

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peripheral artery disease (PAD) is a form of arteriosclerosis that primarily affects the lower extremities and involves ischemia. It is widely regarded as an important risk factor for all causes of death, especially cardiovascular death [1]. It is estimated that there are 500,000 to 800,000 patients with PAD in Japan [2]. In 2010, there were approximately 220 million people with the disease worldwide; notably, this number had increased by nearly 25% during the previous decade [23].
Periodontal disease (PD) is an infectious and inflammatory oral disease caused by bacteria that affects the periodontal tissues surrounding the teeth. Attempts have been made to classify PD and to standardize its diagnosis in recent decades, in order to determine whether phenotypically different cases represent a single disease or different diseases [4]. At an international workshop held in 2017, PD was clearly defined as a host-mediated and microbially-associated inflammation that leads to loss of periodontal attachment; however, it was stated that the staging and grading system for PD exhibited diagnostic complexity without providing substantial clinical information [4].
A national survey of dental diseases in Japan reported that the number of patients with PD who are over 65 years old has increased in recent years [5]. According to the present understanding, PD contributes to the deterioration of an individual's systemic condition [6]. In a longitudinal study of health in Pomerania, serum levels of fibrinogen and white blood cell counts were associated with the extent of sites with deep probing pocket depth (PPD) and a high clinical attachment level (CAL) [6]. Another study reported that serum levels of C-reactive protein (CRP) and interleukin-6 (IL-6) in subjects with PD were significantly decreased by periodontal treatment [7].
Recently, it has been suggested that PD influences arteriosclerosis, including PAD [8]. Previous studies have reported that patients with periodontitis had a high risk of PAD [910]. However, the relationship between these 2 diseases has not yet been fully elucidated. Moreover, previous papers have reported that little relationship exists between PD and arrhythmia (ARR) [111213]. Therefore, in this cross-sectional study, we investigated the relationship between PAD and PD by comparing patients with PAD to those with ARR as a control group.
MATERIALS AND METHODS
Subject population and selection criteria
A large-scale survey was conducted of patients with cardiovascular disease who received cardiovascular care at Tokyo Medical and Dental University Hospital from May 2012 to August 2015, as previously described [9]. Briefly, clinical dental findings were measured in all patients in this cross-sectional study. Patients who agreed to participate in this study were included. We excluded patients who did not agree to participate in this research and had other infectious diseases in the past and/or present. Thereafter, all patients with PAD were extracted from the overall study population (n=25), along with a matching number of patients with ARR (n=25). To compare the PAD (test) and ARR (control) patients, we matched them in terms of age, gender, prevalence of diabetes, hypertension, dyslipidemia, obesity, and smoking rate. The number of subjects in each group was therefore designated as n=25.
All protocols of this study were approved (M2000-1165) by the Ethics Committees of the School of Medicine and the School of Dentistry, Tokyo Medical and Dental University. The protocols were in accordance with the Helsinki Declaration of 1975, as revised in 2013. Written informed consent was provided by the subjects.
Medical examinations
Medical doctors collected the participants' medical history, including hypertension, diabetes mellitus, and dyslipidemia, as well as history of cigarette smoking, by interview. A physical examination was also performed. PAD was diagnosed on the basis of clinical symptoms, which included the classification of Fontaine grade I to IV ischemia and angiographic findings, as well as an ankle brachial pressure index of <0.9 [10]. ARR was diagnosed as tachyarrhythmia or bradyarrhythmia on electrocardiography [11]. We collected samples of peripheral blood, which were centrifuged at 1,500×g for 20 minutes and stored at −20°C. Levels of CRP and hemoglobin A1c (HbA1c) were measured in those samples.
Dental examinations
Three trained periodontists examined the number of teeth in each patient. They then measured PPD, CAL, and bleeding on probing (BOP) with a manual probe (PCP-UNC 15; Hu-Friedy, Chicago, IL, USA) at 6 points per tooth (buccal-mesial, mid-buccal, buccal-distal, lingual-mesial, mid-lingual, and lingual-distal); these measurements were made on a right upper molar, an upper incisor, a left upper molar, a right lower molar, a lower incisor, and a left lower molar. If any teeth were missing, we selected an alternative adjacent tooth [9].
Quantitative real-time polymerase chain reaction (PCR) for bacterial detection
We collected gingival crevicular fluid by inserting a #40 paper point into the deepest periodontal pocket of all the tested sites and collecting unstimulated saliva from each patient. Bacterial DNA was extracted from these samples by the DNeasy Blood and Tissue kit (Qiagen, Tokyo, Japan) in accordance with the manufacturer’s protocol. We performed real-time PCR to detect 2 major periodontal bacteria, Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis. DNA samples obtained from 102 to 108 cells of cultured bacteria were used to set the quantitative range of the PCR. The sequences of the specific primers were as follows: 5′-CTTGACTTCAGTGGCGGCAG-3′ and 5′-AGGGAAGACGGTTTTCACCA-3′ for P. gingivalis, and 5′-CTTACCTACTCTTGACATCCGAA-3′ and 5′-ATGCAGCACCTGTCTCAAAGC-3′ for A. actinomycetemcomitans [14]. We used the Thermal Cycler Dice® Real Time System II (Takara Bio, Shiga, Japan) for real-time PCR. PCR mixtures were made by SYBR® Premix Ex TaqTM II (Takara Bio), and the PCR conditions followed the manufacturer's protocol.
Analysis of anti-bacterial antibody titers and proinflammatory cytokines
Titers of immunoglobulin G (IgG) antibodies against the periodontopathic antigens P. gingivalis and A. actinomycetemcomitans were analyzed in the serum samples by an enzyme-linked immunosorbent assay (ELISA), as previously described [1516]. The absorbance for each well was read using a microplate reader at 450 nm with a reference wavelength of 650 nm. Individual serum antibody levels (U/mL) were calculated by using a standard curve obtained from serial dilutions of the reference solution [17]. For detecting serum levels of the proinflammatory cytokines tumor necrosis factor-alpha (TNF-alpha) and IL-6, we also used ELISA (Quantikine® ELISA; R&D Systems, Minneapolis, MN, USA).
Statistical analysis
Each result, except for antibody levels and bacterial data, was expressed as mean±standard error. The data of the IgG antibodies and the bacterial counts were represented by box-and-whisker plots. The Fisher exact test was performed to compare the edentulism rate. The Mann-Whitney U test was applied for comparisons, except for comparisons of HbA1c, because the Shapiro-Wilk test verified that only the HbA1c data were normally distributed. The Student's t-test was therefore used to compare HbA1c levels. The statistical analysis was conducted using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). P values <0.05 were considered to indicate statistical significance for all tests.
RESULTS
Characteristics of PAD and ARR patients
Fifty patients were included in this cross-sectional study. The PAD and ARR groups were matched in terms of age, gender, diabetes, hypertension, dyslipidemia, obesity, and smoking rate, as shown in Table 1. There were no significant differences in the edentulism rate or HbA1c levels between the 2 groups.
Table 1
Characteristics of PAD and ARR patients
The number of missing teeth was significantly higher in the PAD group than in the ARR group (P<0.05; Figure 1). However, there were no statistically significant differences in indicators of periodontal status, such as mean PPD, CAL, and BOP, between the groups (Figure 1). In terms of the deepest PPD at the front teeth and molars, the mean PPD at the front teeth was deeper in the PAD group than in the ARR group (P<0.05; Figure 2). The serum levels of CRP and TNF-alpha were significantly higher in PAD patients than in ARR patients (P<0.05 and P<0.01, respectively; Figure 3). No statistically significant difference was observed in IL-6 levels between the groups; however, the IL-6 levels in the PAD group were somewhat higher than those in the ARR group.
Figure 1
Periodontal status. (A) mean PPD, (B) CAL, (C) BOP, and (D) number of missing teeth for each subject in both PAD (test) and ARR (control) groups were measured. The values are expressed as mean±standard error.
PPD: probing pocket depth, CAL: clinical attachment level, BOP: bleeding on probing, PAD: peripheral artery disease, ARR: arrhythmia.
a)P<0.05 compared with the ARR group.

Figure 2
The deepest PPD at front teeth and molars. PPD for all tested sites was calculated and we selected sites that had the deepest PPD and single roots at the front teeth area, and the PPD and multiple roots at the molars area, respectively, for each subject. The deepest PPDs for both PAD (test) and ARR (control) groups were averaged as the representative values per group. The values are expressed as mean±standard error.
PPD: probing pocket depth, PAD: peripheral artery disease, ARR: arrhythmia.
a)P<0.05 compared with the ARR group.

Figure 3
Comparison of serum levels. Peripheral blood was collected from all subjects in both PAD (test) and ARR (control) groups and the levels of (A) CRP, (B) IL-6, and (C) TNF-alpha in the serum were measured. The values are expressed as mean±standard error.
PAD: peripheral artery disease, ARR: arrhythmia, CRP: C-reactive protein, IL-6: interleukin-6, TNF-alpha: tumor necrosis factor-alpha.
a)P<0.05; b)P<0.01 compared with the ARR group.

Microbiological status
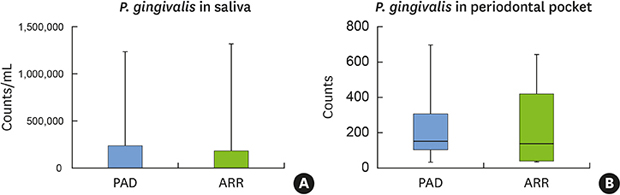
We examined microbiological status by real-time PCR and immunological data obtained using the ELISA method. The levels of serum antibodies against P. gingivalis and A. actinomycetemcomitans are shown in Figure 4. No significant differences in antibody levels between the PAD and ARR groups were observed. Regarding the presence of bacteria, there were no statistically significant differences in the P. gingivalis counts in saliva and the periodontal pocket between the 2 groups (Figure 5). Moreover, no significant differences in A. actinomycetemcomitans counts were observed (data not shown).
Figure 4
IgG antibody titers of periodontal bacteria. IgG antibody titers of each periodontopathic antigens (A) P. gingivalis and (B) A. actinomycetemcomitans were analyzed with serum samples from all subjects in both PAD (test) and ARR (control) groups by ELISA. Box-and-whisker plot shows medians, 25th and 75th percentiles as boxes, and 10th and 90th percentiles as whiskers.
IgG: immunoglobulin G, PAD: peripheral artery disease, ARR: arrhythmia, ELISA: enzyme-linked immunosorbent assay.

Figure 5
P. gingivalis counts in oral samples. Gingival crevicular fluid was collected from the deepest periodontal pocket and unstimulated saliva from each subject in both PAD (test) and ARR (control) groups, then bacterial counts by real-time PCR were measured. (A) P. gingivalis counts in saliva. (B) The counts in periodontal pocket. Box-and-whisker plot shows medians, 25th and 75th percentiles as boxes, and 10th and 90th percentiles as whiskers.
PAD: peripheral artery disease, ARR: arrhythmia, PCR: polymerase chain reaction.

DISCUSSION
In this clinical study, the PAD group had more missing teeth and higher serum levels of CRP and TNF-alpha than the ARR group.
Periodontitis constitutes a large proportion of the etiological basis for missing teeth in Japan [18]. According to a national survey of dental diseases in Japan, the prevalence of periodontitis is high in adults, especially those aged 65 years or older [5]. Notably, the patients with PAD in the present study exhibited significantly greater values of the deepest PPD in the front teeth area than the ARR group. Based on our observations, it seems likely that the main cause of the missing teeth in patients in the present study was periodontitis.
In contrast, there were no significant differences between the PAD and ARR groups in terms of other periodontal markers, such as mean PPD, CAL, and BOP. These parameters, however, may not exhibit a significant difference because they were calculated by an average of all measurement sites. We used those parameters as periodontal indicators in this study, as they are extensively used worldwide. In contrast, the periodontal inflamed surface area, which is a novel indicator of PD, has been adopted for some clinical situations [1920]. The periodontal pocket is the original inflammatory indicator for all periodontal tissue; consequently, it can be presumed that 6-point measurements of representative teeth, as in PPD, do not accurately indicate the status of PD. Therefore, a novel indicator that enables the precise state of periodontitis in a patient to be readily understood would be helpful in future studies.
PAD is a pathological form of atherosclerosis, which involves accumulation of atherosclerotic plaques inside the arterial wall. It can occur due to dysfunction of vascular endothelial cells, as adhesive molecules, including vascular cell adhesion molecule-1 and intercellular adhesion molecule-1, are expressed on vascular endothelial cells, as well as neutrophils and low-density lipoprotein (LDL) cholesterol, which often circulate in the vascular system and are stored in the vascular wall. Subsequently, inflammation results from the chemotaxis of macrophages into blood vessels through production and activation of chemotactic molecules, such as IL-8 and monocyte chemoattractant protein-1. These macrophages become foam cells, which remain in the vascular wall upon phagocytosis of oxidative LDL; thus, the lesion deteriorates into an atheroma [2122]. Additionally, PD is caused by bacterial infection, which leads to the production of proinflammatory cytokines and chemokines, such as IL-1, IL-6, IL-8, and TNF-alpha, by cells in the periodontal tissue; these include epithelial cells, periodontal ligament cells, gingival fibroblasts, osteoblasts, and dendritic cells. This affects immunocytes and osteoclasts, thus deteriorating local inflammation and bone resorption [23]. Moreover, previous studies have reported that PD causes increased levels of systemic proinflammatory markers in the serum, such as CRP, TNF-alpha, IL-1, IL-6, and IL-8 [2425]. In 2014, a systematic review and meta-analysis demonstrated that periodontal treatment significantly improved vascular endothelial function and reduced the expression of proinflammatory markers such as CRP, IL-6, and TNF-alpha [26].
In these 2 diseases, inflammatory cytokines and chemokines, such as IL-1, IL-6, and TNF-alpha, play a role in a mutual inflammatory pathway; each of these molecules that is produced in periodontal tissue and blood vessels enhances the production of CRP and fibrinogen through the liver and promotes inflammation [27]. This relationship is consistent with the present results, specifically the significant elevation of serum levels of TNF-alpha and CRP in the PAD group; these significant increases of systemic inflammatory markers may have been influenced by both PD and PAD. Furthermore, many recent papers have reported associations between periodontitis and a variety of factors, including gender, diabetes, hypertension, dyslipidemia, obesity, and smoking [282930]. Because we considered these associations before selecting and matching patients in the PAD and ARR groups, we adjusted the number of patients with each parameter to ensure matching between the groups.
With the above considerations, the present results suggest that PD may influence PAD via systemic inflammation, which is consistent with a previous report [31]. However, the causal relationship cannot be clarified because this study is cross-sectional. There are 2 additional limitations of this study: the sample size and the use of ARR patients as a control group.
We measured periodontal and systemic inflammatory conditions in a large number of patients with cardiovascular disease, and extracted PAD patients (n=25) for this study. Thus, a sample size calculation was not performed before the present analyses. As a result, we found that PAD patients had a higher number of lost teeth and elevated levels of serum inflammatory markers, despite the small sample. Sample size calculation is important in clinical studies, and the lack of such a calculation is a limitation of this study. To confirm these results, a future study with adequate sample size calculation is needed. Several periodontal parameters, such as PPD and CAL, were not significantly different between the groups in the present study; however, an analysis with an adequate and larger sample size might show statistically significant differences in these parameters.
Regarding the latter limitation, the evidence of a relationship between PD and ARR in previous reports is weak [1112]. Additionally, it has been suggested that there is no association between ARR and PD in elderly patients, despite the possible link between cardiac ARRs and active root caries that was found in a previous study [13]. In addition, there were many patients with ARR in the original dataset of our large-scale study; they were readily available for use as a matched control group for the 25 patients with PAD. However, comparisons between subjects without any cardiovascular disease and PAD patients should be conducted to examine the true association between PAD and PD. Because of the limitations stated above, further studies are needed in the future.
In conclusion, PAD patients appear more likely to exhibit a deteriorated state of oral health, periodontitis, and systemic inflammation than ARR patients. Clinical studies are therefore required to clarify the relationship between PAD and PD in greater detail.
 XML Download
XML Download