

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) is a global public health threat and remains a major cause of death from infectious diseases. Among the many risk factors for active TB,1 end-stage renal disease (ESRD) that requires dialysis has recently been highlighted because of the high global prevalence of this condition, which is related to the increased incidence of diabetes and aging populations in both developing and developed countries.23 Korea is confronted with increasing populations of elderly individuals and patients with diabetes, which has led to a rapid increase in the number of patients with ESRD.4 Thus, the convergence of the TB and ESRD epidemics is generating a significant public health burden and making it difficult to control TB in Korea, which has an intermediate TB-related burden.
Chronic kidney disease (CKD) is associated with altered cellular immunity that is caused by various factors, including advanced age, uraemia, hypoalbuminemia, malnutrition, and medical immunosuppression. During ESRD, abnormal functioning of monocytes, neutrophils, and dendritic cells are directly linked to the risk of infection.5 Furthermore, CKD is linked to other conditions that increase the risk of developing active TB, such as diabetes, transplantation, and human immunodeficiency virus (HIV) infection. Moreover, dialysis patients with ESRD are frequently exposed to the healthcare setting and are very susceptible to nosocomial infections, which might be a source of TB outbreaks.6 Transmission of infectious diseases, such as TB, has attracted considerable public attention in Korea since the Middle East Respiratory Syndrome outbreak during 2015, which involved a large number of suspected hospital-acquired infections.7
TB is a known significant threat to patients receiving dialysis, as they have a 2-fold higher TB-related mortality rate than the general population and a 3-fold higher rate than patients receiving dialysis without TB.8 The health threats of TB to patients with ESRD have attracted researchers' attention for several decades, however, previous studies have been limited to a small number of patients. This retrospective propensity score-matched cohort study used Korean national health insurance data to examine the incidence of active TB in a large population of patients receiving dialysis, as well as the ESRD-related risk of developing active TB.
METHODS
Database
The dialysis and control cohorts were created using the Korean National Health Insurance Service (KNHIS) database, which is maintained by a single national insurance provider that covers > 97% of the Korean population. Data regarding patients who received dialysis were obtained from the KNHIS database, which contains reimbursement data from all medical facilities (Fig. 1). We also collected control data from the KNHIS-National Sample Cohort (NSC), which includes approximately 1,000,000 individuals (2.2% of the total Korean population) and was created using the KNHIS database for use by public health researchers and policy makers.9 The KNHIS database contains data regarding patient gender, age, and income level, as well as data regarding medical care utilisation (e.g., date of treatment, diagnosed disease, prescribed drugs, and medical or surgical procedures).

Cohort definitions
Patients with newly diagnosed ESRD between 2004 and 2013 were selected as the dialysis cohort. Cases with dialysis were identified using claims for any procedures or materials related to haemodialysis or peritoneal dialysis, based on the Korean electronic data interchange codes (O7020 for haemodialysis; O7061 for peritoneal dialysis). Patients with a diagnosis of ESRD who had used medical services in 2003 were excluded based on the assumption that they had chronic ESRD. Patients were considered eligible if they had received dialysis for > 90 days, as a small portion of patients might have received renal replacement therapy after acute kidney injury and recovered sufficient renal function to stop the dialysis. The criteria for identifying dialysis were used to exclude patients in the KNHIS-NSC who had received dialysis, which created the control cohort for the present study.
Definition of TB
The incidences of active TB in the dialysis and control cohorts during 2004–2013 were identified using International Classification of Disease, 10th revision (ICD-10) codes (A15–19). The diagnosis of active TB was then confirmed based on prescriptions for ≥ 2 anti-TB drugs during a 30-day period. The anti-TB drugs included isoniazid, rifampicin, ethambutol, pyrazinamide, amikacin, kanamycin, streptomycin, quinolones, thioamide, cycloserine, and para-aminosalicylic acid. Patients diagnosed with active TB in 2003 were excluded to ensure that only newly diagnosed patients with TB from 2004 were included.
Co-variables
Factors that might influence the incidence of active TB, such as gender, age, income level, and comorbidities, were used as independent variables. Data regarding these covariates were available for the dialysis and control cohorts using the KNHIS database. Comorbidities were identified based on ICD-10 codes such as diabetes mellitus (E10–14), malignancy (B21, C00–97, D37–48, Z08, Z12, Z51.0–51.2, Z85, U99), chronic obstructive pulmonary disease (COPD) (J44), HIV infection (B20–24), and silicosis (J60–64). Income level was scored on a scale of 0 to 10, and was categorised into three groups: low, middle, and high.
Propensity score matching
We included patients who began dialysis before their diagnosis of active TB based on the visit date. We washed out data in 2003 to ensure that only newly diagnosed patients with ESRD were included. Data between 2014 and 2015 were excluded, because the KNHIS-NSC database contained only data up to 2013. Finally, these eligible patients, who started dialysis during 2004–2013 (dialysis cohort), were identified after excluding potentially pre-existing cases of dialysis or active TB. We identified individuals without ESRD from the KNHIS-NSC database (control cohort), who were propensity score matched to an equal number of ESRD cases. Propensity score matching using the nearest neighbour method was performed to identify similar individuals in the dialysis and control cohorts using the Matchlt package version 3.0.1 in R software (version 3.4.3; R Foundation for Statistical Computing, Vienna, Austria). Logistic regression was used to create propensity scores for each patient based on their age, gender, income level, and comorbidities. Individuals in both cohorts were randomly ordered and matched 1:1 using the nearest neighbour method. A matching algorithm identified a unique matched control for each individual in the dialysis cohort according to the propensity score. Once a match was completed, the match was not considered again. If a match could not be found, the algorithm then proceeded sequentially to an individual with the closest propensity score to make the next-best match. To improve generalisability and reduce potential bias caused by incomplete matching, we used a random selection of samples from the set of all subjects.10
Statistical analysis
Proportional differences in independent variables between the ESRD and control cohorts were analysed using the Wald χ2 test. The incidence of active TB was expressed as the number of newly diagnosed active TB cases per 100,000 person-years. The incidence rate ratio (IRR) of ESRD, relative to the controls, was calculated with its 95% confidence interval (CI) using the epiR package version 0.9–96 in R software (version 3.5.0; R Foundation for Statistical Computing). We applied a multivariate Cox proportional hazards model to all independent variables after combining the two cohorts to determine the ESRD-related risk of developing active TB, which was reported as hazard ratio (HR) and 95% CI. We evaluated the proportional hazard assumption by testing the significance of time-dependent interaction terms for all variables, which were found to be satisfactory. Cumulative TB incidence curves were generated using the Kaplan-Meier method, and differences between two cohorts were analysed using the log-rank test. The follow-up period started on the first date of dialysis for the cases and on randomly selected visit dates for the controls, which corresponded to the calendar year that matched to the start of dialysis for the cases. The follow-up period ended at the first date of TB diagnosis or the last follow-up date. Analyses were performed using SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA) and R software (version 3.4.3; R Foundation for Statistical Computing).
RESULTS
A search of the KNHIS database identified 59,584 patients with newly diagnosed ESRD during 2004–2013 (the dialysis cohort), and a corresponding number of individuals were selected for the control cohort. The individuals' characteristics are summarised in Table 1. Individual matching resulted in comparable distributions of age, gender, household income, and comorbidities between the dialysis and control cohorts. The observation periods were 212,417 person-years in the dialysis cohort and 278,960 person-years in the control cohort. The mean durations of follow-up were 3.6 ± 2.7 years in the dialysis cohort and 4.7 ± 2.8 years in the control cohort.
Table 1
Baseline characteristics of the dialysis patients and controls

DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease, HIV = human immunodeficiency virus.
![]()
Newly diagnosed active TB was detected for 457 patients in the dialysis cohort (0.8%) and 125 individuals in the control cohort (0.2%) (Table 2). The incidences were 215/100,000 person-years in the dialysis cohort and 45/100,000 person-years in the control cohort. Compared to the controls, the patients with ESRD had a significantly elevated risk of active TB (IRR, 4.80; 95% CI, 3.95–5.87). The subgroup analyses revealed similarly elevated risks of active TB among patients with ESRD for most subgroups, with the exception of the ≥ 80 years age group. The average interval from the initial enrolment to the diagnosis of active TB was 2.0 years (1.7 years for the dialysis cohort and 3.1 years for the control cohort).
Table 2
Characteristics of active TB cases among dialysis patients and controls

TB = tuberculosis, IRR = incidence rate ratio, CI = confidence interval, PY = person-years, IR = incidence ratio, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease, HIV = human immunodeficiency virus.
aIncidence rate per 100,000 PY.
![]()
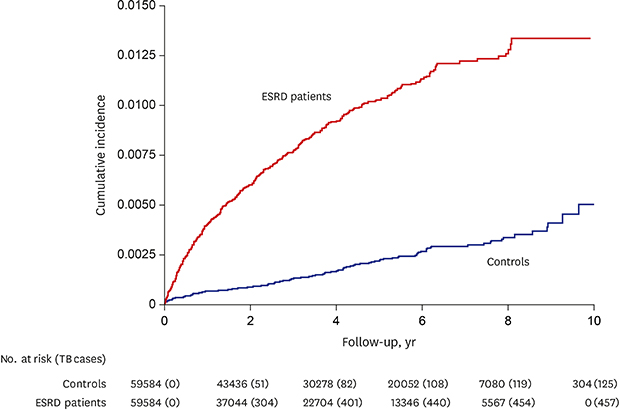
The cumulative active TB incidence was significantly higher in the dialysis cohort than in the control cohort (P < 0.001; log-rank test) (Fig. 2), and subgroup analyses revealed similar results for both haemodialysis and peritoneal dialysis (both P < 0.001; log-rank test). However, there was no significant difference in the risk of active TB between the haemodialysis and peritoneal dialysis subgroups (P = 0.67; log-rank test).
 | Fig. 2Cumulative incidence of active TB among patients receiving dialysis with ESRD and controls.TB = tuberculosis, ESRD = end-stage renal disease.
|
Multivariate Cox proportional hazard analysis revealed that patients who received dialysis for ESRD had an independently elevated risk of active TB (adjusted HR, 4.39; 95% CI, 3.60–5.37) (Table 3). In addition, elevated risks of active TB were independently associated with haemodialysis (adjusted HR, 4.38; 95% CI, 3.58–5.37) and peritoneal dialysis (adjusted HR, 5.80; 95% CI, 4.06–8.29) (Table 4). Further analysis did not reveal any other significant risk factors.
Table 3
Univariate and multivariate analysis of risk factors for active TB

TB = tuberculosis, HR = hazard ratio, CI = confidence interval, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease, HIV = human immunodeficiency virus.
aAdjusted for gender, age, income level, DM, malignancy, COPD, HIV infection, and silicosis.
![]()
Table 4
HRs and 95% CIs according to type of dialysis

HR = hazard ratio, CI = confidence interval, TB = tuberculosis, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease, HIV = human immunodeficiency virus.
aAdjusted for gender, age, income level, DM, malignancy, COPD, HIV infection, and silicosis; bUsed as a reference variable for estimating the HR of haemodialysis and peritoneal dialysis.
![]()
DISCUSSION
This nationwide cohort study revealed that dialysis was associated with a 4.39-fold higher risk of active TB than among the matched control group. To the best of our knowledge, this is the largest study to investigate the risk of developing active TB after starting dialysis for ESRD. However, the results are consistent with previous reports describing a high risk of active TB among patients with ESRD. For example, one nationwide cohort study from a country with a low incidence of TB11 included 14,506 patients receiving dialysis for ESRD, and revealed that the overall incidence of active TB was 66.8/100,000 person-years. A recent meta-analysis12 also estimated that dialysis was associated with a pooled unadjusted rate ratio of 7.69 (95% CI, 5.94–9.95). Although numerous studies have investigated the relationship between active TB and CKD, most of the previous studies were case reports, case-control studies, small hospital-based cohort studies, or regional registry studies.3 A recent Taiwanese study13 included 4,131 patients with new-onset ESRD and an age- and gender-matched control group, and revealed that ESRD was associated with a 2.40-fold higher risk of developing active TB. The present study also examined a large population-based sample of individuals who were receiving dialysis, and comparison to the matched control group revealed that there was a relationship between active TB and ESRD.
In addition to mortality and morbidity, several issues and burdens related to TB should be highlighted among patients with ESRD. For example, the clinical manifestation of active TB during dialysis is often insidious and atypical,14 as patients with ESRD and TB frequently present with systemic symptoms that are similar to uraemia, which can delay the diagnosis. Patients may also present with extra-pulmonary or disseminated diseases.15 Among patients with CKD, the standard anti-TB treatment involves quadruple therapy, although this is problematic because ethambutol and pyrazinamide are both cleared through the kidney and require renal-adjusted dosing. In addition, rifampicin often interacts with anti-hypertensive, antidiabetic, and immunosuppressive medications, which can necessitate dose adjustments.16 Furthermore, anti-TB medication causes more severe and frequent toxicities among patients with ESRD, including gastrointestinal troubles and decreased appetite, which limits the treatment regimen and duration.17 Screening for latent and active TB infections among patients with ESRD is another important issue for controlling TB. Although the World Health Organization recommends systemic testing for TB among patients who are receiving dialysis or transplantation, there is a paucity of evidence for guiding the screening recommendation, and optimal treatment for latent TB infection is unclear among patients with advanced CKD. Thus, there is a need for clear and consistent guidance to develop suitable protocols for screening, diagnosis, and treatment of TB among patient with CKD.
Haemodialysis and peritoneal dialysis were both associated with increased risks of active TB in the present study, and both modalities share the same risks associated with acquired immunodeficiency due to uraemia. Two previous studies have evaluated the risk of active TB among patients undergoing peritoneal dialysis, and both revealed higher prevalence of TB in this population than among the general population.1819 Although patients undergoing haemodialysis have markedly more frequent hospital visits than those undergoing peritoneal dialysis, the risks of TB between them were not different in the present study, which is consistent with the results from previous studies.1320 Therefore, we speculate that the risk of nosocomial TB infection is not a great concern among patients undergoing dialysis.
Several well-known comorbidities are associated with the risk of active TB.1 In our sub-analyses, patients with diabetes, malignancy, and COPD also had increased rate ratios of active TB, although the multivariate analysis revealed that the associations between these comorbidities and TB were insignificant. We hypothesise that the uraemia-related risk of infection is strong enough to outweigh the influences of these conditions. In addition, HIV infection is another important risk factor for active TB, although the prevalence of HIV infection is low in Korea.21 We only identified one case of active TB among patients with HIV infection and ESRD, which indicates that HIV infection status did not likely confound the relationship between dialysis and TB.
The present study has several limitations that should be considered. First, this study collected data that were based on diagnostic codes and insurance claims, which precluded analysis of information regarding other lifestyle and clinical variables that could influence risk of TB infection. We attempted to control for such confounding using other available data. For example, we included COPD to adjust for the effects of smoking, as COPD is mainly attributed to smoking.22 We also included household income, which represents various factors associated with socio-economic status. Those with a history of anti-TB treatment before study enrolment were excluded in order to minimise the effect of recent TB infection. Although use of immunosuppressant drugs is an important risk factor for active TB development, dialysis patients rarely use immunosuppressants in clinical practice, as dialysis also suppresses the patient's immune function.23 Thus, based on its limited use, we elected to omit immunosuppressant use as a co-variable. Second, dialysis patients might have more frequent visits to clinics and a higher likelihood of receiving appropriate screening (e.g., chest radiography), and would be more likely to seek medical attention if TB symptoms arose. Thus, ascertainment and detection biases might contribute to a higher rate of active TB identification in the dialysis cohort than in the control cohort. Nevertheless, Korea has a single national health insurance service that ensures citizens have easy and inexpensive access to medical care, and the National Health Screening Program provides regular chest radiography examinations for every healthy adult,24 which frequently leads to an early diagnosis of active TB. Thus, although there might be some delays in the control cohort's TB diagnosis, we suspect any underestimation of active TB identification in that cohort would be minimal. Third, the diagnosis of active TB was based on the ICD-10 codes and drug prescription history, which may be associated with limited sensitivity. Diagnosing TB with a specific combination of anti-TB drugs might not be accurate, because these drugs may be prescribed for other infectious diseases, such as non-tuberculous mycobacteria disease. A recent study25 showed that some patients with Mycobacterium avium complex lung disease transiently received anti-TB treatment before its final diagnosis. However, this criterion has been used in various previous studies and meta-analyses. Because Korean law requires all active TB cases to be reported using the ICD-10 codes, we assumed the use of these codes to be a valid and reliable approach.
Despite these limitations, the major strength of the present study is its large sample size, which increased the results' statistical power and accuracy and provides for better generalisability. Furthermore, the dialysis cohort was created using patients with a nephrologist-confirmed diagnosis of ESRD, and both cohorts were designed by an epidemiologist. Finally, the prolonged follow-up was sufficient to examine the temporal relationship between the onset of ESRD and subsequent active TB.
In conclusion, the present study revealed epidemiological evidence that receiving dialysis for ESRD was associated with an increased risk of developing active TB. Although there is accumulating evidence regarding the effects of TB and ESRD on public health, international societies have only recently recommended systematic TB testing for patients receiving dialysis, and current guidelines are still ambiguous.3 Therefore, there remains a need for detailed and well-organised guidelines for identification of active TB cases among patients with ESRD.
 XML Download
XML Download