

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease is a major cause of death and hospitalization, and ischemic heart disease (IHD) is one of the most frequent causes of cardiovascular death and heart failure (HF) requiring hospitalization.1)2) Although the mortality of IHD has been recently decreasing due to the introduction of newly developed drugs and interventional methods, early detection and management of prognostic factors is still an important basis to reduce the cardiac adverse events. Recent studies showed that old age, co-morbidity such as diabetes mellitus or chronic kidney disease (CKD), left ventricular systolic and diastolic functions are related to the prognosis of patients with IHD.3)4)5)
Acute heart failure (AHF) is a common and potentially fatal cause of acute respiratory distress in patients with IHD, regardless of whether they presented as acute coronary syndrome or not. In Korea, IHD was the major underlying disease which resulted in AHF and the most frequent cause of HF aggravation was myocardial ischemia.6) In patients with AHF, diastolic dysfunction, especially restrictive filling pattern (RFP) of left ventricle (LV), is associated with mortality and re-hospitalization.7) Based on 2 recent literature-based meta-analyses, the presence of the RFP was associated with a 4-fold increase of death after acute myocardial infarction (AMI) or AHF.8)9)
However, prognostic implications of diastolic dysfunction in patients with IHD have been rarely investigated in Korea. This study aimed to evaluate the clinical impact of RFP of LV on the long-term mortality in patients with IHD presenting as AHF.
METHODS
Study subjects
Among 669 patients who admitted to Jeju National University Hospital as AHF from January 2005 to April 2016, 138 patients with IHD as an underlying disease and sinus rhythm during echocardiographic study were enrolled in this study. Patients with atrial fibrillation/flutter, mechanical heart valve, moderate-to-severe valvular heart disease, conduction abnormality or paced rhythm were excluded.
AHF was defined as rapid onset or worsening of signs and/or symptoms of HF and one of the following criteria was required: (i) pulmonary congestion or (ii) objective findings of LV systolic dysfunction or diastolic dysfunction, or structural heart disease. Pulmonary congestion was defined as ‘congestion’ on a chest X-ray and/or as rales on physical examination.
IHD was defined as an underlying cause of AHF when patients presented as acute coronary syndrome or had a past medical history of IHD, which was confirmed by coronary angiography.
Clinical events related to HF were defined as re-admission due to HF exacerbation or all-cause death. Study protocol was approved by the Institutional Review Board of Jeju National University Hospital. Written informed consents were waived because this study was the retrospective review of the medical records.
Echocardiographic study
Echocardiographic studies were performed using SONOS 7500 (Philips Healthcare, Palo Alto, CA, USA), VIVID 7 (GE Medical, Milwaukee, WI, USA) or ACUSON SC2000 (Siemens Medical, Mountain View, CA, USA).
From the M-mode tracings of the LV and left atrium (LA), LV end-diastolic and end-systolic dimensions and LA dimension at mid-systole were measured. LA volume was measured using biplane method of disc or calculated using an ellipsoid model of three linear measurements. LV volume in diastole and systole were measured at the apical 4- and 2-chamber view using modified Simpson's method, and left ventricular ejection fraction (LV EF) was calculated. When endocardial border was not clear at the apical window, LV EF was calculated using LV end-diastole and end-systolic dimensions and the apical wall motion as recommended in the previous study.10)
Standard diastolic filling parameters such as peak early-diastolic (E wave) and peak late-diastolic (A wave) transmitral flow velocity, deceleration time (DT) of E wave, E/A ratio, early-diastolic (E′ wave) and late-diastolic (A′ wave) septal mitral annular velocity and E/E′ ratio were measured at the apical 4-chamber view using pulsed and tissue Doppler echocardiography. Means of parameters at least three beats were used in the data analysis.
Diastolic dysfunction of LV was graded as ≥ 2 (group 1) or 1 (group 2) according to usual algorithm using E/A ratio, DT of mitral inflow, E′/A′ ratio, and LA size according to 2016 guideline of American Society of Echocardiography.11)
Statistical analysis
Data were expressed as mean ± standard deviation for continuous variables, and frequencies and percentages for categorical variables. If data showed skewed distribution, they were expressed as median (interquartile range). To compare between 2 groups, Student's t-test for continuous parameters with normal distribution, Mann-Whitney U test for those with skewed distribution, or chi-square test for categorical variables was used. Kaplan-Meier method with log-rank test was applied for 2-year event free survival analysis including death and re-admission due to congestive HF. Univariate and multivariate Cox proportional hazard models were used to analysis the prognostic factors for the 2-year mortality.
Statistical analyses were performed using SPSS version 20.0 for Windows (IBM, Markham, Canada) and a p-value of less than 0.05 was considered statistically significant.
RESULTS
Baseline clinical characteristics and laboratory findings of study subjects
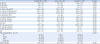
Mean age of all patients was 73.9 ± 11.3 years (77 men) and 58.0% of them were ≥ 75 years old. Mean age of patients in group 1 was significantly younger (69.8 ± 12.1 vs. 77.6 ± 9.1 years; p < 0.05) and systolic blood pressure was significantly lower in group 1 (134.3 ± 28.5 vs. 147.6 ± 32.7 mmHg; p < 0.05). Other clinical characteristics including body mass index, smoker, diastolic blood pressure and heart rate were not significantly different (Table 1). Also, co-morbid conditions including hypertension, angina, diabetes mellitus, CKD and stroke were not significantly different between the 2 groups.
Table 1
Baseline clinical characteristics and laboratory findings of study subjects

Data were expressed as mean ± standard deviation, median (interquartile range), or number (%).
Group 1: diastolic dysfunction, grade ≥ 2, Group 2: diastolic dysfunction, grade 1.
BMI: body mass index, BUN: blood urea nitrogen, CKD: chronic kidney disease, CKMB: creatinine kinase MB isoenzyme, DBP: diastolic blood pressure, eGFR: estimated glomerular filtration rate by Modification of Diet in Renal Disease (MDRD) equation, Hb: hemoglobin, hs-CRP: high sensitivity C-reactive protein, NT-proBNP: N-terminal pro-B-type natriuretic peptide, SBP: systolic blood pressure, TnT: troponin T.
![]()
Baseline laboratory findings including hemoglobin, kidney function presented as estimated glomerular filtration rate (eGFR) by Modification of Diet in Renal Disease equation, N-terminal pro-B-type natriuretic peptide (NT-proBNP), creatinine kinase MB isoenzyme (CKMB) and troponin T (TnT) were not significantly different (Table 1).
Echocardiographic findings of study subjects
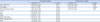
LV EF was significantly lower in group 1 (37.4% ± 12.1% vs. 45.9% ± 15.9%; p < 0.05). LV internal dimension and LV volume in diastole and systole were greater in group 1 (Table 2). Patients in group 1 have more mitral regurgitation of mild-to-moderate and higher systolic pressure of the right ventricle.
Table 2
Echocardiographic findings of study subjects
Data were expressed as mean ± standard deviation.
Group 1: diastolic dysfunction, grade ≥ 2, Group 2: diastolic dysfunction, grade 1.
A: peak late-diastolic transmitral flow, A′: peak late-diastolic mitral septal annular wave, DT: deceleration time, E: peak early-diastolic transmitral flow, E/A ratio: ratio of peak early- to late-diastolic transmitral flow velocity, E/E′: ratio of peak early mitral inflow velocity to peak early septal mitral annular velocity, E′: peak early-diastolic septal mitral annular wave, LA: left atrium, LV EF: left ventricular ejection fraction, LVIDd: left ventricular end-diastolic internal dimension, LVIDs: left ventricular end-systolic internal dimension, RVSP: right ventricular systolic pressure.
![]()
Among the parameters related to the diastolic dysfunction, E velocity, E/A ratio and E/E′ ratio wave were significantly higher in group 1 than group 2 (104.1 ± 22.9 vs. 63.0 ± 23.6 cm/sec; 2.1 ± 1.2 vs. 0.7 ± 0.2; and 27.2 ± 10.1 vs. 16.4 ± 5.4, respectively; p < 0.05). A velocity, DT of E wave and A′ velocity were significantly lower in group 1 (59.8 ± 25.2 vs. 96.0 ± 27.3 cm/sec; 163.4 ± 73.8 vs. 230.3 ± 76.6 msec; 5.5 ± 2.4 vs. 7.4 ± 2.1 cm/sec, respectively; p < 0.05). E′ velocity was not significantly different.
Prediction of independent variables for outcomes
Among 138 enrolled patients, 38 patients (27%) were lost to follow up during 2 years. There were 27 deaths, 39 re-admissions due to congestive HF, and 50 clinical events.
Patients with group 1 showed higher 2-year mortality rate than those with group 2 (36.2% ± 6.7% vs. 13.6% ± 4.5%; p < 0.05). However, re-admission due to congestive HF (34.0% ± 6.6% vs. 35.1% ± 6.2%) or clinical event rate (49.1% ± 6.9% vs. 38.9% ± 6.5%) was not significantly different between groups (Figure 1).
 | Figure 1Kaplan-Meier 2-year survival curves for the pseudonormal (PN) or restrictive filling pattern (RFP) of left ventricle (LV) and LV ejection fraction.
|
Two-year mortality rate of patients with LV EF ≥ 50% was lower (13.7% ± 7.4%) compared with patients < 40% (26.8% ± 6.0%) or with LV EF 40%–49% (28.0% ± 8.0%), but without statistical significance (p = 0.442) (Figure 1). Also, re-admission due to congestive HF (37.5% ± 6.5%, 34.0% ± 8.4%, and 28.3% ± 9.9%, respectively) or clinical event rate (49.2% ± 6.7%, 39.4% ± 8.6%, and 36.6% ± 10.4%, respectively) was not significantly different according to LV EF < 40%, 40–49%, and ≥ 50%. In addition, when patients were divided into 2 groups as LV EF less than 50% and 50% or more, there was also no statistically significant difference in 2-year mortality rate, re-admission due to congestive HF or clinical event rate between groups (data not shown). Patients were further divided into six groups according to the presence or absence of PN or RFP and LV EF (PN or RFP of LV with LV EF ≥ 50%, 40–49%, or < 40%, and no PN or RFP with LV EF ≥ 50%, 40–49% or < 40%), but 2-year mortality rate was not significantly different among groups (data not shown). In addition, even when patients divided into four groups (PN or RFP of LV with LV EF ≥ 50% or < 50%, and no PN or RFP with LV EF ≥ 50% or < 50%), there was also no significant difference in 2-year mortality among groups (data not shown).
Univariate Cox proportional hazard analysis for 2-year mortality showed that PN or RFP of LV, higher stage of CKD and higher New York Heart Association (NYHA) functional class were poor prognostic factors, but neither LV EF nor older age ≥ 75 years predicted 2-year mortality. On multivariate analysis, PN or RFP of LV (hazard ratio [HR], 2.52; 95% confidence interval [CI], 1.09–5.84; p = 0.031), higher stage of CKD (HR, 1.57; 95% CI, 1.14–2.17; p = 0.006) and higher NYHA functional class (HR, 1.81; 95% CI, 1.11–2.94; p = 0.017) were still significant prognostic factors for 2-year mortality (Table 3).
Table 3
Cox proportional hazards analysis for predictors of 2-year mortality
CI: confidence interval, CKD: chronic kidney disease, EF: ejection fraction, HR: hazard ratio, LV: left ventricle, NYHA: New York Heart Association, PN: pseudonormal, RFP: restrictive filling pattern, RVSP: right ventricular systolic pressure.
![]()
DISCUSSION
This study investigated whether the diastolic dysfunction of LV was associated with major cardiac events, including death and re-admission due to congestive HF in patients with IHD presenting as AHF, and showed that PN or RFP of LV was an independent predictor of death at 2-year and a more useful than LV EF.
Echocardiographic evaluation at the time of admission in patients with IHD is considered to be a simple, non-invasive test to assess the extent of myocardial damage, LV systolic and diastolic function, mechanical complications, and prognosis.12)13) Echocardiographic parameters such as LV EF, E/A ratio, DT, or E/E′ ratio are usually used to evaluate LV systolic or diastolic dysfunction in patients with AHF.
The development of early or late HF after AMI, which is the natural consequence of significant myocardial damage, is related to a poor prognosis.14) One meta-analysis reported a mean incidence of in-hospital HF of 36% in patients with AMI.15) Early development of HF portended higher in-hospital and one-year mortality.16) About 6% of patients with AMI without previous HF developed late-onset (≥ 3 months after the attack) HF, which was found to be associated with a 10-fold increase in 5-year mortality.17) In addition, patients with HF after AMI are also at high risk of future HF re-admissions.18)19)
LV systolic dysfunction after AMI has been recognized as an important marker of outcome and may be sustained or progressively aggravated by the process of ventricular remodeling, which is related to the risk of HF and death.20)21) LV systolic function has been anticipated as an independent predictor of death after AMI, and the severity of LV systolic function was associated with an almost exponential relationship with survival.22) However, in this study, LV EF was not related to 2-year mortality when Kaplan-Meier analysis or Cox proportional hazard analysis was performed.
Diastolic dysfunction of LV is also known to be associated with clinical outcome after AMI. Many patients who develop PN or RFP of LV after AMI may already have diastolic dysfunction resulting from intrinsic abnormal myocardial function and vascular dysfunction.23) The greater the size of the infarcted myocardium, the more stiffness increases with the appearance of restrictive disorder. In patients with AMI, mortality incrementally increased according to the grade of diastolic dysfunction. The patients with PN or RFP of LV, at four-year follow-up, had almost half the chance of survival compared to the patients with normal diastolic function.24)
A recent study showed that progression of LV diastolic dysfunction in outpatients with preserved LV systolic function was a strong and independent predictor of all-cause death.25) Obviously, when PN or RFP of LV was present after AMI, the mortality rate increased regardless of LV EF23) and an odds ratio of 10 for developing future HF was observed.7) In this study, 2-year mortality was significantly higher in patients with PN or RFP of LV, and PN or RFP of LV was an independent predictor of 2-year mortality.
The previous studies also demonstrated that PN or RFP of LV was a strong predictor of future HF after AMI, and higher mortality in patients with existing HF.26) PN or RFP of LV was associated with higher LA pressure,27) higher NYHA functional class,28) and higher neurohormone concentration, which are associated with prognosis after acute coronary syndromes.29)
The present study has limitations. This study was a single center study, only a small number of patients were enrolled, and patients' data were retrospectively collected. In some cases, LV volume was not obtained because of poor echocardiographic image. If more patients were enrolled, patients with preserved LV EF may have better prognosis. Different baseline characteristics may affect the results, despite of multivariate Cox proportional analysis. Patients who died before echocardiographic study were not included in this analysis. Because cause-specific mortality data were not available in all died patients, only all-cause mortality was reported. However, despite of these limitations, we thought that this study showed meaningful data, because most previous studies have been conducted on patients who were somewhat different in clinical characteristics compared with Korean patients, and clinical evaluation of the impact of diastolic function on mortality in patients with IHD and AHF has been relatively rare in Korea.
In conclusion, PN or RFP of LV was a more useful prognostic factor for long-term mortality than LV EF in patients with IHD presenting as AHF.
 XML Download
XML Download