

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Surgery in neonates had been earlier associated with high mortality and postoperative complications. However, due to continuous improvement in postoperative management, survival rates in neonates have significantly improved [12]. One of the important factors to be considered in the postoperative management of neonates is their nutrition. Therefore, active nutritional support, such as the beginning of early oral nutrition and the supply of sufficient protein, is recommended in many journals and by nutrition societies for pediatric patients [34]. However, most of the recommendations on postoperative nutritional support have been made for children and adults, and studies on the effect of nutritional support after surgery, especially abdominal surgery, in neonates, are rarely conducted.
There are few reports on delayed postoperative growth in neonates [567]. In a study that examined the postoperative growth in infants with congenital heart disease or necrotizing enterocolitis, growth-related factors such as weight, height, and head circumference were reported to be significantly lower than those in normal infants [67]. In addition, the delay in growth is closely related to the course of surgery, including the type of surgery and its associated complications; thus, postoperative growth in neonates is a major factor that can predict their postoperative outcome and survival [8].
In this study, we aimed to evaluate the relationship between nutritional support and growth velocity after abdominal surgery in neonates.
METHODS
1. Patient selection
This study was retrospectively conducted at a single center. A total of 113 neonates who underwent abdominal surgery in neonatal intensive care unit (NICU) from January 1, 2012 to December 31, 2016 were enrolled in this study. All neonates who underwent abdominal surgery were candidates of this study. We excluded 57 neonates who had undergone enterostomy closure operation and diagnostic laparotomy, 6 who died in hospital or after discharge, and 5 with incomplete medical records. Finally, 45 neonates were included in the study. The need for obtaining patients' informed consent was waived off due to the retrospective nature of the study.
2. Data collection
Clinical data on surgery and postoperative recovery period of the neonates were retrospectively collected from their electronic medical records.
1) Patients-related factors
Gestational age, birth weight, sex, Apgar score at birth (1-minute to 5-minute), accompanying malformations, and length of hospital stay, were recorded for all infants. The maternal factors were not considered.
2) Nutritional factors
Information on the oral and parenteral nutrition (PN) provided on postoperative days (PODs) 1, 3, 5, 7, and 9 was examined. For oral nutrition, whole milk (67 kcal per 100 mL containing 7.3 g carbohydrates, 1.5 g proteins, and 3.5 g lipids) and breast milk (68 kcal per 100 mL containing 7.2 g carbohydrates, 1.0 g proteins, and 3.9 g lipids) were administered. In premature infants, 14% premature milk (70 kcal per 100 mL containing 7.4 g carbohydrates, 2.1 g proteins, and 3.6 g lipids), and Neocate (Nutricia, Strombeek-Bever, Belgium; 71 kcal per 100 mL containing 8.0 g carbohydrates, 2,0 g proteins, and 3.5 g lipids) were administered. PN was administered by combining carbohydrates/proteins/lipids with dextrose water (Dextrose water's concentration was changeably used every day the range of 6%–10%; we calculated the total amount of glucose in the dextrose water administered for 24 hours), Primene 10% (Baxter, Clintec Benelux NV, Brussels, Belgium), and Smoflipid 20% (Fresenius Kabi, Bad Homburg, Germany).
A full feeding was defined as the completion of target calorie of premature neonates (150 kcal/kg/day) [9]. We examined if and when a full feeding was obtained in the neonates. Fasting for more than 24 hours during the course of diet advance from nothing per oral to milk feeding was recorded, and the dietary progress was recalculated based on the time when diet was resumed after fasting. The target calorie intake after surgery was 60 kcal/kg/day in the immediate postoperative period, and the total target protein intake was 3 g/kg/day [10].
3) Growth-related factors
We found the record about body weights of neonates before surgery and on PODs 1, 3, 5, 7, and 9, body weights at discharge, and heights and body weights at 1 year after birth. When heights and body weights of outpatients could not be collected at 1 year after birth, these were estimated as close as possible to the values at 1 year after birth.
Growth velocity was calculated as:
where Wn=weight at discharge, W1=weight just before surgery, and Dn–D1=days of hospitalization after surgery. We used body weights at the time of surgery and at discharge [11].
Expected growth velocity was calculated based on World Health Organization growth chart, the mean body weight (Z=0) based on the age at discharge (calculated by age on weeks, corrected age for prematurity) was calculated.
Additionally, at 1 year after birth, Z scores were calculated using the World Health Organization growth charts based on the neonates' heights and weights at 1 year of postnatal age to determine the growth rates in premature infants with less than 37 weeks of gestational age and to compare these with the growth rates in normal infants of the same age.
4) Operative factors
The operative data collected included the time of operation, type of operation, and presence of bowel resection. Surgical complications were defined as all events associated with surgery (including wound infections and widening, intestinal adhesions, and perforations). Body weight and growth velocity were calculated based on the last surgery when reoperation was performed for any reason, except enterostomy closure surgery.
4. Statistical analysis
Statistical analysis was performed to evaluate the relationship between nutritional support and growth velocity after abdominal surgery in neonates. We used SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). Patient-related, nutritional, growth-related, and operative factors were assessed with Student's t-test. The Mann-Whitney U test was used to evaluate the relationship between the operative factors, nutritional factors, and growth-related factors. The p<0.05 was considered statistically significant.
RESULTS
1. Patient-related factors
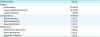
The mean gestational age of 45 neonates who underwent abdominal surgery in NICU was 34.4 weeks; 42.2% of them were premature neonates, of which 17.8% were born before 28 weeks of gestational age. The mean birth weight was 2.4 kg, and 88.9% of the neonates had appropriate weight for gestational age. The most common anomaly (in 24.44% of the infants) was patent ductus arteriosus (PDA), and 4 of them with large PDA underwent PDA clipping in NICU. The mean length of hospital stay after abdominal surgery was 42.53 days (Table 1).
Table 1
Patients-related data (n=45)

Values are presented as number of patients (%) or meam±standard deviation.
LBW, low birth weight; VLBW, very-low birth weight; ELBW, extremely-low birth weight; SGA, small for gestational age; AGA, appropriate for gestational age
a)Gestational age was divided into 2 groups: preterm (≥28 and <37 weeks) and extremely preterm (<28 weeks); b)Birth weight was divided into 3 groups by a SI units; LBW (<2.5 kg at birth), VLBW (<1.5 kg at birth), and ELBW (<1.0 kg at birth); c)Birth weight was divided into 2 groups by the Z score; SGA (Z≤−2) and AGA (−2<Z≤2); d)Spina bifida, ventricular septal defect.
![]()
2. Growth velocity
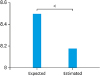
The average body weight at discharge was 3.26 kg. At 1 year after birth, there was no growth delay (as reflected in the Z score of less than −2) in 45 patients (Fig. 1). Based on the day of discharge, the expected growth velocity from the day of surgery was 8.50; however, the estimated growth velocity was 8.18, with a statistically significant decrease in the growth velocity (p<0.01; Fig. 2).

3. Operative factors
Most common cause for abdominal surgery was perforated necrotizing enterocolitis (22.2%). The next most was small bowel atresia (20%), and midgut volvulus (15.6%). In 26 (57.8%) patients, intestinal resection was performed, and mean length of bowel was 11.9 cm. Surgical complications were seen in 18 (40%) neonates, and reoperation was performed in 7 (38.9%) of them (Table 2).
Table 2
Operative data
Values are presented as number of patients (%). All p values were more than 0.05, considered not significant.
![]()
Based on the Mann-Whitney U test to determine the association between operative factors and growth velocity, there was no significant difference between the two groups in the absence of intestinal resection, surgical complications, and reoperation (Fig. 3).

4. Nutritional factors
The mean duration of PN use was 23.58 days. Ten (22.2%) neonates were administered bolus feeding without continuous feeding, and continuous feeding was started at average 4.29 days postoperatively. Bolus feeding was started at average 14 days postoperatively. The first stool was observed at average 3.42 days postoperatively, and 20 (44.4%) neonates experienced fasting for more than 24 hours during the dietary onset. The most frequent cause of fasting was stasis in 11 (24.4%) neonates and small bowel obstruction in 4 (8.8%) neonates. Two of them required reoperation.
Ten (22.2%) neonates were administered more than the target calorie intake from POD 1, and 24 (53.3%) were administered the target calorie intake from POD 3. The protein intake over and above the target calorie intake was provided to 16 (35.6%) neonates on POD 1 and 25 (55.6%) neonates on POD 3.
Mann-Whitney U test was used to examine the relationship between nutritional factors and growth velocity. The growth velocity during hospitalization of the neonates who met the target protein intake on POD 1 and 3 were 15.21 and 4.31, respectively. There was a significant difference in the rate of weight gain in patients with and without target protein intake on POD 1 (p=0.004). In addition, there was a significant difference of the growth rate whether the neonates had succeed for full feeding (150 kcal/kg/day) and the need for fasting for more than 24 hours (p=0.041 and 0.017, respectively). There were no significant differences in the relationship among the target calorie intake, amount of target protein intake on POD 3, initiation of enteral nutrition on POD 3, and rate of weight gain (Table 3 and Fig. 4).
Table 3
Nutritional data
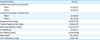
Values are presented as number of patients (%) or meam±standard deviation.
POD, postoperative day; PN, parenteral nutrition.
a)Fasting for more than 24 hours during the course of diet.
![]()

DISCUSSION
Nutritional support after surgery is considered necessary to reduce the postoperative complications and hospitalization period [3]. However, for neonates, the standardization of nutritional supply has not been well achieved due to their different physiological characteristics, nutritional requirements, and specificity of their condition due to various other comorbidities [3]. In addition, specific changes at the time of birth and coexisting anomalies of other organs, including the heart, make it more difficult to establish nutritional standards for neonates in NICU [1012].
Growth retardation has been commonly observed in many studies conducted in neonates who underwent surgery [67]. In this study, we evaluated the growth velocity and Z scores of neonates in the first year of life after hospital discharge. The growth velocity at discharge was significantly lower than the predicted growth velocity, but the Z score in the first year of life was above −2, indicating no delay in growth. This suggests that the method of providing nutritional support immediately after surgery was slightly different for each neonate, and it was possible to maintain continuous monitoring and appropriate nutritional support in all neonates.
The severity of surgery, complications, and reoperation also affect the postoperative growth in neonates [8] In particular, intestinal resection in the neonatal period has been reported to cause long-term growth retardation. Cole et al. [13] reported that infants with short bowel syndrome who had complications after surgery had significantly lower heights and head circumferences than the healthy infants. In this study, a better growth velocity was observed in the absence of intestinal resection, but it was not statistically significant. There was no significant difference in the growth rate between cases with reoperation and complications. This might have been due to a small sample size and short segment of small bowel resected with average of 11.9 cm in length which was not resulting short bowel syndrome, but it is likely that the decrease in growth was due to improper nutrition.
Our point of focus was the difference in growth velocity of neonates based on the nutritional methods. Many studies have reported that an early postnatal protein intake in premature and low birth weight infants is a predictor of growth, and it positively affects their neurological development [69].
In addition, the energy demand due to stress reaction increases postoperatively; so, it is also important to provide adequate calories [12]. We interested to know how energy and protein supplies affected the growth in neonates after surgery.
Although at the start of this study, infants had gradually increased their nutritional intake, subsequently, the neonates were administered the target protein requirement within the next day or within 3 days after surgery. They were provided active tube feeding. When the required calories were supplied from POD 1 or 3, the growth velocity did not increase rather decreased, and a statistically significant increase in growth velocity was observed in the protein-fed neonates due to protein activation. This suggests that a sufficient amount of protein rather than calories administered immediately after surgery may have a positive effect on the growth of neonates. Therefore, proper and sufficient nutrition after surgery, especially in the form of protein supply, should be considered. However, one study in the European Childhood Obesity Program reported that an adequate protein supply in premature neonates affects the rate of growth, which in turn increases the risk of subsequent obesity, and thus, adequate nutritional monitoring is an important concern [14].
This study has a few limitations. First, the sample size was small, and this retrospective study was conducted at a single institution. Second, all patients in this study were neonates who were operated on within 30 days of NICU admission; the premature neonates and term neonates were not separated. In each case, the nutritional support requirement was different; however, the same criteria (target calorie intake 60 kcal/kg/day and target protein intake 3 g/kg/day) were used to evaluate whether the correct nutritional support was achieved. Therefore, a well-controlled large-scale prospective study is needed to clarify the relationship between nutritional support and growth in infants immediately after surgery.
We concluded in this study that adequate protein supplement from the first day of surgery could have a positive effect on the growth velocity of neonates who underwent abdominal surgery. Especially, protein supply in the early neonatal stage seems to be important for improving the growth rates after surgery. Although additional research is needed to validate our results, active nutritional support, including appropriate nutritional monitoring, should be considered in neonates after abdominal surgery.
 XML Download
XML Download