

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An increasing number of studies have demonstrated an association between periodontitis and rheumatoid arthritis (RA) based on their similar inflammatory pathogenesis. Both multifactorial diseases involve chronic inflammation activated by pro-inflammatory cytokines, connective tissue breakdown, and bone erosion. They also share genetic and environmental risk factors. Periodontitis is a chronic infectious disease characterized by an irreversible loss of connective tissue attachment and alveolar bone [1]. Periodontitis is diagnosed by evaluating information collected during a periodontal examination, including demographic information, medical history, previous and current periodontal problems, periodontal pocket probing, radiographic findings, and intraoral clinical features or observations. Supplemental assessments of the gingival crevicular fluid and subgingival microflora can also be performed to provide additional information [2]. RA is a chronic destructive inflammatory disease characterized by the accumulation and persistence of an inflammatory infiltrate in the synovial membrane, leading to synovitis and joint architecture destruction [3]. The diagnosis of RA is based on the clinical manifestation, physical examination, and serologic analysis, including erythrocyte sedimentation rate (ESR) and serum C-reactive protein (CRP) and rheumatoid factor (RF) levels. Radiographic techniques can also be used to assess various joints [4]. Recently, Kaur et al. [5] summarized several hypotheses regarding the association of the 2 diseases in a systematic review. One of the hypotheses, the “two-hit” model, suggested that a primary “hit” of chronic inflammation via chronic periodontitis, followed by a secondary arthritogenic “hit” to induce RA, can aggravate the inflammatory response [6]. Increased systemic inflammatory mediators in the circulation further stimulate resident cells in the synovium and the periodontium. Another hypothesis has been proposed regarding RA development via the humoral response to periodontal bacteria [7]. Porphyromonas gingivalis (Pg) is currently the only known periodontal bacterium that can citrullinate proteins and induce anticyclic-citrullinated peptide autoantibodies (anti-CCP antibodies), a key factor in RA development. The presence of Pg and its free-form DNA in synovial fluid supports the role of Pg in anti-CCP antibody and citrullination [8]. Citrullination occurs through the activity of an enzyme family known as peptidylarginine deiminases (PAD), of which Pg produces a variant [9]. The other hypothesis focuses on the common molecular pathways of the 2 diseases within the RANK/OPG/TRAIL axis, whereby decreased osteoprotegerin results in reduced vascular protection [10]. Increased RANKL and TRAIL levels in inflamed tissues may lead to progression of vascular damage and osteoclast activation, followed by subsequent bone damage. Based on the association of Pg and rheumatoid arthritis, several studies have evaluated the periodontal microbiological profiles in patients with and without RA. Ziebolz et al. [11] examined 11 different periodontal pathogenic bacteria, reporting that RF had no statistically significant influence on periodontal classification or on microbiological parameters. Schmickler et al. [12] also reported that there was an unclear interrelationship between periodontal pathogenic bacteria and rheumatoid parameters, and that the prevalence of all 11 periodontal pathogenic bacteria was similar in the RA and control groups.
Although numerous hypotheses and studies have investigated the causative relationship between RA and periodontitis, no clear explanation has been proposed regarding clinically useful diagnostic tools for other diseases. This study is essentially an extension of previous studies by Choi et al. [13] and Lee et al. [14]. Several cross-sectional studies were conducted jointly by the Department of Periodontology and the Department of Internal Medicine with the same participants to identify factors playing major roles in this association. Choi et al. [13] investigated the relationships of periodontal factors with the clinical manifestations of RA. The RA patients showed a higher prevalence of moderate-to-severe periodontitis than the control group. Periodontal indices of inflammation were correlated with RA disease duration, ESR, and anti-CCP antibodies, and the human leukocyte antigen DRB1 shared epitope was correlated with less periodontal structural damage in the RA patients. Lee et al. [14] focused on serum antibodies against Pg and human α-enolase (ENO1) titers in aspects of the humoral response. Both antibody titers were significantly higher in the RA group than in the control group and both showed correlations with periodontitis severity. Anti-Pg antibody titers in the RA group were significantly correlated with several periodontal indices. Anti-ENO1 antibody titers were significantly correlated not only with some periodontal parameters, but also with the clinical characteristics of RA. The present study further focused on microbiological periodontal profiles including Pg and their possible roles in RA and periodontitis. This study aimed at evaluating the relationship between RA and periodontitis and identifying the clinical significance thereof through a quantitative analysis of periodontal pathogens in a large sample of Korean adults. It was based on the hypothesis that individuals with RA would have a higher prevalence and larger amount of periodontal pathogens than those without RA. It was further hypothesized that there would be close associations of the RA indices with the periodontal indices and amount of periodontal pathogens.
MATERIALS AND METHODS
Participants
This was a prospective, cross-sectional study comparing RA patients with controls. The RA group included patients who satisfied the 1987 American College of Rheumatology classification criteria for RA at the rheumatology clinic of Seoul National University Hospital from May 2011 to February 2012. An age- and sex-matched control group of patients without arthritis was enrolled. In this study, the sample size was calculated using specialized software (Kane SP, Sample Size Calculator, Clincalc LLC). Clinical attachment level (CAL) was considered as the primary endpoint, with an expected difference of 1.0 mm and a standard deviation of 2.0 mm between the RA group and the control group. An α error probability of 0.05, a power of 90%, and an enrollment ratio of 3:1 (RA group to control group) were also assumed. As the result, the minimum sample sizes were calculated to be 168 and 56 for the RA group and control group, respectively. Participants who underwent periodontal treatment in the 3 months prior to the study, were pregnant, or had <15 teeth present were excluded in order to eliminate sources of bias. The Institutional Review Board and ethics committee approved the protocol (H-1103-151-357), and written informed consent was obtained from each participant prior to enrollment in the study.
Clinical and laboratory assessments
RA and baseline characteristics assessments
Overall, 295 patients were assessed by a rheumatologist at the rheumatology clinic of Seoul National University Hospital. Sociodemographic data, medical history, and comorbidities were collected for both groups. In the RA patients, we examined clinical parameters, including the 68-joint tender joint count (TJC), the 66-joint swollen joint count (SJC), and disease duration, and evaluated the serum erythrocyte sedimentation rate (ESR) and CRP levels. The disease activity score 28 (DAS28) was calculated as [0.56×√(28-TJC)+0.28×√(28-SJC)+0.70×ln(ESR)]×1.08+0.16 [15]. Concurrently, serum RF, anti-CCP antibody, and erosive radiographic changes were also measured.
Serologic analyses
Serologic analyses were performed in the RA laboratory for the RA group. The immunoturbidimetry method (Roche, Basel, Switzerland) was used to obtain the serum RF values, and a chemiluminescent microparticle immunoassay (Abbott, Lake Bluff, IL, USA) was performed to measure anti-CCP antibody values according to the manufacturer's instructions. An anti-CCP antibody titer >5 arbitrary units/mL was considered positive. The Pg strain FDC381 was grown and cultured in appropriate processes under anaerobic conditions (GasPak-EZ Anaerobe Container Systems, Becton Dickinson Microbiology Systems, Cockeysville, MD, USA) and the cells were extracted. In RA patients, 2-fold serial dilutions were added to the treated Pg cell plate, and bound human immunoglobulin G (IgG) was detected with horseradish peroxidase–conjugated anti-human IgG antibodies (Millipore, Billerica, MA, USA, 1/6,000 dilution), followed by a developer containing TMB (KPL, Gaithersburg, MD, USA). The anti-Pg antibody titer used the inverse value of the largest serial dilution for detectable antibody.
Periodontal clinical examination
Among the 295 RA patients, periodontal indices were evaluated in 264 patients by dentists specializing in periodontology. Individuals with <15 teeth or who were receiving ongoing dental care (n=29) were excluded due to the possibility of bias in evaluating the overall severity of periodontitis. The age- and sex-matched non-RA control group (88 volunteers) was also evaluated. The plaque index (PI), gingival index (GI), probing pocket depth (PPD), bleeding on probing (BOP), and clinical attachment level (CAL) were used as indices of periodontitis. The PI and GI were examined at 4 sites (mesio-, mid-, and disto-buccal points and a lingual point) on each tooth and graded as 1, 2, and 3; mean values were used for calculating the PI and GI [1617]. PPD was measured at 6 sites (mesio-, mid-, and disto-buccal points and mesio-, mid-, and disto-lingual points) on each tooth using a 15-mm University of North Carolina probe. BOP was assessed as positive or negative (represented as 1 or 0), and the mean value measured at 6 sites on each tooth was recorded as the percentage. The CAL, which is the distance from the cementoenamel junction to the base of the probable crevice, was calculated as the sum of PPD and the gingival recession. The mean value calculated at 6 sites on each tooth was used as the CAL for each patient, as CAL is a practical index of periodontitis severity. Periodontitis severity was defined as slight (CAL 1–2 mm), moderate (CAL, 3–4 mm), and severe (CAL ≥5 mm) according to the American Academy of Periodontology (AAP) classification [18]. And participants with a mean CAL ≥1 mm were considered to have periodontitis in this study.
Periodontal microbiological analyses
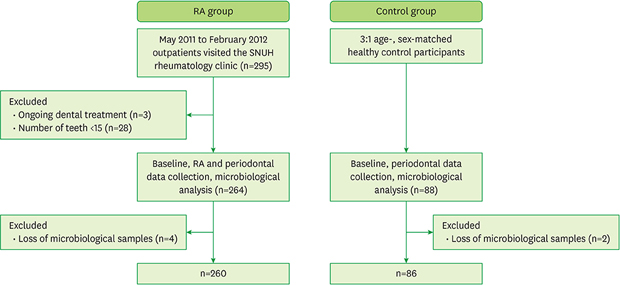
The 3 teeth with the highest PPD and the 2 deepest sites in each tooth were identified in every participant in both groups. After supragingival plaque removal, 6 subgingival biofilm samples were taken from each participant with sterile paper points and stored in a freezer at −80°C until analysis was performed. According to the classification of Socransky et al. [19], 9 different subgingival periodontal pathogens corresponding to red, orange, and green complexes were selected. The periodontal pathogens and their annealing temperatures are shown in Table 1. DNA was extracted using a commercially available DNA isolation kit. Real-time PCR assays and their standard curves were evaluated using a 7500 Real-Time PCR system (Applied Biosystems, Foster City, CA, USA) and 7500 software version 2.0.4 (Applied Biosystems) for quantitative analyses. In total, 4 patients from the RA group and 2 from the control group were excluded due to the loss of microbiological samples. The overall flowchart is shown in Figure 1.
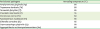
Table 1
The investigated periodontal pathogens and their annealing temperatures in real-time PCR
![]()

Statistical analyses
Variables were statistically analyzed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). The Student's t-test was performed for analyzing independent parametric variables, and the Mann-Whitney U test was used for analyzing independent nonparametric variables. The χ2 test or Fisher exact test was used to compare categorical or nominal data. Correlations between periodontal indices or quantitative data of periodontal pathogens and RA disease activities or characteristics were analyzed using Pearson or Spearman correlation coefficients as appropriate. All P values were 2-sided, and P values <0.05 were considered to indicate statistical significance.
RESULTS
Baseline characteristics
Overall, 260 RA patients and 86 controls participated in the study. There were no significant differences in the baseline characteristics between the 2 groups (Table 2). The proportion of smokers, which is known to be a risk factor for RA and periodontitis, was 6.4% and 8.0% respectively. In the RA group, the mean disease duration was 14.24±9.72 years, and the mean DAS28 was 3.62±1.35, corresponding to moderate RA disease activity. The proportion of RF-positive patients was 67.4%, and that of anti-CCP antibody-positive patients was 67.5%; radiographic bone erosion was found in 70% of patients.
Table 2
Baseline characteristics, RA disease characteristics, and activities (t-test, chi-square test)
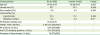
Values are presented as mean±SD not otherwise specified.
RA: rheumatoid arthritis, DAS28: disease activity score 28, RF: rheumatoid factor, CCP: cyclic citrullinated peptide, SD: standard deviation.
![]()
Comparison of periodontal indices between the RA and control groups
The RA group had significantly higher values than controls (P<0.05) for all periodontal indices except the number of teeth (Table 3): PI (0.83±0.48 vs. 0.72±0.34), GI (0.51±0.43 vs. 0.16±0.20), PPD (1.96±0.36 vs. 1.75±0.24), BOP (20.32±15.43 vs. 12.44±11.00), and CAL (3.25±0.74 vs. 2.91±0.52). The severity of periodontitis in all participants was slight or more than slight. The RA group had a significantly higher prevalence of moderate-to-severe periodontitis than the control group (64.2% vs. 34.9%, P<0.001, Table 3).
Table 3
Periodontal disease indices and periodontitis severity in the RA and control groups (t-test and χ2 test, respectively)
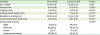
Values are presented as mean±SD or No. (%).
RA: rheumatoid arthritis, SD: standard deviation.
a)P value <0.05 by the t-test; b)P value <0.05 by the χ2 test (slight vs. moderate-to-severe).
![]()
Quantitative and qualitative analyses of periodontal pathogens in the RA and control groups
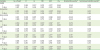
All 9 pathogens were recorded as having >80% prevalence (Table 4). The chi-square or Fisher exact test was used for qualitative analyses of the relationship between the presence of each pathogen and RA. No statistically significant differences were observed in any of the 9 pathogens according to the presence or absence of RA. Quantitative analyses were performed between the 2 groups using the Mann-Whitney U test. Fusobacterium nucleatum (Fn) showed a significantly higher rank sum in the RA group than in the control group (P=0.024). Conversely, Eikenella corrodens (Ec) was noted to have a higher rank sum in the control group (P<0.001) (Table 4).
Table 4
Prevalence of each periodontal pathogen and a quantitative comparative analysis between the RA and control groups

Values are presented as No. in % or rank sum of Mann-Whitney U test.
Pg: Porphyromonas gingivalis, Td: Treponema denticola, Tf: Tannerella forsythia, Pi: Prevotella intermedia, Pm: Parvimonas micra, Fn: Fusobacterium nucleatum, Ec: Eikenella corrodens, Cg: Capnocytophaga gingivalis, AA: Aggregatibacter actinomycetemcomitans.
a)P value by the χ2 test or Fisher exact test; b)P value by the Mann-Whitney U test; c)P value <0.05.
![]()
Associations of periodontal indices with RA disease activity and characteristics
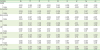
Table 5 presents the correlations of periodontal indices with RA disease activity and characteristics. The number of teeth and PI were not correlated with any aspects of RA disease activity or characteristics. The GI was correlated with DAS28 (r=0.125, P=0.049), RA disease duration (r=0.253, P<0.001), ESR (r=0.162, P=0.010), and anti-CCP antibody titer (r=0.205, P=0.004). PPD was correlated with ESR (r=0.139, P=0.027) and the anti-Pg antibody titer (r=0.203, P=0.001). BOP was correlated with DAS28 (r=0.137, P=0.030), RA disease duration (r=0.202, P=0.001), ESR (r=0.136, P=0.030), the anti-Pg antibody titer (r=0.177, P=0.005), and the anti-CCP antibody titer (r=0.188, P=0.007). The CAL was correlated with the anti-Pg antibody titer (r=0.201, P=0.002). Periodontitis severity was evaluated as slight (CAL 1–2 mm), moderate (CAL 3–4 mm), or severe (CAL≥5 mm) according to the AAP guidelines [18]. In this study, nominal severity was also evaluated, which was classified into 2 categories: slight (CAL 1–2 mm) and moderate-to-severe (CAL ≥3 mm). Both severity measures were correlated with the anti-Pg antibody titer (the former: r=0.175, P=0.006; the latter: r=0.159, P=0.012).
Table 5
Correlations of periodontal indices with RA disease activity and characteristics of the RA group (n=260)
RA: rheumatoid arthritis, PI: plaque index, GI: gingival index, PPD: probing pocket depth, BOP: bleeding on probing, CAL: clinical attachment level, DAS28: disease activity score 28, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, Anti-Pg ab: anti-Pg antibody titer, RF: rheumatoid factor, Anti-CCP ab: anti-cyclic citrullinated peptide antibody titer, r: Spearman correlation coefficient (rho).
a)Periodontitis severity: slight/moderate/severe; b)Nominal periodontitis severity: slight/moderate-to-severe; c)Significant correlation at P<0.05.
![]()
Associations of the amount of periodontal pathogens with RA disease activity and characteristics
The quantity of Pg in the periodontal environment was positively correlated with the anti-Pg antibody titer (r=0.148, P=0.020) in serum. Ec was negatively correlated with the RF titer (r=−0.203, P=0.001). Aggregatibacter actinomycetemcomitans (Aa) showed a negative correlation with RA disease duration (r=−0.129, P=0.042) (Table 6).
Table 6
Correlations of the amounts of periodontal pathogens with RA disease activity and characteristics of the RA group (n=260)
RA: rheumatoid arthritis, Pg: Porphyromonas gingivalis, Td: Treponema denticola, Tf: Tannerella forsythia, Pi: Prevotella intermedia, Pm: Parvimonas micra, Fn: Fusobacterium nucleatum, Ec: Eikenella corrodens, Cg: Capnocytophaga gingivalis, AA: Aggregatibacter actinomycetemcomitans, DAS28: disease activity score 28, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, Anti-Pg ab: anti-Pg antibody titer, RF: rheumatoid factor, Anti-CCP ab: anti-cyclic citrullinated peptide antibody titer, r: Pearson or Spearman correlation coefficient.
a)Significant correlation at P<0.05.
![]()
DISCUSSION
In this study, the RA group showed significantly higher values than the control group for all investigated periodontal indices, except the number of teeth. Individuals with <15 teeth were excluded from this study due to the possibility of bias in evaluating the difference in periodontitis severity between the RA and control groups. Papapanou [20] reported that periodontitis is thought to be the cause of 30%–35% of all tooth extractions, whereas dental caries and their sequelae account for up to 50% in older age cohorts. Therefore, tooth loss data are not feasible to use as an indicator of the prevalence of periodontal disease. Several studies [21222324] with similar subjects also limited the number of teeth to 10–20, and the results in the number of teeth were not consistent between the RA and control groups. The PI is an index of dental hygiene; thus a high PI value could be expected to result from compromised joint movement in RA patients. However, DAS28, which was used in this study as an RA disease activity index, did not show a statistically significant correlation with the PI. Moreover, our preceding study [13] did not find a statistically significant correlation between the PI and the TJC or SJC. Furthermore, the PI was not correlated with any other RA indices in this study; therefore, it can be excluded as a predisposing factor in the expected mutual relationship between RA and periodontitis. However, it is still important to emphasize dental hygiene practices to RA patients because impaired dental hygiene is directly connected with periodontitis onset and progression. The GI is an observable index of periodontal inflammation, and BOP is a useful index for the early diagnosis of periodontitis. These 2 indices had higher values in the RA group than in the control group, implying a possible connection between these 2 diseases linked to inflammation. Indeed, in the correlation data (Table 5), increases in DAS28 and RA disease duration — indicators of RA disease activity — were associated with higher mean values of the GI and BOP. Moreover, the anti-CCP antibody titer, which was used as a marker of elevated inflammation linked to RA, also was positively correlated with the GI and BOP. Furthermore, the ESR, which is used in diagnosing RA as a factor indicating systemic inflammation, showed a correlation with the GI, BOP, and PPD in this study. Recently, Harvey et al. [25] reported that the citrullinated proteins PAD-2/-4 were present in inflamed periodontal tissues and that anti-CCP antibodies were found mostly in the gingival crevicular fluid of individuals with periodontitis. Several studies [324] have reported that RA patients with periodontitis had higher serum ESR values than did RA patients without periodontitis. These results support the possibility of a common inflammatory pathway or linkage in the development of these 2 diseases. Meanwhile, the PPD and CAL, indices of periodontal structural destruction, also had higher values in the RA group than in the control group in the present study. According to a systematic review by Kaur et al. [5], 7 of 10 studies [24262728293031] evaluating differences in CAL depending on RA reported statistically significant differences, and a meta-analysis showed a higher CAL in the RA group than in the non-RA control group, with an overall weighted mean difference of 1.17 (95% CI, 0.43–1.90). In addition, the prevalence of moderate-to-severe periodontitis was higher in the RA group (64.2%) than in the control group (34.9%) in this study, corresponding with several previous reports [1224].
There was no significant difference in the prevalence of periodontal pathogens between the RA and the control group in this study, unlike the hypothesis initially formulated. This result accords with that of the aforementioned study of Schmickler el al. [12]. In the present study, all of the pathogens showed a prevalence of >80% in both groups. On one hand, the relatively high prevalence of periodontal pathogens compared with other studies [1112] might have been due to the prevalence of periodontal disease among the participants. Indeed, all participants of both groups showed slight or more than slight periodontitis according to the AAP criteria. On the other hand, quantitatively, Fn showed a higher rank sum in the RA group than in the control group (P=0.024), which also corresponds with the study by Schmickler et al. [12], which tested the distribution of bacterial concentration. In their study, Fn and Pm showed higher concentrations significantly more often in RA patients than in healthy controls. Meanwhile, in our study, Ec had a higher rank sum in the control group than in the RA group (P<0.001); Ec also was negatively correlated with the RF titer. However, according to each microbial complex, there was no overall tendency for quantitative differences to exist between the RA and the control groups. Recently, Konig et al. [32] suggested that Aa induces cellular hypercitrullination from neutrophils in joints affected by RA via leukotoxin A (LtxA), and anti-LtxA antibody positivity was significantly associated with anti-CCP antibodies and RF factor positivity in RA. However, Aa only showed a negative correlation with RA disease duration in this study.
Several studies reported significantly higher antibody responses to Pg in RA patients than in controls [3334]. In the present study, we focused on the anti-Pg antibody titer in the RA group only. There was a positive correlation between the quantity of Pg in the periodontal environment and the serum anti-Pg antibody titer, which means that more Pg in the oral environment can lead to more serum anti-Pg antibody, essentially verifying the theory that Pg in the oral cavity might be circulated systemically. Furthermore, positive correlations were found between the anti-Pg antibody titer and PPD, BOP, CAL, and periodontitis severity. Other studies also have reported correlations between the anti-Pg antibody titer and periodontal indices such as PPD and CAL [353637]. These results could suggest that high anti-Pg antibody titers in RA patients might be considered as an indicator of the need for periodontal disease treatment. It is therefore recommended that RA patients with symptomatic periodontal issues and an elevated anti-Pg antibody titer should be treated for periodontal disease due to the risk of periodontal tissue destruction (PPD, CAL), periodontal inflammation (BOP), and increasing severity of periodontitis. Alternatively, periodontal examinations in the dental clinic can be used as an evaluation of the need for intensive RA care in RA patients. Those who present with increasing periodontal indices (e.g., GI, PPD, and BOP) at regular periodontal checkups might be referred to the RA clinic for control of their RA disease activity, as these changes could be connected with higher values of serum ESR or anti-CCP antibody titer, which indicate further RA disease progression.
This study examined the relationships of 9 periodontal pathogens with RA indices based on the interrelationships of periodontal disease with RA indices, using a relatively large sample size to increase statistical power. The study was particularly focused on the role of Pg, as analyzed using quantitative data for the oral environment and serum antibody data for the systemic environment, and the finding of positive relationships between the serum antibody titer and periodontal indices was meaningful. However, all correlation coefficients were relatively low (all r<0.3), even if they were statistically significant. Thus, the results cannot be interpreted as strongly supporting the hypothesis of this study that RA indices would be closely related to periodontal indices and the amount of periodontal pathogens. There were other limitations of this study. We only analyzed anti-Pg antibody and anti-CCP antibody titers in the RA group, although a comparison with the control group would have allowed a clearer elucidation of the possible role of Pg as a risk factor for RA. Further, smoking has been identified as a major risk factor for the development of RA [3839] and periodontal disease [20]. However, the proportion of ever smokers was 6.3% in the RA group and 9.3% in the control group, which is relatively low compared with other study cohorts [40]. There were no statistically significant differences between the 2 groups. Conversely, however, the use of a cohort with a low proportion of smokers could be effective for assessing the role of periodontal disease as a risk factor for RA.
In conclusion, the presence of RA was associated with high values of periodontal indices and periodontitis severity. There was no significant difference in the prevalence of periodontal pathogens between the RA and the control groups. Fn showed a higher rank sum in the RA group than in the control group, but according to each microbial complex, there was no overall tendency for quantitative differences between the 2 groups. The GI, BOP, and PPD showed positive relationships with several indicators of RA disease activity. A positive correlation was found between the quantity of Pg and the serum anti-Pg antibody titer, which had positive relationships with PPD, BOP, CAL, and periodontitis severity. Thus, increasing values of periodontal indices could be used as a risk indicator of disease development in RA patients, and an increasing anti-Pg antibody titer could be considered as a warning sign in RA patients suffering from periodontitis. For further meaningful results, a prospective study comparing RA indices, including serum antibody levels, between baseline and after periodontal treatment might be necessary, as well as a study investigating the correlations of more specific serum antibodies related to Pg. Further research in these directions may be helpful not only for defining the association of these 2 diseases pathobiological, but also for evaluating the clinical implications of this relationship.
 XML Download
XML Download