

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular complications are the major causes of morbidity and mortality in patients with chronic kidney disease (CKD).1 The prevalent form of vascular calcification (VC) in CKD is medial VC leading to the increased vascular stiffness which causes the loss of capacity of buffering cardiac load, left ventricular hypertrophy and relative ischemia of myocardium to culminate in the increased cardiovascular complications in this patient population.2 VC actually constitute a major component of chronic kidney disease-mineral and bone disorder (CKD-MBD) along with bone disorder implicating that VC and bone disorder are closely related each other in CKD.3
Osteoprotegerin (OPG), a soluble decoy receptor inhibiting the signals from receptor activator of nuclear factor kappa-B ligand (RANKL), has increasingly been recognized to play an important role in VC and bone disorder.4 OPG released from osteocyte and osteoblast inhibits the activation of osteoclast to prevent excessive bone resorption. OPG from endothelial cells and vascular smooth muscle cells (VSMCs) inhibit RANKL-induced trans-differentiation of VSMCs into calcified VSMCs with osteoblastic phenotype.5 Hence OPG is an attractive candidate involved in pathogenesis of CKD-MBD. Actually, a previous study using the data from the same cohort used in this study reported the inverse relationship between serum OPG and bone mineral density in pre-dialysis CKD patients.6
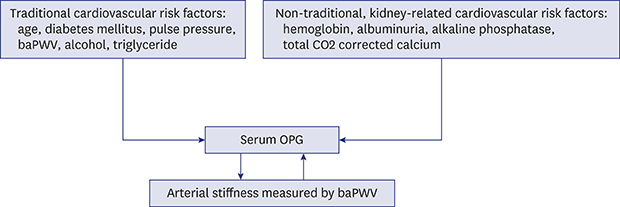
Serum OPG was elevated in patients with cardiovascular events such as ischemic heart disease,7 heart failure,8 and peripheral vascular disease9 which are major causes of morbidity and mortality in patients with CKD. Moreover, serum OPG was reported to be related to the surrogate markers of atherosclerosis such as intimal-medial thickness of carotid artery even in asymptomatic patients in metabolic syndrome,10 stress echocardiography in type 2 diabetes mellitus (DM) with silent myocardial infarction,11 and flow-mediated vasodilation of brachial artery in pre-dialysis CKD12 suggesting the role of OPG as one of excellent biomarkers of cardiovascular disease. Thus, it is tempting to search for traditional and non-traditional, kidney-related cardiovascular risk factors which correlate with serum OPG in CKD. In this study, we cross-sectionally analyzed the baseline data obtained at enrollment in a multi-center prospective CKD cohort study in Korea with aims to find the non-traditional, kidney-related cardiovascular risk factors correlated to serum OPG and to assess the effect of serum OPG on the brachial ankle pulse wave velocity (baPWV) which reflects medial VC in peripheral and central arterial system in patients with the pre-dialysis CKD.
METHODS
Study populations
Korean Cohort Study for Outcome in Patients with Chronic Kidney Disease (KNOW-CKD) is currently on-going prospective CKD cohort study inaugurated January 2012 (ClinicalTrials.gov accession number NCT016304860) in which 9 tertiary university hospitals in Korea are participating with the aim to investigate the renal or cardiovascular outcomes of Korean patients with pre-dialysis CKD. The detailed design and method of the KNOW-CKD study was previously published elsewhere.13 Out of 2,238 adult CKD patients aged 20 to 75 years enrolled between 2011 and 2015, baPWV and serum OPG were both measured in 1,913 patients. Because the obliterative arterial lesion in lower limb seriously influence the value of baPWV,14 we finally choose 1,832 patients whose ankle-brachial index were larger than 0.9 in both limbs (Fig. 1).
Data collection and measurements
Baseline information related to age, sex, smoking, alcohol consumption, and medical history was provided by the patient with the aid of trained person. Anthropometric measurement and blood pressure measurement were carried out by the trained nurse. Hypertension was defined as a systolic blood pressure (SBP) > 140 mmHg, diastolic blood pressure (DBP) > 90 mmHg, self-reported history of hypertension, or current use of antihypertensive medication. DM was defined as a fasting serum glucose > 126 mg/dL or self-reported history of diabetes or current use of diabetic medication. Hypercholesterolemia was defined as fasting total cholesterol > 240 mg/dL or current use of lipid-lowering drugs. Coronary artery disease (CAD) was defined by self-reported history of angina or myocardial infarction without any further verification by laboratory, electrocardiography, echocardiography or imaging studies.
Blood sample were obtained after overnight fasting, centrifuged within 1 hour after collection. Glomerular filtration rate was estimated by Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) Cr equation using serum creatinine level measured by isotope dilution mass spectrometry (IDMS)-traceable method in central laboratory. Urine albumin-creatinine ratio (UACR) was measured using first void urine sample in the central laboratory. All other laboratory measurement in blood and urine sample were measured in each participating center.
Measurement of serum OPG concentration
As reported previously,6 we measured serum OPG (BioVendor R&D, Brno, Czeck Republic) by using enzyme-linked immunosorbent assay kit in the central laboratory (Lab Genomics, Seongnam, Korea). Intra-assay coefficients of variations was < 4.9% and inter-assay coefficients of variations was < 9.0%. Sample assays were done in duplicate. Mean values were used for reporting results.
Measurement of baPWV
A VP-1000 analyzer (Collin Co., Komaki, Japan) was used for measuring baPWV. As reported previously,15 this device takes a measurement of ankle-to-brachial index by using the electrocardiogram, phonocardiogram, and pressure waveforms. Pressure waveforms of the brachial and tibial arteries were documented with plethysmographic and oscillometric pressure sensors using occlusion/sensing cuffs that were twined around both arms and both ankles. The time intervals between pressure waveforms of the brachial and tibial arteries (pulse transit time) were checked, and baPWV were automatically computed by the VP-1000 analyzer using the formula below:
where Lb is 0.2195 × patient's height (cm) − 2.0734 and La is 0.8129 × patient's height (cm) + 12.328. The mean value of the right and left baPWV (mean baPWV) was used for this study.
Statistical analysis
The normal distributions of variables were examined by Kolmogorov-Smirnov test or Shapiro-Wilk test. Categorical variables were presented as the number and percentage and continuous variables are expressed as mean ± standard deviation. The characteristics of study population across the quartile value of serum OPG were compared by the Pearson's χ2 test for categorical variables and the Kruskal-Wallis test for continuous variables. The Jonckheere-Terpstra test and linear by linear association were used to evaluate the P for trend for continuous variable and categorical variables respectively. The variables related to serum OPG were examined by stepwise multiple linear regression using variables with P value < 0.05 in comparison between quartile groups of serum OPG. The characteristics of study population across the quartile value of mean baPWV were compared by the Pearson's χ2 test for categorical variables and the Kruskal-Wallis test for continuous variables. The Jonckheere-Terpstra test and linear by linear association were used to evaluate the P for trend for continuous variable and categorical variables respectively. The variables related to mean baPWV were examined by stepwise multiple linear regression using variables with P value < 0.05 in comparison between quartile groups of mean baPWV. The difference of mean baPWV between OPG quartile using the lowest quartile group as reference was examined by linear mixed model. All statistical analyses were carried out by software SPSS version 22 (IBM Corp., Armonk, NY, USA) and statistical significance was defined as P value < 0.05 at both tails.
Ethics statement
All study population provided written informed consent. This study was carried out in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board at each participating clinical center — i.e., Seoul National University Hospital (1104-089-359), Seoul National University Bundang Hospital (B-1106/129-008), Yonsei University Severance Hospital (4-2011-0163), Kangbuk Samsung Medical Center (2011-01-076), Seoul St. Mary's Hospital (KC11OIMI0441), Gil Hospital (GIRBA2553), Eulji General Hospital (201105-01), Chonnam National University Hospital (CNUH-2011-092), and Pusan Paik Hospital (11-091) in 2011. The protocol summary is also registered at the ClinicalTrials.gov with accession number NCT01630486.
RESULTS
Baseline demographic and clinical characteristics of study population
The mean age of 1,832 study population was 52.9 ± 12.3 years; and the number of females was 736 constituting 40.2% of population. DM, hypertension, hypercholesterolemia and CAD were present in 32.6%, 95.7%, 56.1% and 4.9%, respectively. The percentage of alcohol drinker was 86.1%; and 46.2% of study population were current smoker or ex-smoker. The body mass index (BMI) and waist-hip ratio (WHR) were 24.5 ± 3.5 kg/m2 and 0.90 ± 0.07, respectively. The mean estimated glomerular filtration rate (eGFR) was 53.4 ± 31.5 mL/min/1.73 m2; and UACR was 862.9 ± 1,335.1 mg/g.
Characteristics of study population according to quartile group of serum OPG
The serum OPG concentration was 6.76 ± 3.45 pmol/L with range of 1.66 to 44.20 pmol/L with interquartile interval of 4.45 to 8.11 pmol/L. The characteristics of study populations according to quartile groups of serum OPG are shown in Table 1. The populations in increasing quartile of OPG were older and had more frequent history of DM, hypertension, CAD, and hypercholesterolemia. There was less frequent alcohol drinker in higher quartile group but there was no difference in the frequency of smoker. While SBP and pulse pressure (PP) were higher in higher quartile groups, DBP was lower in higher quartile group. The higher quartiles of serum OPG was associated with lower eGFR and higher urinary excretion rate of albumin suggesting that they had more severe CKD. There were significant differences in CKD-MBD markers. Increasing quartile OPG groups were characterized by increasing higher serum phosphorous and total alkaline phosphatase (ALP) and decreasing corrected calcium, and bone mineral density measured at femur head. Also, C-reactive protein (CRP), a well-known inflammatory marker, tended to be higher in the patients in higher OPG quartile. Importantly, as the OPG quartile increased, mean baPWV progressively increased.
Table 1
Demographics, clinical and laboratory findings according to the quartile values of serum OPG (pmol/L)

Quartile values of serum OPG: Quartile 1, 1.66–4.45 pmol/L; Quartile 2, 4.46–5.95 pmol/L; Quartile 3, 5.96–8.105 pmol/L; Quartile 4, 8.106–44.2 pmol/L.
OPG = osteoprotegerin, DM = diabetes mellitus, HTN = hypertension, CAD = coronary artery disease, BMI = body mass index, WHR = waist-hip ratio, SBP = systolic blood pressure, DBP = diastolic blood pressure, PP = pulse pressure, MBP = mean blood pressure, eGFR = estimated glomerular filtration rate, FBS = fasting blood sugar, ALP = alkaline phosphatase, TC = total cholesterol, LDL = low density lipoprotein, HDL = high density lipoprotein, TG = triglyceride, TCO2 = total CO2, CRP = C-reactive protein, UACR = urine albumin-creatinine ratio, baPWV = brachial-ankle pulse wave velocity.
![]()
Independent variables associated with serum OPG concentration
We analyzed the variable associated with serum OPG by stepwise multivariate linear regression as shown in Table 2. Traditional cardiovascular risk factors such as age, DM, PP, triglyceride, and alcohol drinker were significantly associated with serum OPG. Age was the most important variable associated with the serum OPG explaining 28.6% of serum OPG value. The 10 years increment of age was associated with the increase in serum OPG by 0.94 pmol/L. The brachial-ankle pulse wave velocity, which reflects central and peripheral vascular stiffness and PP, was independently associated with serum OPG. The 100 cm/sec increment of mean baPWV was associated with the increase in serum OPG by 0.1 pmol/L. DM, in which medial VC is known to be prominent, was also associated with serum OPG. Alcohol drinking was negatively associated with serum OPG. With regard to kidney-related factors, eGFR was not associated with serum OPG while urine albumin excretion showed relatively strong association with serum OPG. The other kidney-related factors significantly associated with serum OPG included serum level of hemoglobin, total CO2 content, ALP and corrected calcium. Serum hemoglobin, total CO2 content, and corrected calcium were negatively associated with serum OPG while positive association between serum ALP and OPG was observed.
Table 2
Independent variables associated with serum OPG in stepwise multivariate linear regression

OPG = osteoprotegerin, CI = confidence interval, UACR = urine albumin-creatinine ratio, baPWV = brachial-ankle pulse wave velocity, DM = diabetes mellitus, PP = pulse pressure; TCO2 = total CO2.
![]()
Characteristics of study population according to the quartile value of mean baPWV
The mean baPWV was 1,592.9 ± 339.1 cm/sec with range of 857.5 to 4,632.5 cm/sec and interquartile interval of 1,293.4 to 1,701.5 cm/sec. The characteristics of study populations are shown in Table 3. The populations in increasing quartile of mean baPWV were older and had more frequent history of DM, hypertension, CAD, and hypercholesterolemia. The higher mean baPWV groups had more frequent smokers and less frequent alcohol drinker. BMI, WHR and blood pressure were higher in higher quartile groups. DBP which was different across the quartile group of serum OPG was not different between mean baPWV groups. The higher quartiles of mean baPWV was associated with lower eGFR and higher urinary excretion rate of albumin suggesting that they had more severe CKD. There was significant difference in CKD-MBD markers. Increasing quartile groups of mean baPWV were characterized by increasing higher serum phosphorous and total ALP and decreasing corrected calcium, and bone mineral density measured at femur head. Also, CRP, a well-known inflammatory marker, tended to be higher in the patients in higher OPG quartile. The prescription rates of cholesterol-lowering drugs, beta blocker, calcium channel blocker, and alpha blocker were higher in higher quartile group of mean baPWV while there were no difference in prescription rates of angiotensin converting enzyme inhibitor, angiotensin receptor antagonist, and minoxidil. Importantly, as the mean baPWV quartile increased, serum OPG progressively increased.
Table 3
Demographics, clinical and laboratory findings according to the quartile values of mean baPWV (cm/sec)

Quartile values of mean baPWV: Quartile 1, 857.5–1,293.4 cm/sec; Quartile 2, 1,293.5–1,460.5 cm/sec; Quartile 3, 1,460.6–1,701.5 cm/sec; Quartile 4, 1,701.6–4,632.5 cm/sec.
baPWV = brachial-ankle pulse wave velocity, DM = diabetes mellitus, HTN = hypertension, CAD = coronary artery disease, BMI = body mass index, WHR = waist-hip ratio, SBP = systolic blood pressure, DBP = diastolic blood pressure, PP = pulse pressure, MBP = mean blood pressure, eGFR = estimated glomerular filtration rate, FBS = fasting blood sugar, ALP = alkaline phosphatase, TC = total cholesterol, LDL = low density lipoprotein, HDL = high density lipoprotein, TG = triglyceride, TCO2 = total CO2, CRP = C-reactive protein, UACR = urine albumin-creatinine ratio, OPG = osteoprotegerin, LLD = lipid lowering drug, CPB = calcium containing phosphorus binder, VTD = vitamin D, AVD = active vitamin D, ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin receptor blocker, CCB = calcium channel blocker.
![]()
Independent variables associated with mean baPWV
We analyzed the variable associated with mean baPWV by stepwise multivariate linear regression as shown in Table 4. Age was the most important variable associated with the mean baPWV explaining 29.2% of mean baPWV value. The 10 years increment of age was associated with the increase in mean baPWV by 96.19 cm/sec. OPG was the second most important variable for mean baPWV explaining 7.4% of mean baPWV. The increment of serum OPG by 1 pmol/L was associated with the increase of mean baPWV by 17.1 cm/sec. The bone mineral density measured at femur neck was inversely associated with mean baPWV. eGFR was not associated with mean baPWV while urinary albumin excretion was. Also included variables were SBP and DM.
Table 4
Independent variables associated with mean baPWV in stepwise multivariate linear regression

baPWV = brachial-ankle pulse wave velocity, CI = confidence interval, OPG = osteoprotegerin, SBP = systolic blood pressure, DM = diabetes mellitus, UACR = urine albumin-creatinine ratio.
![]()
Comparison of mean baPWV according to the quartile groups of serum OPG
To further evaluate the association of OPG with mean baPWV, we compared mean baPWV of the quartile group OPG with lowest quartile group as reference by linear mixed model as shown in Table 5. Mean baPWV of 2nd, 3rd, and 4th quartile group of OPG were significantly higher than that of 1st quartile group in model adjusted by age and sex (P value = 0.002, < 0.001, < 0.001, respectively). In model adjusted by age, sex and all significant variable for mean baPWV, mean baPWV of 3rd and 4th quartile group of OPG were significantly higher than that of 1st quartile group of serum OPG. (P value = 0.009, < 0.001 respectively)
Table 5
Mean pulse wave velocity (cm/sec) compared with reference quartile by quartiles of serum OPG

OPG = osteoprotegerin, SD = standard deviation, DM = diabetes mellitus.
aAdjusted by age and sex; bAdjusted by age, sex, OPG, systolic blood pressure, DM history, T-score of femur neck, urine albumin-creatinine ratio.
![]()
DISCUSSION
Main findings in this study were; 1) along with traditional cardiovascular risk factors, non-traditional, kidney-related factors are associated with serum OPG in CKD, 2) serum OPG concentration was significantly associated with baPWV in multivariate regression, and 3) the baPWV was significantly higher in higher quartile groups of OPG than lowest quartile group in a model fully adjusted by sex, age and all significant variables for baPWV. Through these findings, the close association of serum OPG concentration with kidney-related cardiovascular risk factors and arterial stiffness in pre-dialysis CKD was robustly demonstrated. Although a few previous studies in pre-dialysis CKD1617 also reported the similar findings, this study is much more comprehensive in that; 1) the number of study population was much larger, 2) study population encompass wide range of eGFR and albuminuria, two most important index determining the severity of CKD, and 3) extensive use of variables encountered in clinical practice such as demographic, physical, laboratory finding, comorbidities and medications in analysis.
Serum OPG were positively related to traditional cardiovascular risk factors such as old age, smoking, DM, SBP, CRP in studies from general population.8181920 In agreement with those studies, old age, DM, and PP were also related to serum OPG in this study. The insignificant relation of smoking to serum OPG in this study needs several discussions. The prevalence of smoker was relatively higher in our study (46.1%) than these general population studies (13% to 31.7%). Moreover, smoking status were defined as current smoker in general population studies while ex-smoker in addition to current smoker was included as smoker in our study. Additionally, already high enough risk of CKD for cardiovascular events might dilute the effect of smoking on serum OPG. Consistent with this study, previous study about pre-dialysis CKD patients also showed no difference in smoking status across serum OPG groups.17 Total cholesterol level was negatively associated with serum OPG in Framingham cohort19 whereas the reverse association was found in other studies.161820 The increased usage of cholesterol-lowering drugs might complicate these relationship as in this study where medical history of hypercholesterolemia was positively but serum cholesterol level was negatively associated with serum OPG. Counterintuitively, serum triglyceride was negatively associated with serum OPG, as shown in a previous study.20
Because the study population in this study is pre-dialysis CKD, non-traditional, CKD-related risk factors for cardiovascular disease such as albuminuria, serum level of ALP, corrected calcium, total CO2 content and hemoglobin demonstrated significant associations with serum OPG in this study. Estimated GFR, the most important variable of CKD, was not associated with serum OPG in multivariate analysis in our study. Several previous studies in pre-dialysis CKD121617 or kidney transplant recipients21 demonstrated graded decrease in eGFR across the increased serum OPG group in univariate analysis as also shown in this study. However, analysis for the relation of eGFR to serum OPG, adjusted by other variables, were not done in those studies. Furthermore, the number of study subjects in those studies was relatively small with consequent limited statistical power. The lack of an association between eGFR and OPG implies that the complications of CKD, such as hypertension, dyslipidemia, disturbance of mineral metabolism, rather than decreased GFR itself, may lead to damage to bone and vasculature. Therefore, the increased release of OPG into the circulation and intensive control of these CKD complications could ameliorate bone and vasculature disorders in CKD. Although albuminuria was not associated with serum OPG in a subset of CRIC cohort,16 a very large meta-analysis involving 105,872 CKD subjects revealed that graded increase in albuminuria was associated with progressive cardiovascular mortality up to 9.49 folds across the whole range of eGFR.1 Thus, it is not surprising to observe the significant association of albuminuria with serum OPG in this study. The correlation between albuminuria and serum OPG was also reported in study subjects with type 2 DM although multivariate analysis was not performed.22
The serum OPG was widely reported to be related to osteoporosis and fracture which is an important component of CKD-MBD.3 In biologic experiment, OPG deficient mice exhibited severe osteoporosis and fracture beginning from 2 weeks after birth.23 And the sequence variant in OPG gene was associated with bone mineral density and osteoporotic fracture in a large human study.24 A large population study demonstrated the association between higher serum OPG and the increased incidence of hip fracture in men and woman not taking hormonal therapy.25 The association of higher serum OPG with the increased incidence of low-trauma fracture was also reported in patient with stage 3–5 CKD.26 We also observed that increased serum OPG was related to decreased bone mineral density of femur neck in this study. And a previous study from KNOW-CKD cohort also reported the similar findings.6 While a few previous studies demonstrated association of CKD-MBD parameters such as serum calcium, phosphorous and parathyroid hormone with serum OPG,2027 these association was not observed in another study.16 In our study, well known parameters of CKD-MBD (decreased serum levels of corrected calcium and increased ALP level), and decreased total CO2 content were significantly correlated with serum OPG. Taken together, these findings suggest that disordered bone metabolism from mineral disturbance and metabolic acidosis induce compensatory release of OPG from osteocyte and osteoblast. In addition, increased VC secondary to increased calcium influx into VSMC from disordered bone metabolism might evoke enhanced secretion of OPG.
Serum OPG was reported to be associated with various surrogate markers of vascular injury such as coronary artery calcium score,1728 abdominal aorta calcium score,29 intima-media thickness of carotid artery,30 flow-mediated vasodilation of carotid artery,12 and pulse wave velocity16 in patients with CKD. Several studies about the relationship between PWV and OPG in end-stage renal disease (ESRD) were published.3132 In these studies, PWV was positively associated with age, hypertension and OPG levels which is consistent with the findings in our study. After multivariate analysis, age, OPG, SBP, history of diabetes, T-score of femur neck, UACR was shown to be independent variables associated with baPWV in our study. In ESRD studies, OPG and age were also independent variables for PWV in multivariate analysis. Thus, OPG has been commonly shown as an independent variable predicting PWV in CKD studies. Unlike previous studies, T-score of femur neck and albuminuria were related to baPWV in this study. Inverse correlation of bone mineral density with baPWV is quite consistent with the concepts in CKD-MBD implicating that bone disorder and VC are interrelated phenomenon in CKD. It has been already well reported that albuminuria was significantly associated with PWV in non-diabetic, non-hypertensive patients33 and hypertensive patients.34 This study also demonstrated that this association also existed in pre-dialysis CKD patients. We also found that the baPWV of the highest and second highest OPG quartile are significantly higher than that of the lowest OPG quartile after adjustment of all independent variables found from multivariate analysis. Consistent with this finding, Scialla et al.16 also reported that the highest tertile of OPG had 10% higher aortic PWV than the lowest tertile of OPG in CKD patients. Taken together, these findings further strengthen the relation between OPG and PWV. The meta-analysis of 17 longitudinal studies involving 10,820 low risk general population and 5,077 high risk patients such as hypertension, CAD and renal disease demonstrated that PWV was strong predictor of future cardiovascular events and all-cause mortality.35 The strong relationship of OPG with mean pulse wave velocity (MPWV) therefore suggest that serum OPG would be an excellent biomarker for cardiovascular events. Serum OPG was inversely related to global longitudinal strain and strain rate in type 2 DM patients having chronic heart failure.36 Serum OPG was also associated with the number of circulating endothelial-derived and mononuclear-derived progenitor cells37 and the ratio of endothelial-derived microparticle originating from apoptotic cells to from healthy endothelial cells in metabolic syndrome and DM.38 These findings further strengthen the role of serum OPG as a biomarker of cardiovascular damages.
Many laboratory studies suggest that OPG protect against the VC via inhibition of RANKL signaling. OPG deficient mice exhibited severe osteoporosis and medial VC beginning from 2 weeks after birth.23 The administration of recombinant OPG to ldlr(−/−) mice fed on atherogenic diet significantly inhibit VC.39 The OPG protein and mRNA were detected mainly in area adjacent to calcification in human blood vessel.40 These studies suggest that elevated serum OPG in our study is the result of compensatory response to protect blood vessel, bone, and other tissues against the damage induced by CKD.
This study has several limitations; 1) because of cross-sectional nature of this study, the relations of serum OPG to PWV and other kidney-related cardiovascular risk factor are simple associations. Therefore, we do not know whether these associations are simple epiphenomenon or causal relation, 2) this study did not provide answer to paradoxical association of increased serum OPG with increased PWV despite vessel-protecting function of OPG, 3) there is unavoidable some ambiguity in variables used for analysis. For example, medical history of CAD reported in patients was not verified by relevant tests, the influence of medications on blood pressure measurements and lipid profiles were not ascertained.
In summary, our study demonstrated that there were non-traditional, kidney-related cardiovascular risk factors correlated with serum OPG. Serum OPG was closely related to vascular stiffness in pre-dialysis CKD.
 XML Download
XML Download