss) attached to a fluorescent lamp (HBO 100 illuminator, Zeiss) and a charge-coupled device camera (Aziocam 506, Zeiss).
A densitometric analysis to quantify the immunoreactivity of OPG and RANKL was performed by determining the relative optical density (ROD) using Scion ImageJ (National Institutes of Health, Bethesda, MD, USA). The ROD was calculated as a percentage, and the ROD of the control group was designated as 100%.
Statistical analysis
The total sample size of 24 was calculated using the G*Power program on the basis of an effect size of 0.25, a type I error of 0.05, a power of 0.80, and the presence of 4 groups in 1-way repeated-measures analysis of variance. Six samples per group were required.
Non-parametric analysis of variance for repeated measures (the Friedman test) was performed to evaluate changes in GLUs among groups. The Wilcoxon signed-rank test was also performed for pairwise comparisons of time points within each group. The significance of multiple comparisons was adjusted using the Bonferroni method. Data are presented as the mean±standard deviation. P values less than 0.05 were considered to indicate statistical significance. All statistical analyses were performed using a software package for statistical analysis (SPSS version 23, IBM Corp., Armonk, NY, USA; Microsoft Excel, Microsoft, Redmond, WA, USA).
RESULTS
Alloxan-induced diabetic rabbits
Of the 22 experimental rabbits, 9 died within 7 days, 5 failed to show elevated blood glucose levels, and 2 died during bone defect surgery. Six rabbits showed elevated blood glucose levels, and were distributed into 3 experimental groups (groups 1, 2, and 3), each comprising 2 rabbits with DM. The rabbits underwent bone defect surgery 1, 2, and 4 weeks after DM induction, respectively. The control group comprised 2 rabbits without DM, which were subjected to bone defect surgery. Eight specimens per group were obtained. On the day of diabetes induction, the mean FBS levels were 149.63±19.38 mg/dL in the diabetic rabbits. FBS levels increased over time, reaching over 500 mg/dL by 4 weeks after the injection. The mean FBS level of diabetic rabbits at 4 weeks after DM induction was 554.75±29.94 mg/dL. The diabetic state of all diabetic rabbits was well-maintained throughout the experimental period (Figure 1).

CBCT scanning, GLU measurements, and 3-dimensional (3D) imaging
Table 1 shows the GLU levels of the groups. The control group showed a mean GLU of 326.25±64.27 at baseline, 685.88±175.56 at 2 weeks after surgery, and 915.25±274.37 at 4 weeks after surgery. Group 1 showed a mean GLU of 460.25±58.19 at baseline, 438.88±141.64 at 2 weeks after surgery, and 463.00±215.74 at 4 weeks after surgery. Group 2 showed a mean GLU of 345.38±107.90 at baseline, 322.25±151.61 at 2 weeks after surgery, and 529.38±125.77 at 4 weeks after surgery. Group 3 showed a mean GLU of 331.00±45.41 at baseline, 589.13±174.01 at 2 weeks after surgery, and 530.88±197.48 at 4 weeks after surgery. The change in GLU showed a significant relationship with the experimental group (i.e., to the time elapsed), and the GLU values of the control group were significantly different from those of the 3 experimental groups (P<0.001). However, no significant difference was observed among groups 1, 2, and 3. On reconstructed 3D imaging, the control group showed evident bone regeneration, while groups 1, 2, and 3 showed relatively slow bone healing (Figure 2).
Table 1
Gray level units obtained from cone-beam computed tomography

Data are shown as mean±standard deviation.
a,b,c)The same superscript letters indicate values that are not significantly different (P>0.05).
![]()

Histological analysis
For a morphological analysis of bone defect areas, bone sections were stained with hematoxylin and eosin (H&E) and Masson trichrome. In the control group, the bone defect area was mostly filled with bone tissue (regenerated bone) stained with H&E or Masson trichrome. However, in groups 1, 2 and 3, there was significantly less regenerated bone in the bone defect areas than in the control group. In the experimental groups, the defect areas were mainly filled with connective tissue (Figure 3).
 | Figure 3Hematoxylin and eosin staining and Masson trichrome staining of specimens (scale bae=1 mm). The control group (B) showed notable bone regeneration, whereas groups 1 (C), 2 (D), and 3 (E) showed scarce bone regeneration. (A) baseline. Black arrowheads indicate defect margin.CTL: control, DM: diabetes mellitus, W: weeks.
|
Immunofluorescence analysis
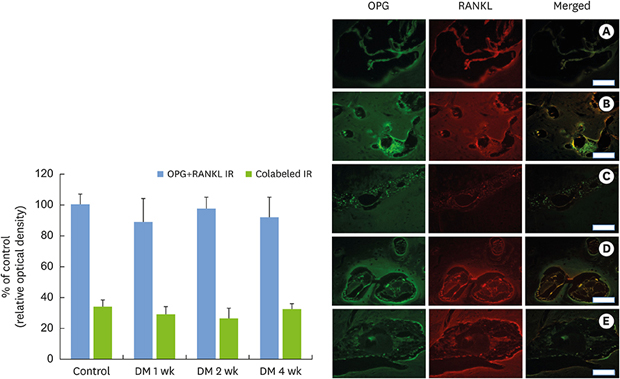
To identify the activated osteoclasts in the bone defect margin, double immunofluorescence staining for RANKL and OPG was performed. In all experimental groups, RANKL and OPG immunoreactivity was observed around the Howship lacuna. However, relative to the optical density of the control samples, RANKL, OPG, and RANKL/OPG immunoreactivity did not show any remarkable change (Figure 4).
 | Figure 4Immunofluorescence analysis of OPG and RANKL, as well as merged images (Scale bar = 25 um). There were no obvious differences among the groups. The relative optical density was derived from the immunofluorescence analysis. No statistically significant difference was shown among groups. (A) baseline, (B) control group, (C) group 1, (D) group 2, (E) group 3.OPG: osteoprotegerin, RANKL: receptor activator of nuclear factor-kappa B, CTL: control, DM: diabetes mellitus, IR: immunoreactivity, W: weeks.
|
DISCUSSION
We evaluated the association between the duration of DM and bone-healing capacity using an experimental diabetic rabbit model, and found that DM duration over 1 week could impair bone-healing capacity to some extent. However, we did not identify a link between the magnitude of bone healing impairment and the duration of DM. Since the levels of OPG and RANKL did not significantly differ among groups, osteoclast activity might not contribute to the alteration of bone metabolism in DM.
ALX is one of the most commonly used chemical agents for the induction of DM, and it is used for experimental DM in animals such as rabbits, rats, mice, and dogs. ALX has 2 distinct pathological effects: selective inhibition of glucose-induced insulin secretion through specific inhibition of glucokinase—the glucose sensor of β-cells—and induction of a state of insulin-dependent DM by the induction of reactive oxygen species formation, leading to selective necrosis of β-cells [25]. The major disadvantages of ALX are variability in the response to DM induction and systemic toxicity [26]. Susceptibility to both toxic and diabetogenic doses of ALX varies widely not only across different species, but also among animals of the same species [27]. In our study, the lethality of 100 mg/kg ALX was 52.6%, and the success rate of DM induction was 36.4%. In the literature, lethality rates of 25%–83% and success rates of 16%–50% have been demonstrated with the same dose of ALX [2829]. When considering both the lethality rate and the DM induction success rate, the dose applied in this study can be regarded as acceptable. This study required 6 samples per group, but only 8 of the 24 rabbits survived. We created 4 bone defects per rabbit to obtain an adequate number of samples.
To evaluate bone healing in live diabetic rabbits in real time, we used GLUs obtained by CBCT measurements. A GLU is a value assigned to the voxels in CBCT. GLUs are not the same as Hounsfield units (HUs), which provide a quantitative assessment of bone density; however, Mah et al. [30] demonstrated that GLUs had a linear relationship with attenuation coefficients, and that HU values could be calculated from GLU values. The GLU values of the control group significantly differed from those of groups 1, 2, and 3. Moreover, since the appearance of GLUs at 4 weeks after surgery corresponded with the histological appearance to some extent, GLUs can be regarded as a practical means to quantify and assess bone healing.
Since an objective of this study was to establish an optimal protocol for the evaluation of the bone-healing capacity of diabetic animals, we studied the effect of varying intervals between DM induction and bone defect induction. As hyperglycemia is usually confirmed 1 week after DM induction, the shortest interval was set at 1 week. Two preclinical studies evaluated the effect of chemically-induced DM on bone-healing capacity [1724]. Both studies evaluated the extent of damage to bone healing caused by DM depending on the size of cranial defects created about 3 weeks after DM induction, and demonstrated altered bone healing in diabetic animals. Designation of the precise duration of DM before surgical intervention that would be most suitable for expressing alterations in bone healing would be helpful for minimizing the experimental period and planning optimal schedules in future animal studies.
As can be seen in the 3D images obtained by CBCT and through the histological analysis, an interval of at least 1 week between DM induction and the intervention was sufficient for DM to exert a harmful effect on bone healing. Although there were some variations among the sites, bone regeneration was generally much more prominent in the control group than in groups 1, 2, and 3. Most of the regenerated bone was located on the top of the defect, and was misshapen owing to the protrusion of intracranial tissue into the bone defect [31]. Careful effort not to damage the dura mater during bone defect induction would minimize this phenomenon.
In the immunofluorescence analysis, the ROD of OPG and RANKL did not significantly differ among groups. OPG and RANKL have been identified as components of a ligand–receptor system that directly controls osteoclast differentiation and bone resorption. RANK is the cognate receptor of RANKL, and is expressed at high levels in osteoclast precursors [32]. The coupling of RANK and RANKL activates the formation and maturation of osteoclasts [33]. OPG works as a decoy receptor of RANKL and hinders the activation of RANK by selectively binding to RANKL, thereby protecting bone against destruction [34]. For these reasons, OPG and RANKL are considered good markers of osteoclast activity. Our results suggest that altered osteoclast activity does not contribute to altered bone metabolism in DM. In future studies, examination of other possible factors, like osteoblast activity, can be recommended.
New Zealand white rabbits were used in the present study. Many animal studies on DM have used rats as experimental animals. One disadvantage of rodents as experimental animals is that, due to their short life span, they may not develop the clinical complications that manifest in humans under long-term diabetic conditions [35]. In addition, calvarial bone and the other bones of rats are very small, making surgical interventions relatively difficult. Rabbits, however, are adaptable animals for prolonged-duration DM studies [36]. Rabbits are known to have suitable characteristics for experimental animals, such as appropriate size, a longer life span than small rodents, strain specificity, good temper, maneuverability, and relatively low cost [37]. In our study, all the diabetic rabbits survived and maintained elevated FBS throughout the experimental period. This demonstrates the viability and ease of handling of rabbits in DM animal models. Furthermore, the diabetic rabbit model can be used for implant studies due to the sufficient bone volume of the rabbit tibia.
We demonstrated that bone healing slowed when the interval between DM induction and surgical intervention was longer than 1 week. However, we failed to show a relationship between the extent of bone healing impairment and the duration of DM. Some limitations of this study, such as the small number of samples, relatively short period of the study, and high lethality and toxicity of ALX, might have been responsible for this outcome. The dose of ALX used in this study yielded relatively acceptable results; however, further research is needed to determine more precisely the dose of ALX that would maximize the success rate of DM induction and minimize lethality. A role of osteoclasts in altered bone metabolism was not evident. Other possible factors that would reveal the exact mechanisms affecting bone healing in DM should be considered in future studies.
Taken together, the dose of 100 mg/kg of ALX seems to have been an acceptable dose for DM induction in rabbits, and effects of DM on bone healing were demonstrated when the interval between DM induction and intervention was at least 1 week. However, osteoclast activity might not be responsible for altered bone metabolism in DM.
 XML Download
XML Download