

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As increase of maternal ages and improvement of neonatal intensive care, the survival of low birth weight infants following abdominal surgery have increased [12]. Acute abdomen such as necrotizing enterocolitis (NEC), spontaneous intestinal perforation (SIP), meconium-related ileus (MRI), and meconium non-related ileus (MNRI) was common in low birth weight infants. There are three different surgical options for acute abdomen: primary anastomosis, enterostomy formation, and peritoneal drainage. The safety and efficacy among 3 options are still controversial. While some studies have reported that primary anastomosis is a safe surgical treatment, others have reported that complications of primary anastomosis are more frequent than those of an enterostomy formation [34]. A randomized controlled trial between a peritoneal drainage and a laparotomy showed that an operative method does not affect survival rate [5]. Nevertheless, some studies have reported that peritoneal drainage is not effective, increasing mortality by 55% or needing a “salvage” laparotomy after drainage [67]. Currently, an enterostomy is accepted as a safe surgical method for infants with acute abdomen although the rate of its related complications has been reported to be 24%–68% [89].
When we could repair enterostomy has been controversial. Published studies are compared and summarized in Table 1. On their studies, inclusion criteria of subjects such as body weight, corrected age, and enterostomy maintenance duration at the time of enterostomy closure (EC) are variable. Among studies using enterostomy duration as inclusion criteria, the specific values of enterostomy maintenance duration also varied from each other (4, 8, or 10 weeks) [101112131415].
Table 1
Previous studies regarding the timing of EC

| Reference | Study year | Patient groups | Variables used to determine EC timing | Criteria to distinguish EEC and LEC | Results |
|---|---|---|---|---|---|
| Lee et al. [10] | 2014 | NEC | Body weight at enterostomy closure | 2,660 g | 10 times higher complication in EEC group |
| Festen et al. [11] | 1987 | Acute abdomen | Enterostomy duration | 4 weeks | No mortality and only 10% anastomosis leakage in EEC group |
| Struijs et al. [12] | 2012, 2017 | NEC | Enterostomy duration | 8 weeks | No significant difference between EEC and LEC in complication, PN duration, and hospital stay |
| Zani et al. [13] | |||||
| Banerjee et al. [14] | 2017 | NEC | Enterostomy duration | 10 weeks | Significantly high morbidity in EEC group |
| Kang et al. [15] | 2013 | Preterm with acute abdomen | Corrected age at enterostomy closure | 40 weeks | Significantly high complication in EEC group |
EC, enterostomy closure; EEC, early enterostomy closure; LEC, late enterostomy closure; NEC, necrotizing enterocolitis; PN, parenteral nutrition.
![]()
This article summarized points to consider before an EC and controversial points about the timing of EC in infants and neonates who underwent enterostomy for acute abdomen.
POINTS TO CONSIDER BEFORE AN EC
To determine the timing of EC, it is essential to judge whether there is a functional or mechanical disorder or not. Pathology review can reveal the cause of underlying surgical problem. Refeeding can resolve electrolyte imbalance and nutritional imbalances, and can estimate the function of distal bowels.
1. Loopography
As aforementioned, the distal loopography should be performed before EC to evaluate the necessity of other operations. It can determine post-operative complications and whether excrement is transitioned to the distal site [16]. Fig. 1A shows multiple stenosis of the large intestine following NEC. Fig. 1B shows a delayed contrast passage in the colon after 24 hours. In order to confirm the accuracy of loopography, Koivusalo et al. [16] have compared preoperative loopography and actual surgical findings in 25 patients with NEC and SIP. As a result, the positive predictive value was 100%. However, the sensitivity was only 38%. Specificity and negative predictive value were 100% and 77%, respectively. This means it is difficult to predict anastomosis complication through preoperative distal loopography. For the patient in NEC, distal loopography should be performed to evaluate postoperative stricture that can be shown in 32%–40% of patients [917].
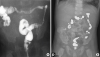 | Fig. 1(A) Colonic stricture after necrotizing enterocolitis. This colon study was obtained 3 month later after enterostomy formation. (B) A delayed evacuation of contrast agent with meconium-related ileus.
|
Despite importance of distal loopography, it could have several side effects. An intestinal perforation may occur by a tube while injecting contrast agent into the distal bowel. High osmotic pressure of the contrast may increase the amount of excrement, resulting in dehydration and high fever [18]. For this reason, careful observation is required during and after the examination.
2. Pathology review
The pathophysiology of a NEC is known to be an innate immune response to intestinal microorganisms that causes inflammation and injury to the intestinal tract of infant [19]. On the other hand, some studies have shown that a NEC in term infant might be related to ganglion cell of the intestine [20]. Patients who underwent surgery for NEC were classified according to their age and weight (term infants, 9 infants with weight of more than 2,400 g; immature infants, 8 infants with weight of less than 2,400 g). For small intestine specimens of each patient, 4 cases of aganglionosis were observed in the group of term infants whereas no such case was found in the group of immature infants. Although these results were obtained from a small number of patients, they implied that NEC in term infants might need to be determined to confirm the existence of ganglion cell.
Pathologic results of 13 MRI patients with very low birth weight infants have been reported [21]. Nevertheless, the relationship between pathologic findings and MRI has not been elucidated. The size or the number of ganglion cell nuclei did not show any significant difference between patients and control group of subjects who died from other causes whose gestational ages were similar to patients. But MRI has been reported to be associated with an intestinal ganglion cell abnormality in other reports [2223].
Regardless of the primary disease causing acute abdomen, Hirschsprung's disease should be kept in mind for the primary disease. But there is no evidence to perform rectal full thickness biopsy routinely for all acute abdomen patients in neonate. There is a paper analyzing the characteristics of colon perforation in neonates and infants [24]. Of 60 patients with colon perforation, 47 patients were diagnosed as Hirschsprung's disease. Although relatively high gestational age (mean, 36.39 weeks) in this study may reflect the potential different population with acute abdomen in preterms, this result can suggest rectal biopsy for colon perforation in near term neonates.
3. Refeeding
Refeeding refers to an injecting excretion from the proximal intestine into the distal intestine. As excretion from the proximal intestine contains much of nutrients with electrolytes, it can cause malnutrition with electrolyte imbalance. Refeeding makes distal intestine absorb these nutrients and electrolytes that can help to grow the patient and to correct electrolyte imbalance. [2526] The use of a total parenteral nutrition (TPN) to supplement nutrients can improve the nutritional status, but it can lead to serious complications such as cholestasis, liver failure, and central catheter infection [27]. Refeeding could prevent TPN related complications or reduce TPN dependence. [28].
Another advantage of refeeding is that the size discrepancy between proximal and distal bowel can be resolved [29]. As time passes after enterostomy formation, the distal bowel may develop disuse atrophy. Conversely, as patient grows, the proximal intestine may also grow together and gradually differ in size compared to distal intestine. Even if there is a difference in size, it can be anastomosed using an end-to-oblique anastomosis. However, if the size of the proximal intestine is large while the distal intestine is small, there may be an anastomotic leakage or a passage disturbance. The refeeding enables a safe anastomosis through the growth of distal intestine.
It is necessary for caregivers to be educated about refeeding if an EC is planned when patients grow up to a certain degree after discharge. If the caregiver is not educated as to how much, how often, how to refeed, or how to manage the stools, hematochezia or an intestinal perforation by tube could occur. Injecting contaminated stools into the patient's body through enterostomy might happen too. One study has reported how many bacteria can reproduce after collecting excretion from the proximal intestine in the pocket after a certain period of time [30]. Intestinal bacteria such as Escherichia coli and Escherichia faecalis can propagate to 105 colony forming units/mL within just 2 hours while anaerobic bacteria such as Bacteroides fragilis start to increase after 2 hours. The authors therefore have argued that it is dangerous to refeed what has been left for more than 2 hours after they are released.
There are many advantages to refeed before an EC: 1) It can be rather dangerous for the patient if it is not carefully supervised. It is necessary to thoroughly educate the medical staff and caregivers who will actually carry out the refeeding. 2) Since there are no studies conducted in the setting of high level of evidence like randomized controlled trial, it is difficult to say that this is necessary yet. It is better for medical staff to decide to do the refeeding or not after discussion with the caregivers about the benefits and side effects of the refeeding.
TIMING OF AN EC
Before discussion about the timing of EC, the definition of early closure or late closure was varied from study to study. In this review, the authors aimed to discuss the timing of the EC, not to find the right, exact timing of EC from many studies. It is beyond the scope of this review.
There are several factors that affect the time of an EC. If the proximal site is located at the jejunum rather than the ileum, an early closure needs to be performed since the amount of excretion may be significant, resulting in delayed growth or complications of the TPN. It is well-known that stenosis occurs at 6–10 weeks after surgery [31]. If EC is conducted too early, stenosis may proceed after the closure [16]. The general condition, corrected age, body weight, and underlying disease of patient need to be considered prior to EC.
Depending on results of pre-closure examination, the timing may change. Regardless of underlying cause of acute abdomen, distal loopography, pathology review, and refeeding were performed. When contrast agent does not fully evacuate after 24 hours in distal loopograpphy or when pathologic result suggests a hypoganglionosis or aganglionosis, or refeeding is not smoothly carried out, it would be safe to perform an additional test or observation some time. In MRI, rectal biopsy can be performed to distinguish Hirschsprung's disease.
An early closure presented in many articles has several advantages: 1) it can prevent and treat electrolyte imbalance and dehydration [32], 2) it does not have a high incidence of wound infection compared to late closure [113334], and 3) it could promote growth [3335]. In addition, it can potentially reduce medical cost and improve the quality of life of patients [36]. Early closure also enables to perform the surgery when there is small discrepancy in size between proximal and distal intestine [11]. In contrast to early closure, advantages of a late closure are less postoperative complication and early recovery. In addition, it can reduce TPN period after operation with early enteral nutrition and reduce of mechanical ventilator periods [1035]. Each procedure will be described in this report as follows.
1. Early closure
In 1982, Rothstein et al. [32] suggested the importance to conduct an early closure after enterostomy formation. They found that 6 out of 35 patients who underwent enterostomy for NEC needed re-hospitalization due to persistent diarrhea and dehydration. The range of body weight of the six patients was 2.20–3.97 kg while the amount of enterostomy excretion reached 225–450 mL per day. Composition analysis of enterostomy excretion showed higher sodium value than its value in the blood. After conservative management, EC was performed when patients reached at least 6-month-old. Dehydration, diarrhea, and electrolyte imbalance resolved in all patients. Based on this observation, the authors suggest that early closure would be beneficial to patients suffering from chronic dehydration and electrolyte imbalance after enterostomy formation.
In 1987, Musemeche et al. [37] reported results of an early closure. Seventeen out of 100 NEC patients suffered complications. The authors analyzed these patients based on their weights at the time of EC. Complications occurred in 24% of patients who were less than 2.5 kg and in 20% of patients with weight was 2.5–5.0 kg. Based on this, it was argued that early reversal did not increase the morbidity rate.
In the same year, results of early closure within 30 days after enterostomy formation were reported. Of 27 patients who underwent enterostomy due to NEC or volvulus, 22 of these patients underwent an EC within 30 days. Anastomotic leakage occurred in only 2 cases and no one died.
Data from the American College of Surgeons National Surgical Quality Improvement Program® did not show significant difference in the rate of wound infection for pediatric patients who underwent EC before 1-year-old between early 2012 and 2014 [34]. Wound infection occurred in 161 (7.6%) out of total 2,110 cases and 79 (6.8%) out of 1,157 under 1-year-old cases. The incidence of wound infection of prematurity was also found in 58 (7.6%) out of 767 cases, which was not significantly different from the incidence of wound infection of whole pediatric population. There were only congenital anomaly, especially Hirschsprung's disease affecting wound infections. Nutritional support, delayed growth, or weight loss of more than 10% did not affect the rate of wound infection.
Some researchers have argued that an EC should be conducted early because it shows a rapid growth after an EC. In fact, a previous study [35] has analyzed patients who underwent enterostomy formation within 20 weeks after birth. The average z-score of weight before EC was −0.747. It was significantly increased to 0.892 after the EC. The proportion of patients who had less than 0 z-score was 69.7%. This proportion was significantly decreased to 24.2% after EC. Another study reported that patients who had severe dehydration and diarrhea showed rapid growth after the closure [32].
In one study, 75 patients who underwent enterostomy formation due to NEC were divided into 2 groups based on the enterostomy duration (6 weeks). The number of patients who were re-hospitalized was smaller in patients who underwent early closure [36]. Total expenditure on medical care for patients with early closure did not show any significant difference from that for patients with late closure. Based on these results, the authors suggest that an early closure should be considered to improve quality of life if the patient is stable.
2. Late closure
As seen ahead, the benefits of early closure were reported in the 1980s. Since then, there has been few research on the timing of EC. In 2009, Al-Hudhaif et al. [38] published results contrary to previous studies. In their study, 37 patients who underwent enterostomy for pneumatosis intestinalis, intestinal obstruction, and septicemia were divided into two groups according to enterostomy duration of 10 weeks. Hospital stay, duration of mechanical ventilator, and TPN period were significantly longer in the group with early closure. This result might be due to the fact that the group with early closure had younger gestational age and lower body weight at the time of EC than those with late closure.
Banerjee et al. [14] also reported that patients who underwent EC earlier than 10 weeks after an enterostomy formation for NEC had a higher rate of morbidity compared to those who underwent after 10 weeks.
Two papers divided patients into two groups according to the presence or absence of complications [1035]. The gestational age at the time of EC was significantly lower (40+4 vs. 45+6) in the group with complication than that in the group without complication. The weight was also lower in the group with complication (2,200 g vs. 3,940 g) [10]. According to the logistic regression analysis of risk factors affecting complications, the body weight less than 2,660 g at the time of closure showed the odds ratio of 10.45, suggesting that body weight at the time of EC was a significant factor. Bethell et al. [35] reported similar results in their experience. A total of 24 patients with complications had less weight (3,655 g vs. 5,185 g) at the time of an EC compared to 34 patients without complications. In addition, patients without complications after an EC were born at near-term or higher gestational age at the time of enterostomy formation.
Kang et al. [15] reported the timing of EC using corrected age. Patients who underwent surgery for an acute abdomen such as NEC, SIP, and meconium plug syndrome were included. Results revealed that patients who underwent EC earlier than 40 weeks of corrected age showed longer period of mechanical ventilator dependence, TPN use, and hospital stay than those who underwent EC later than 40 weeks of corrected age. The period of full feeding also took longer in the group of patients who underwent an EC earlier than 40 weeks.
3. Controversial results
There are reports that there are no significant differences between early and late closure. The rate of major morbidity was studied for 89 patients aged under 6 months at the time of EC who were stratified into four groups based on their weight (<2.0 kg, 2.0–2.5 kg, 2.5–3.5 kg, and >3.5 kg) [39]. All factors considered, there were no statistically significant differences among groups. Only an incisional hernia occurred significantly in the group with weight <2.0 kg. Veenstra et al. [40] have analyzed patients who underwent enterostomy formation due to NEC by dividing patients into three groups based on the enterostomy duration: 8 weeks, 8–12 weeks, and 12 weeks. There were no significant differences in TPN-related cholestasis, TPN period, or mechanical ventilator period. Mortality or complications did not show significant difference among groups either.
Results from the most recent meta-analysis are not different from results noted above. Zani et al. [13] recently collected data from several papers regarding the EC after enterostomy formation due to NEC. They found that the timing of EC did not affect the period of TPN period, hospital stay, or complications when patients were divided based on enterostomy duration of 8 weeks.
CONCLUSION
Pre-closure evaluation is essential. Timing of the EC should be determined by distal loopography, pathology results, refeeding, patient age, weight, and enterostomy duration. The best time to perform an EC remains controversial. Individualized approach seems to be needed considering the benefit of a late closure or an early closure. Additional randomized controlled trials seem to be needed.
 XML Download
XML Download