

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Kawasaki disease (KD) is a type of acute, multi-systemic febrile vasculitis with an unknown etiology that can result in acquired heart disease in children [12]. Although gastrointestinal (GI) symptoms or signs are not part of the diagnostic criteria for KD, sonographic gallbladder (GB) abnormalities are reported as associated with intravenous immunoglobulin G (IVIG) resistance [345].
We report a case of a boy of 6 years of age with KD who presented with an unusually severe and prolonged course of GB hydrops.
CASE REPORT
A 6-year-old, previously healthy boy was admitted to our hospital due to a fever that persisted for 6 days. He was unresponsive to oral antibiotics treatment, had a sore throat and 3 days of abdominal pain, and exhibited decreased oral intake. He had no vomiting, diarrhea, or jaundice. On physical examination, his oral mucosal and tongue were fissured and hyperemic. Furthermore, he had bilateral conjunctivitis, unilateral cervical lymphadenopathy (right, 3×3 cm in size), and a maculopapular rash on abdomen; however, he exhibited no Pastia lines. Abdominal examination revealed abdominal distension and tenderness in the right upper quadrant (RUQ), but no signs of peritoneal inflammation or hepatosplenomegaly were observed.
Laboratory findings showed neutrophilic leukocytosis (22,560 cells/mm3, with 81% neutrophils), elevated erythrocyte sedimentation rate (118 mm/hr), C-reactive protein (CRP) (19.8 mg/dL), brain natriuretic peptide (BNP) (1,022 pg/mL), and decreased sodium (131 mEq/L). Liver function tests were hyperbilirubinemia (total bilirubin, 3.4 mg/dL) as well as elevation of aspartate transaminase (AST) (155 U/L) and alanine transaminase (ALT) (418 U/L). His abdomen radiograph revealed modest shadowing of GB distension and no specific findings (Fig. 1A and B).
 | Fig. 1Abdominal radiograph supine view (A) and erect view (B) indicated modest shadowing of gallbladder distension.
|
On the first day after admission, he received 2 g/kg IVIG and 50 mg/kg/day aspirin, following which his fever subsided and no further IVIG treatment was needed. His first echocardiography showed myocarditis (ejection fraction [EF], 45%) and mild ectasia of left main coronary artery (3.2–3.4 mm in diameter). On the second day after his admission, echocardiography (second follow-up) showed improved mild myocarditis (EF, 55%), improved ectasia of left main coronary artery (2.7–2.8 mm in diameter), and severe GB distension (8.9×4.6 cm in size), which possibly indicated GB hydrops (Fig. 2A). On the fourth day after his admission, although he had no fever and exhibited improvements in KD symptoms (i.e., eye injection, rash on abdomen, and cervical lymphadenopathy), he still complained of abdominal pain, distension, and tenderness of the RUQ. Follow-up laboratory findings were improved: neutrophilic leukocytosis (6,130 cells/mm3, with 33% neutrophils); decreased CRP (4.4 mg/dL), BNP (347 pg/mL), AST (40 U/L), and ALT (72 U/L); and improved hyperbilirubinemia (total bilirubin, 0.7 mg/dL). Echocardiography (third follow-up) showed normal completely improved carditis and still severe GB distension (10.2×5.5 cm in size) (Fig. 2B). Abdominal ultrasonography (US) was performed, which showed a markedly distended GB without stone, sludge, or wall thickening as well as normal bile ducts and liver morphology, which confirmed GB hydrops (Fig. 3A). On the sixth day after his admission, although his signs of KD had nearly disappeared, he still complained of abdominal discomfort, which had been moderately improving. The second follow-up abdominal US revealed a no notable change in GB distension compared to previous sonographic findings (Fig. 3B). An abdominal computed tomography (CT) scan was also obtained to exclude other hepatobiliary abnormalities, which showed similar findings as sonography, including a marked dilatation of the GB (8.0×5.5 cm in size) without stone, sludge, or wall thickening as well as normal bile ducts and liver morphology (Fig. 4). No complications necessitating surgical intervention had occurred and he was discharged 7 days after admission with only mild tenderness on the right upper-mid quadrant.
 | Fig. 2Echocardiography showed severe gallbladder distension (A) 8.9×4.6 cm in size and (B) 10.2×5.5 cm in size.
|
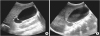 | Fig. 3Abdominal ultrasonography showed severe gallbladder distension (A) 9.8×4.9 cm in size and (B) 9.3×4.3 cm in size.
|
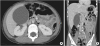 | Fig. 4Abdominal computed tomography (A, B) performed at 10 days after fever onset showed marked distended gallbladder (8.0×5.5 cm in size) without wall thickening or sludge, which is consistent with gallbladder hydrops.
|

DISCUSSION
The diagnosis of complete KD is based on typical clinical features, including fever for at least 5 days in the presence of 4 of the following conditions: bilateral non-purulent conjunctival injection, oral mucosal change (erythema or fissuring lips, strawberry tongue, or erythema of the oropharynx), cervical lymphadenopathy (over 1.5 cm in diameter), peripheral extremity change (edema or erythema of palms or soles, desquamation of tip of fingers, and toes), or polymorphic rash [26]. And the major sequelae of KD is related to the cardiovascular, specifically the coronary artery lesions which is leading cause of long-term morbidity [6].
Although GI symptoms do not belong to the typical diagnostic criteria, many patients with KD often have abdominal manifestations as part of their clinical features [6]. Abdominal pain and vomiting occurs commonly in patients with KD [367]. However, when persistent abdominal pain and distension, palpable mass, or jaundice were presented, clinicians should consider complications of KD such as GB hydrops or acute surgical abdomen.
Hydrops of the GB in children has been associated with systemic non-infectious disease and many infectious agents, including Epstein-Barr virus and leptospirosis [8910]. Among them, KD is most commonly associated with pediatric hydrops of GB [10], with an incidence rate of 5%–15% [561112]. KD with various GI symptoms that are suggestive of GB hydrops or acute surgical abdomen more frequently arise in older children [71314].
Generally, abdominal US is enough to identify the cause of abdominal symptoms and evaluate clinical course in patients with KD [5810]. Typical sonographic findings of GB hydrops include: GB enlargement (longitudinal and horizontal diameter greater than that for age-matched average values) with an elliptical shape and without change in anatomic abnormalities, such as increased wall thickness, sludge, or pericholecystic fluid collection [58]. However, further evaluations for excluding other GI disorders should be considered when abdominal symptoms persist or be worsen even after treatment for KD. In our case, abdominal CT was additionally performed because patient consistently complained abdominal pain and distension.
The management of GB hydrops associated with KD is mainly supportive care, such as intravenous fluids, analgesics, and GI rest and symptoms usually subside within 1 week of management [81314]. Surgical interventions should be considered only when the patient is unresponsive to supportive care or exhibits signs of complications (e.g., GB rupture and bile peritonitis secondary to rupture) [891213].
In this patient, other KD symptoms also slowly improved and have subsided entirely after 6 days of IVIG treatment without any sequelae. Previous case studies have reported that the symptoms of GB hydrops associated with KD were ameliorated within 15 days [8] or after 35 days [13] of admission. Usually, GB hydrops resolves or reduces in severity when the other KD symptoms improve after IVIG treatment. However, in our case, the GB hydrops persisted even after improvements in other KD symptoms. Moreover, the size of GB was completely normalized after 81 days of fever onset. The cause of prolonged and severe enlargement of GB hydrops in this patient is unclear. Kuijpers et al. [15] reported that immune system is generally implicated in the development of KD. Although there is no clear immunologic basis of GB hydrops with KD, this disease also may be associated with immune dysregulation. Thus, inappropriate immune response to vasculitis or inflammation that is secondary to KD may account for the delayed resolution of GB hydrops.
In conclusion, pediatricians should be aware that GI symptoms and signs, such as abdominal pain, distension and RUQ tenderness, can present with early stage of KD and also be a clue for diagnosis GB hydrops. Abdominal US should be performed to identify abnormal findings in the hepatobiliary tract, particularly GB hydrops. If necessary, additional abdominal imaging study should be considered for excluding other GI complications. GB hydrops associated with KD is spontaneously resolved with supportive treatment and has a good prognosis in most cases.
We experienced unusual case of markedly distended and prolonged GB hydrops associated with typical KD, even if treated promptly. When GB hydrops persist for long period such as our case, it is important to perform physical examination carefully and repeat follow-up abdominal US until the GB exhibits a normal morphology.
 XML Download
XML Download