

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Isolated H-type tracheoesophageal fistula (TEF) is a rare malformation of the airways representing the subtype without esophageal atresia, comprising 4% to 5% [1234]. Moreover, double H-type TEF is an extremely rare anomaly [1]. It is not included in Gross classification because of its scarcity, and a very few number of patients had been reported in the literature. The first case report in the English literature was published in 1957 but one case was revealed previously in a series of 103 TEF patients published in 1952, identified in postmortem examination [25]. The first successful surgical repair was done via a right posterolateral thoracotomy followed by the left cervical approach, reported in 2009 [2].
In Korea, 9 cases of H-type TEF were reported in a series of 130 cases [6] but double H-type TEF had never been reported. This is the first case with double H-type fistulae in a Korean newborn who has been operated first with a preoperative diagnosis of a single H-type fistula and then with another H-type fistula which was located above the level of the first lesion.
CASE REPORT
A male full-term neonate presented to emergency room with cyanosis after breastfeeding. The patient was delivered by planned caesarian section 12 hours before arrival. Chest radiograph taken on the first day of life was cleaned but the radiograph taken on the third day of life suggested aspiration pneumonitis (Fig. 1). Upper gastrointestinal (GI) series showed gastroesophageal regurgitation with pulmonary aspiration but esophagoscopy and video esophagogram on the eleventh day of life showed no abnormality. Contrast esophagogram was followed on the 33rd day of life, and an H-type TEF was found at 1 cm above the carina, at T4 level (Fig. 2). Surgical repair was performed on the 37th day of life through a right posterolateral thoracotomy incision. The fistula was positively identified, divided, and closed with non-absorbable interrupted sutures during the operation.
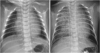 | Fig. 1Two days after birth (right), chest radiograph shows aspiration pneumonitis which was absent on the date of birth (left).
|

Routine esophagogram taken on postoperative day 10 still showed an evidence of fistula (Fig. 3). Recurrence or presence of another H-type fistula had been suspected. To confirm the diagnosis, rigid bronchoscopy was scheduled under general anesthesia on postoperative day 15. However, the bronchoscopy failed to demonstrate the opening of the fistulous tract even under positive ventilation.

When feeding was started assuming that the esophagogram showed contrast aspiration, cyanosis and pneumonitis recurred, only less severely than the preoperative days. The baby was treated with antibiotics and kept being fed per oral. He suffered from recurrent pneumonitis.
Two months later, on the 124th day of life, the baby underwent esophagogram to reassure the existence and location of the second H-type fistula. Identifying the fistula at T2 level, a second operation was scheduled on the 146th day of life. A rigid bronchoscopy was performed to confirm the second H-type fistula just before the operation. Fistula opening was finally visible at 2 cm above the previously repaired site, and a Fogarty catheter was inserted through the opening (Fig. 4). The lesion was accessed through right cervical incision, and the fistula was located just below the clavicular level. The second fistula was divided and closed with non-absorbable fine sutures. The baby was fed via orogastric tube for two weeks, and oral feeding was tried. The baby was discharged on postoperative day 27 due to transient recurrent laryngeal nerve palsy. He suffered from vocal cord palsy and hypopharyngeal motility disorder but symptoms alleviated gradually and disappeared when the baby was one year old.

DISCUSSION
Double H-type TEF is an extremely rare variant of congenital esophageal fistula which is a double existence of H-type fistula, equivalent to E-type in Gross classification. This anomaly was first reported by Hübner in a German article in 1943 [2], and very few cases have been reported so far [125]. The first reported case in English literature by Babbitt was a neonate who was succumbed to death after the completion of second operation with preoperative diagnosis of single H-type fistula. Respiratory difficulty was developed in postoperative period, and double H-type fistula was revealed in postmortem examination [2]. Schulte et al. [2] performed surgery on the patient with H-type fistula through a thoracotomy incision but respiratory symptom developed on the second postoperative day, and the other H-type fistula was found by rigid bronchoscopy. They approached the fistula through a cervical incision, and the second operation was successfully finished. It was the first successful surgery with patient survival on double H-type fistulae. Mattei [1] reported a case with double H-type fistulae successfully operated in a single surgery with preoperative diagnosis of double H-type fistulae. As seen in the literature, it seemed to be difficult to diagnose at once, preoperatively.
Because of the configuration of the fistula and the absence of esophageal atresia, the diagnosis of an H-type fistula may be delayed [7]. Difficulty in diagnosing double H-type TEF in the literature might be due to extremely low incidence and difficulty in visualization of fistulae in a single diagnostic study. To make a correct diagnosis, starting with a high index of suspicion is necessary because symptoms are almost the same as in single H-type fistula.
In the literature, the same pattern of symptoms appeared as they did in single H-type fistula. Helmsworth and Pryles [8] described a triad of symptoms of H-type fistula, including 1) paroxysm of coughing precipitated by feeding; 2) gaseous distention of the GI tract; 3) pneumonitis. Particularly, if preoperative symptoms persist after surgery, another possible H-type fistula must be suspected, in addition to the possibility of recurrence.
For a correct diagnosis, it is necessary to understand the anatomy and location of the fistula. Andrassy et al. [9] described that 70% of 23 TEF were within 2 cm above or below the sternal notch, while 17% were more than 2 cm above, and 13% were more than 2 cm below the sternal notch. His clinical studies showed that TEF exists over a wide range, and this range must be included in any examination in esophageal atresia anomalies. The direction of H-type fistula is running a little bit downward to esophagus, so ‘N-type’ rather than ‘H-type’ is more relevant [10].
Diagnostic methods in suspected H-type fistulae are upper GI series, esophagogram, esophagoscopy, and bronchoscopy. It is recommended that initial investigations in esophagogram should be proceeded with water-soluble contrast with low osmolarity. However, there was an approximately 50% chance of diagnostic miss in routine esophageal contrast swallow study, thus tube video esophagography is recommended [11]. Rigid bronchoscopy is a useful adjunct for repair of the H-type TEF because it allows confirmation of the level of the fistula, helping the surgeon decide which is the best approach [2]. Bronchoscopy with esophagoscopy should be performed in the operating room just before the surgery. Catheterization of the TEF with Fogarty catheter or guidewire is suggested by several authors [312]. It is plausible that every diagnostic test is necessary and complimentary to make a correct diagnosis.
Diagnostic methods used in our patient were esophagogram, upper GI series, video esophagography, and bronchoscopy. The first lesion could be confirmed in esophagogram only. Also, the second fistula was confirmed in esophagogram only, yet not in diagnostic bronchoscopy. The contrast material used in esophagogram was diluted barium. For ligation of the second fistula, bronchoscopy was done just before surgery for identification of fistula and cannulation.
Surgery can be accessed through neck or chest according to the anatomic location of the fistulae. In this patient, it was helpful to insert a Fogarty catheter under rigid bronchoscopy prior to surgery to find the fistula easily during surgery. We approached the second lesion through a right cervical incision, and the division was done successfully.
 XML Download
XML Download