

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy, accounting for >90% of all endocrine cancers (1). With the development of new diagnostic techniques, the worldwide incidence of thyroid carcinoma has progressively increased in recent decades (2). Although PTC has a favorable prognosis overall, with an average 10-year survival rate of over 90%, it is frequently recurrent and metastasizes to regional lymph nodes (LNs) (3). Indeed, up to 35% of patients suffer from disease recurrence during long-term follow-up, and over 35,000 patients worldwide die due to thyroid cancer each year (4).
In general, PTC prognosis depends on several clinicopathological factors, including age, sex, histological subtype, tumor size, LN metastasis, extrathyroidal extension (ETE) and distant metastasis (5). Recent studies have demonstrated that certain genetic events may also carry diagnostic, prognostic and therapeutic value in the management of PTC. Furthermore, the precise identification of these genetic events may help to decrease the recurrence of thyroid carcinoma. BRAF mutation is the one of the most representative genetic alterations, and several studies have shown that BRAF mutation indicates a poor prognosis and is associated with advanced PTC (67). In fact, an ongoing phase I study is currently investigating inhibition of BRAF mutation in an effort to identify its therapeutic potential (8).
Receptor tyrosine kinases are transmembrane proteins that are involved in various cellular functions, such as cell growth, differentiation, and survival. Among these receptors, epidermal growth factor receptor (EGFR) and human EGFR 2 (HER2) are monomeric cell-surface receptors that are part of the ErbB family of receptor tyrosine kinases. Mutations leading to EGFR overexpression have been shown to be associated with a variety of malignancies, including head and neck, esophageal, ovarian, cervical, lung and bladder cancers (9). EGFR expression has also been found to be a significant independent prognostic factor for thyroid cancer (10).
HER2 overexpression has been shown to be a potential marker of aggressive biological behavior in a variety of tumors, such as breast cancer and gastric cancer. However, the role of HER2 in PTC remains unclear. Several groups have reported HER2 expression in thyroid cancer, but the results of their studies were inconclusive (11121314).
The present retrospective study compared the expression of EGFR and HER2 in PTC using immunohistochemistry and analyzed the association between the expression of these proteins and the clinicopathological features of PTC at a single institution.
METHODS
1. Patient selection
This retrospective study analyzed surgical specimens from consecutive patients with PTC who were treated at Uijeongbu St. Mary's Hospital from October 2013 to February 2015. Majority of patients performed underwent thyroid surgery plus prophylactic central LN dissection. We selectively performed modified radical neck dissection if the preoperative imaging studies (ultrasound and computed tomography) raised suspicious of malignancy and if the fine needle aspiration cytology were found to contain atypical cells or metastatic papillary carcinomas. In total, 129 patients with sufficient tissue for immunohistochemical and molecular marker evaluation were included in this study. Written informed consent was obtained from all patients and their families. This study was reviewed and approved by the institutional review board of Uijeongbu St. Mary's Hospital (UC15RISI0101).
Clinical information was retrieved retrospectively from the patients' medical records and pathology reports. The histological diagnosis was confirmed by experienced pathologists after hematoxylin and eosin staining of tissue sections.
Distant metastasis, patient age, completeness of resection, local invasion, and tumor size (MACIS) scores were considered to predict mortality for PTC (15). These scores were calculated using following formula:
MACIS score=3.1 (if aged ≤39 years) or 0.08×(if aged ≥40 years)+0.3×tumor size (cm), +1 (if not completely resected), +1 (if locally invasive), +3 (if distant metastases were found)
2. Immunohistochemistry
All specimens were sliced into consecutive 4-µm sections, stained with hematoxylin and eosin and examined blindly by two independent pathologists with experience in thyroid pathology. All specimens were classified according to previously published diagnostic criteria for thyroid tumors (16).
The 4-μm sections of paraffin blocks were immunohistochemically stained. Briefly, the paraffin sections were deparaffinized in xylene and rehydrated in serial-graded ethanol, and endogenous peroxidase activity was blocked with 3% hydrogen peroxide in methanol. Antigens were retrieved by boiling the slide-mounted sections in citrate buffer (0.01 mol/L, pH 6.0) in a pressure cooker at 125°C for 15 minutes. The sections were then incubated with the primary antibodies mouse monoclonal anti-EGFR (DAKO Corporation, Carpinteria, CA, USA) (diluted 1:100) and prediluted rabbit monoclonal anti-HER2/neu (rocheDAKO Corporation, Glostrup, Denmark) for 32 minutes at room temperature, after which the sections were counterstained with Mayer's hematoxylin, dehydrated, cleared and mounted.
A modified version of a semi-quantitative scoring system that had been described in previous studies was applied. The percentage of positive tumor cells (PP) was scored as follows: 0, no tumor cells stained; 1, 1%–5% of cells stained; 2, 6%–20% of cells stained; 3, 21%–50% of cells stained; and 4, >50% of cells stained. In addition, the intensity was scored as follows: 0, no staining; 1, weak staining; 2, moderate staining; and 3, strong staining. The immunoreactive score (IRS) was calculated by multiplying the percentage of positive cells by the staining intensity, and tumors with an IRS ≥1 were considered as positive for EGFR expression (17). The degree of HER2 staining was scored as 0, 1, 2 or 3 by two pathologists according to breast cancer criteria because no criteria for PTC have been established. The staining of the samples was interpreted on a standard scale (0 to 3+): 0, no staining in tumor cells; 1+, weak and incomplete membrane staining or complete but weak staining in <10% of tumor cells; 2+, weak complete membrane staining in at least 10% of cells or intense complete membrane staining in <30% of tumor cells; and 3+, uniform intense circumferential staining in >30% of tumor cells (18).
3. Statistical analysis
Data analyses were performed using MedCalc for Windows, version 13.3 (MedCalc Software, Ostend, Belgium). The χ2 test and Fisher's exact test were used to analyze categorical variables, and independent-sample Student's t-test was used to analyze continuous variables. Continuous variables are presented as the mean±standard deviation. Differences were considered statistically significant when P<0.05.
RESULTS
The clinicopathological characteristics of the 129 patients (104 females [80.6%] and 25 males [19.4%], mean age of 46.26±11.89 years at the time of surgery) are summarized in Table 1. ETE and LN metastases were present in 49 (38%) and 48 (37.2%) patients, respectively. Total thyroidectomy (or near-total thyroidectomy) was performed in 91 (70.5%) patients. Additionally, the mean number of retrieved LNs was 7.03±5.99, and the mean tumor size was 1.08±0.75 cm.
Table 1
Clinicopathological characteristics of the study population (n=129)
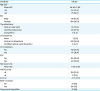
Values are presented as mean±SD or number (%).
SD = standard deviation; LN = lymph node; ETE = extrathyroidal extension; MACIS = distant metastasis, patient age, completeness of resection, local invasion, and tumor size; LI = labeling index.
![]()
Table 2 shows the association between EGFR expression and the clinicopathological characteristics of the patients. EGFR expression was observed in 111 of the 129 (86.0%) patients with PTC. Although positive expression of EGFR was not significantly associated with age, size, ETE, or LN metastasis, the Ki-67 labeling index (LI) was significantly higher in the presence of EGFR expression than in the absence of expression (4.49±6.36 vs. 2.00±2.13, P=0.002).
Table 2
Univariate analysis of the associations between clinicopathological characteristics and EGFR expression
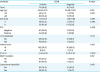
Values are presented as mean±standard deviation or number (%).
EGFR = epidermal growth factor receptor; LN = lymph node; ETE = extrathyroidal extension; MACIS = distant metastasis, patient age, completeness of resection, local invasion, and tumor size; LI = labeling index.
![]()
HER2 expression was significantly associated with younger age and cervical LN metastasis. The Ki-67 LI tended to be higher in the presence of HER2 expression, although this association was not statistically significant (Table 3).
Table 3
Univariate analysis of the associations between HER2 expression and clinicopathological characteristics in 129 patients with PTC
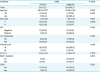
Values are presented as mean±standard deviation or number (%).
HER2 = human epidermal growth factor receptor 2; PTC = papillary thyroid carcinoma; LN = lymph node; ETE = extrathyroidal extension; MACIS = distant metastasis, patient age, completeness of resection, local invasion, and tumor size; LI = labeling index.
![]()
Also, positive expression of EGFR and HER2 were not significantly associated with higher MACIS scores.
DISCUSSION
EGFR is a receptor tyrosine kinase that is important for the transduction of extracellular signals from the surface to the interior of a cell to mediate cell proliferation and apoptosis (19). EGFR is frequently overexpressed in malignant tumors, including breast and bladder cancers (20). Little is known about the value of EGFR expression for the prediction of PTC prognosis. In recent years, several studies have reported the relationship between EGFR expression and prognosis of PTC. These studies suggested that increased expression of EGFR is associated with poor prognosis of PTC. Fisher et al. (10) demonstrated that EGFR is correlated with advanced stage, ETE, LN metastasis, and BRAF(V600E) mutations in univariate analysis. The authors concluded that EGFR could be an important biomarker for aggressive PTC. Tang et al. (21) investigated EGFR expression in PTC, nodular hyperplasia, and normal thyroid tissue specimen using immunohistochemistry. They found that EGFR expression levels were up-regulated in PTC and were associated with LN metastasis. On the contrary, our data did not show the positive results associated with aggressive features of PTC. These differences may be caused by small sample size. Interestingly, the mean Ki-67 LI was higher than the EGFR expression. The expression of Ki-67 is generally evaluated immunohistochemically as an LI, and a high Ki-67 LI has been shown to be associated with a poor outcome in patients with breast or prostate cancer (22). Although many published studies have indicated the value of the Ki-67 LI in PTC, no studies in the literature have investigated the association of Ki-67 and EGFR expression in PTC. The Ki-67 LI was found to be higher in EGFR expression cases in some studies investigating the correlation of Ki-67 and EGFR in other carcinomas (2324). However, certain studies have shown that Ki-67 LI is correlated with ETE, tumor size, and prognosis (252627).
HER2 is a proto-oncogene that has an important role in the development and progression of human cancers, and especially breast cancer. Overexpression of the HER2 protein and amplification of the HER2 gene have been recognized as prognostic factors in breast cancer in particular (28). Additionally, HER2 overexpression in gastric cancer is associated with a poor prognosis and more advanced disease (29). Therefore, anti-HER2 therapy, such as trastuzumab, has been applied in breast and gastric cancer patients with HER2 overexpression. However, no study has thoroughly investigated HER2 expression in thyroid carcinoma. In the present study, HER2 was highly expressed in younger patients (40.55±13.77 vs. 47.30±11.26) and in patients with cervical LN metastases (60% vs. 33.0%), and these associations were statistically significant. There are some considerations in analysis of these results. Age is the most important prognostic factor for patients with well-differentiated thyroid cancer. Younger age (<45 years) is associated with good prognosis. Thus, these results contradict an existing theory. Although, HER2 expression is associated with LN metastases in this study, it is difficult to decide that HER2 is an important marker for PTC as mentioned earlier. The Ki-67 LI was higher in the presence of HER2 expression, but this association was not statistically significant.
Our study has certain limitations. First, a small sample size was used to identify the value of EGFR/HER2 expression in PTC because of the short study period. Second, we described the degree of HER2 staining according to criteria for breast cancer, as there are no established criteria for this parameter in thyroid cancer. Enrollment of additional patients and establishment of criteria for determining the degree of HER2 staining in thyroid carcinoma are therefore necessary. Third, there is no follow-up of the patients. Patients with papillary thyroid cancer rarely die of their disease, and this study is designed and performed recently.
In conclusion, our study showed that HER2 expression was associated with younger age and cervical LN metastasis. Additionally, the Ki-67 LI was higher in the presence of EGFR expression. The immunohistochemistry of EGFR and HER2 has limited value in PTC. A long-term follow-up study will be necessary to identify the clinical value of EGFR/HER2 expression in PTC.
 XML Download
XML Download