

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aortic valve sclerosis (AVS) is defined as an abnormal valve morphology in the absence of a hemodynamically significant valve orifice obstruction, and is regarded as a precursor to aortic valve stenosis.1) AVS and aortic valve stenosis, characterized by increased leaflet thickness, stiffening and calcification, are common in the elderly population.2) There is increasing evidence that this condition is regulated by active cellular processes, including complex inflammation-related mechanisms. Several population-based longitudinal studies have found that cardiovascular risk factors such as hypercholesterolemia impact the development of degenerative aortic valve stenosis.3) Wierzbicki and Shetty4) described an ‘early lesion’ resembling the early lesions in atherosclerotic plaques, and proposed classifying calcific aortic stenosis as an atherosclerotic disease.
Therefore, it seems logical to hypothesize that the modification of atherosclerotic risk factors would slow the progression of aortic valve stenosis.5) General experimental support for this hypothesis has been provided by animal model studies; however, statins do not appear to have a specific role in the progression of aortic stenosis.6)7) Due to the limited and inconsistent data available, there remains a question about the therapeutic role of statins in human patients with AVS.8)9)10)
The aim of our study was to evaluate the effects of statins on the progression of AVS, an early stage of aortic valve lesions.
METHODS
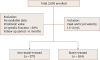
We retrospectively analyzed the echocardiograms of all patients with AVS diagnosed by 2-D and Doppler echocardiography (irregular leaflet thickening, focally increased echogenicity on 2-D echocardiogram and increased peak aortic valve velocity [> 1.5 and < 2 m/s] on Doppler echocardiogram), and subsequently selected patients who had undergone at least two echocardiography examinations at least 6 months apart from August 2010 to August 2015. Initially, 3,695 patients were enrolled. The exclusion criteria included the presence of other significant valvular diseases, left ventricular dysfunction (left ventricular ejection fraction < 40%), congenital heart disease, cardiomyopathy, a permanent pacemaker, uncontrolled tachycardia or bradycardia and a history of cardiac surgery. Of the 3,695 candidate patients, 541 were included in the present study (Figure 1).
Clinical data including the medical history and presence of risk factors were obtained by a complete review of each patient's medical records. The presence of hypercholesterolemia (total cholesterol > 200 mg/dL or use of lipid-lowering therapy), diabetes mellitus (fasting plasma glucose > 126 mg/dL, plasma glucose level [anytime] > 200 mg/dL or use of antidiabetic medication), hypertension (blood pressure ≥ 140/90 mmHg or use of antihypertensive medication) and coronary artery disease (previously documented myocardial infarction or coronary artery stenosis with a lumen diameter > 50% on angiography) were recorded. The progression rate of AVS was expressed as the increase in peak velocity per year (m/s/yr). Inclusion in the statin-treated group required patients to have been prescribed a statin during the study follow-up period.
This study was approved by the Ethical Review Board of our institution.
Echocardiography
Comprehensive transthoracic echocardiography was performed on commercially available equipment (Vivid E9, GE Healthcare, Milwaukee, WI, USA or Acuson SC2000, Siemens Medical Solutions, Mountain View, CA, USA). Standard M-mode, 2-D and color Doppler imaging were performed in parasternal, suprasternal, substernal, and apical views with positional adjustment of the patients. The first and last echocardiograms taken during the study period were used to evaluate echocardiographic changes. Anatomic measurements were made according to the ASE guidelines.11)
Statistical analysis
Continuous variables are shown as the mean ± standard deviation (SD). Mean values were compared with independent t-tests. Categorical variables are presented as frequencies or percentages. Differences in categorical variables were analyzed using the chi-square test. Pearson's correlation coefficients were used to evaluate correlations. Stepwise multiple linear regression analysis was used to identify the independent predictors of AVS progression. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed with SPSS for Windows software (ver. 18.0, SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline patient characteristics
Tables 1 and 2 display the initial clinical and echocardiographic characteristics of each group. Of the 541 patients, 214 (40%) were men and 327 (60%) were women. The mean age was 70 ± 11 years. Statins were prescribed to 264 patients (45%). Of these, 191 (72%) began taking statins after their first echocardiography examination, while the remaining 73 (28%) had taken statins before.
Table 1
Clinical characteristics
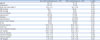
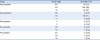
Table 2
Echocardiographic characteristics

The two treatment groups did not differ in age, gender, or smoking status. Relative to the non-statin-treated group, the statin-treated group included a higher proportion of patients with hypertension, hyperlipidemia, diabetes, ischemic heart disease, and stroke. In addition, the levels of C-reactive protein (CRP) and hemoglobin A1c (HbA1c) were elevated in the statin-treated group (p = 0.020 and p = 0.001, respectively; Table 1). The levels of low-density lipoprotein (LDL) at follow-up were available for 356 patients (153 in the non-statin-treated group, 203 in the statin-treated group), and were significantly lower in the statin-treated group (p < 0.001). The baseline echocardiographic parameters were similar in the two groups, with the exception of the left atrial volume index, which was significantly higher in the non-statin-treated group (p = 0.003). Table 3 displays the different types and doses of statins that were prescribed in the statin-treated group.
Progression rate of AVS
The mean follow-up duration was 24.9 ± 13.3 months for the statin-treated group and 24.1 ± 12.4 months for the non-statin-treated group (p = 0.460). The mean initial and follow-up peak aortic jet velocities were also similar in the two groups (Table 2). There was no difference in the progression rate of AVS between the statin-treated group and the non-statin-treated group (0.012 ± 0.340 vs. 0.014 ± 0.245 m/s/yr, respectively, p = 0.956; Table 2, Figure 2A).
Figure 2
Peak aortic jet velocity rate of progression: with or without statin treatment in all study patients (A); with or without statin treatment in patients who were followed up for more than 1 year (B); with or without statin treatment in patients who were followed up for more than 2 years (C); and according to changes in low-density lipoprotein (LDL) levels (D). Bars are the mean ± SD.

We next stratified patients based on the duration of follow-up evaluation. Of those who were followed up for more than one year (n = 441), 211 were prescribed statins. In this subset of patients, the progression rate of AVS also did not differ between the two treatment groups (0.024 ± 0.217 vs. 0.019 ± 0.199 m/s/yr, p = 0.263; Figure 2B). A total of 246 patients received more than 2 years of follow-up evaluations, and the progression rate of AVS was again similar between the two groups (0.007 ± 0.111 vs. 0.000 ± 0.106 m/s/yr, p = 0.621; Figure 2C). Finally, we divided patients into two groups according to whether their LDL levels decreased over the course of the study. Follow-up LDL levels were available for 356 patients, of whom 239 had reduced LDL levels. The progression rate of AVS did not differ between the two groups (0.008 ± 0.249 vs. 0.011 ± 0.329 m/s/yr, p = 0.924; Figure 2D).
Multiple regression analysis for factors associated with AVS progression
A stepwise multiple regression analysis was carried out to identify the specific factors associated with increases in the maximum aortic jet velocity per year. Univariate analysis showed the progression rate of AVS was significantly related to age, body mass index, E/e’ and initial peak aortic jet velocity (Table 4). All variables with p-values < 0.10 in the univariate analysis were entered into the model. The annual progression rate was only influenced by the initial peak aortic jet velocity (β = 0.153, p = 0.009; Table 4).
Table 4
Association of the rate of aortic valve sclerosis progression with clinical and echocardiographic parameters

DISCUSSION
In this study, statins did not appear to influence the mean progression rate of AVS. Some retrospective studies in humans have suggested that statin therapy might slow the progression of aortic stenosis.12)13)14)15) In addition, a prospective study (Rosuvastatin Affecting Aortic Valve Endothelium [RAAVE]) revealed that the rate of disease progression was significantly slower in hypercholesteremic patients treated with rosuvastatin than in untreated patients with normal cholesterol levels.16) However, three recent prospective randomized studies found neither regression nor reduction in the progression of aortic stenosis in statin-treated patients: SEAS (Simvastatin and Ezetimibe in Aortic Stenosis),17) SALTIRE (Scottish Aortic Stenosis and Lipid Lowering Trial, Impact on Regression)18) and ASTRONOMER (Aortic Stenosis Progression Observation: Measuring Effects of Rosuvastatin).19) Finally, a meta-analysis that included 10 studies with 3,822 participants (2,214 non-statin-treated and 1,608 statin-treated) did not support the use of statins to improve outcomes or reduce disease progression in patients with non-rheumatic calcific aortic valve stenosis.20)
Several studies have examined the role of statins in the progression of AVS. In 2005, Antonini-Canterin et al.8) reported that the rate of change in peak aortic velocity (Vmax) was significantly lower in statin-treated patients than in non-statin-treated patients (0.04 ± 0.04 vs. 0.08 ± 0.06 m/s/yr, p = 0.007). However, the number of patients with AVS in this study was low (n = 52; 26 statin-treated, 26 controls). An additional study involving a large number of patients with long-term follow-up demonstrated that statins effectively slowed the progression of aortic valve disease in AVS. The progression rate of AVS was 0.04 ± 0.09 m/s/yr in patients receiving statins and 0.07 ± 0.10 m/s/yr in untreated patients (p = 0.01).21) In contrast, in animal models, the cellular response to statin therapy did not result in full regression of the sclerotic process in established AVS.9)
To validate these limited and conflicting findings, we assessed a large human patient population and determined whether statin treatment improved AVS progression. We did not find a link between statin treatment and the rate of disease progression. Given the higher baseline risk for stenosis progression in the statin-treated group (higher prevalence rates of hypertension, diabetes, ischemic heart disease and stroke, and higher CRP levels) and the fact that Vmax did not increase in statin-treated patients with AVS, it is plausible that statins have beneficial effects, since more rapid disease progression could be expected in this group.
In our study, the mean follow-up period was shorter than those in previous studies. For example, in the reports by Antonini-Canterin et al., the mean follow-up durations were 54 ± 34 months in 20058) and 5.6 ± 3.2 years in 2008.21) AVS is a slowly progressing disease. Therefore, the duration of follow-up in our study may have been too short to detect differences in the disease progression rate between the two groups.
The mean progression rate was 0.012 ± 0.340 m/s/yr in the statin-treated group and 0.014 ± 0.245 m/s/yr in the non-statin-treated group. These values were lower than those in previous studies8)21) and consistent with results in patients with aortic stenosis. In a previous study involving Korean patients,22) the progression rate of aortic stenosis was similar to that found in Japanese patients but slower than those reported for the Western population. Ethnic differences have also been reported for aortic valve calcification, which plays an important role in the progression of AVS.23) Therefore, ethnicity and other as-yet unrecognized factors may influence the progression rate of AVS. More research is needed in this area.
Multivariate analysis revealed that the initial peak aortic jet velocity was the only independent predictor of the AVS progression rate. Previously, Palta et al.24) reported that the initial aortic valve area (AVA), smoking status, and serum calcium levels were associated with the progression of aortic stenosis. Also, Bahler et al.25) found that the severity index (based on valve calcification and mobility) was an independent predictor of aortic stenosis progression, as was the initial AVA. However, in our study, no severity index of aortic valvular calcification was used, and the smoking status and serum calcium levels did not appear to be associated with the progression of AVS.
This study had several limitations. First, due to the retrospective study design, we encountered incomplete records of clinical and echocardiographic parameters. Second, we did not grade aortic valve calcification based on echocardiography. Aortic valve calcification has been shown to be associated with more rapid progression of aortic stenosis.26) However, we believe that the quantitation of aortic valve calcification by echocardiography is not reliable, because it relies heavily on the machine settings, image quality and echocardiographer experience. Third, we could not analyze the data according to the type and dose of statin, due to the small sample size. Lastly, the retrospective nature of this study limited the participants to a single center and a single ethnicity. Therefore, our findings should be expanded and further verified in well-controlled prospective studies.
In conclusion, our retrospective study demonstrated that statin treatment had no effect on the progression of AVS. The progression rate of AVS observed herein was slower than that in the Western population. Therefore, well-designed, prospective, large-volume randomized controlled studies including participants from all races are needed to further define the prognosis and specific management of AVS.
 XML Download
XML Download