

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recent trends in breast cancer surgery reflect an increasing proportion of mastectomies with breast reconstruction and a corresponding decreased proportion of breast-conserving therapies [1]. Although nipple-sparing or skin-sparing mastectomies provide superior aesthetic results, their efficacy and effectiveness in the treatment of cancer is still questionable [2]. In patients with total mastectomy, the creation of a nipple-areola complex (NAC) is the final stage of the breast reconstruction. Although this structure is only noticeable when the patient is undressed, patient satisfaction with the breast reconstruction is highly affected by the completion of this stage. Specifically, patients who undergo NAC reconstruction after breast mound reconstruction show significantly greater satisfaction compared to that in patients who do not undergo NAC reconstruction [3].
Although various techniques have been introduced for NAC reconstruction, a flattening of the reconstructed nipple is inevitable. The nipple projection demonstrates a major decrease during the first 3 months after surgery, becoming stable after 6 months, with 29%–60% of the projection reliably maintained over a 1-year follow-up [4567]. In an effort to allow additional insight into the long-term changes of the reconstructed nipple in accordance with the type of breast mound reconstruction performed, we reviewed a series of patients who underwent nipple reconstruction at our institution.
METHODS
Patients
Seventy-eight NAC reconstructions using the C-V flap technique were performed in 78 patients following breast mound reconstruction by a single plastic surgeon. Patients were divided into 3 groups according to the type of breast mound reconstruction: TRAM group underwent free transverse rectus abdominis myocutaneous (TRAM) flap reconstruction, latissimus dorsi (LD) group underwent LD myocutaneous flap reconstruction, and implant group underwent expander and implant-based reconstruction. The study was conducted in accordance with the Helsinki Declaration and was approved by Yonsei University Medical Center Institutional Review Board (approval number: 4-2018-0197). Given the retrospective nature of the study, informed consent was waived.
Surgical procedures
Nipple reconstruction was performed using a modified C-V flap technique. The tip of V-flap was modified into round shape that resembles U-shape for sufficient perfusion to the tip of flaps [8]. After the dermal flap was elevated, the subcutaneous fat tissue was thinned to prevent tension on the sutures, except at the base of the flap. Thus, the center of the flap had adequate fat tissue to maintain the blood supply and volume. The bilateral wings of the U-shaped flap were folded to form a barrel shape and were sutured with nylon. The skin was deepithelized along the newly constructed nipple base. The C-flap and V-flap donor sites were closed primarily (Fig. 1). Subsequently, nipple caps were applied to minimize external compressive forces on the neo-nipples in all patients.
Assessments
Nipple projection was measured from the base to the top of the reconstructed nipple, and nipple circumference was measured around the center of the reconstructed nipple using a flexible ruler. The first measure was performed approximately ten days after surgery, and the second measure was performed average 10 months after surgery, at the time when the tattoo procedure was performed. The maintenance was calculated in terms of the percent change from the first measurement to the second measurement. Both measurements were taken in the same manner at the outpatient department. Furthermore, in implant group, we evaluated the total inflationamount of expander before changing to a permanent implant, and analyzed the relationship between the amount of inflation and the change in nipple size.
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). Descriptive statistics are presented as means with standard deviations or as numbers and percentages. Group differences were evaluated in 1-way analyses of variance, with Bonferroni correction. In addition, we evaluated the nipple size according to the amount of inflation in implant group using the Pearson correlation coefficient. A P-value < 0.05 was considered statistically significant.
RESULTS
A total of 78 nipples were evaluated and the average follow-up duration was 10 ± 7 months. The patient demographics are presented in Table 1; no statistically significant differences were observed among the groups. The overall mean circumference and projection at the final measurement were 91.43% ± 7.11% and 62.16% ± 21.55%, respectively, of the immediate postoperative values. The decrease in the circumference over time did not significantly differ among the 3 groups (Table 2). In contrast, the decrease in the projection over time was significantly greater in group C (52.08%) compared to that in TRAM (66.49%) and LD (68.39%) groups (P < 0.05) (Fig. 2), with no significant difference between TRAM and LD groups (Table 2).
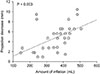
In addition, among the patients in implant group, greater inflation was significantly associated with greater decrease in the nipple projection (Fig. 3).
DISCUSSION
Among various reconstruction methods, including free composite grafts, nipple banking, opposite nipple sharing and tattoo alone, local flaps using the adjacent tissue followed by intradermal tattooing is the currently the most common method. Local flap techniques, such as Anton's star flap, Kroll and Hamilton double opposing tab flap [9], Bostwick C-V flap [10] and their modifications [1112131415], have continuously evolved since Little first described the skate flap in 1984 [16]. Although many techniques have been introduced, no specific technique has been proven to be superior. However, in the present study, breast mound reconstruction with autologous musculocutaneous flap techniques was found to achieve better long-term maintenance of the neo-nipple projection compared to that achieved with expanded tissue and implantation.
Several studies have shown a tendency for the reconstructed nipple to shrink over time, especially in terms of the projection, regardless of the reconstruction technique performed. Up to 50% postoperative shrinkage can occur following conventional nipple reconstruction [17]. A previous study evaluating three different pull-out flap techniques showed that the projection of the reconstructed nipple decreases the most during the first 6 months, 60% of the projection reliably maintained after 1 year [4]. Similarly, Few et al. [5] reported that a plateau in the shrinkage is reached by approximately 1 year after reconstruction, with an average loss of 59% in the nipple projection. In addition, Banducci et al. [7] reported that the postoperative shrinkage rate is up to 71%.
The maintenance of the long-term projection of the neo-nipple is a major challenge for reconstructive surgeons and greatly affects how patients feel about their reconstructed nipple. In a study on patient satisfaction in NAC reconstruction, patients were asked what they disliked most about the reconstructed nipple; more than 50% of the patients indicated that an excessive flattening of the nipple was most disliked. Previous authors have suggested the use of autologous remote tissue to improve the long-term maintenance of the nipple projection and minimize flattening. Brent and Bostwick first introduced the use of auricular tissue in 1977 [18], and Tanabe et al. [19] reported that 8 nipples reconstructed using auricular cartilage rolled inside bilobed dermal-fat flaps had a 94.6% maintenance rate. Guerra et al. [20] introduced a technique using an arrow flap with a rib cartilage graft and followed the size of the nipple projection for more than 7 years; the authors reported that all of the neo-nipples achieved an acceptable and reliable maintenance rate. Furthermore, Heitland et al. [17] reported a 25% decrease in the nipple projection over an average of 1 year after reconstruction using the same method as that in the study by Guerra et al. [20]. Yanaga made a further development, replacing the rolled auricular cartilage with artificial bone, which eliminates the risk of transferring cancerous cells back to the reconstructed breast, reduces donor-site morbidity, and decreases the operative time [21]. In addition, the postoperative nipple projection was maintained in all 100 patients. As a substitute for autologous tissue, acellular dermal matrix was first introduced by Nahabedian in 2005 [22]. AlloDerm (LifeCell Corp., Branchburg, NJ, USA) was used for augmentation in secondary and tertiary nipple reconstruction with an elongated C-flap and C-V flap. This method achieved an acceptable projection, regardless of the type of breast mound reconstruction. In 2007, Garramone and Lam [23] demonstrated the use of AlloDerm in primary nipple reconstruction. The technique involved the use of a modified star dermal flap pattern with the placement of an AlloDerm graft as a central core. However, only 56% and 47% maintenance was achieved at one year in the TRAM flap and tissue-expanded groups, respectively. Thus, the use of AlloDerm cannot be the ultimate solution for preventing nipple shrinkage. In contrast, Bernard and Beran [24] demonstrated satisfactory results at an average of 10 months follow-up using an autologous fat graft in cases with insufficient underlying subcutaneous fat.
In a previous study comparing the reconstructed nipple projection between autologous tissue-based mound reconstruction and implant-based reconstruction, the implantbased group showed worse results [13] consistent with the present results. Furthermore, the present study demonstrated a significant relationship between the amount of inflation in implant-based reconstruction and the projection decrease. After implant-based reconstruction, the expanded dermis of the breast mound loses its thickness via elastosis and zonal fragmentation of the elastic fibers [25]. This prevents the elevated dermal flap from being thicker, which results in more wound contraction. In addition, there is internal pressure that is applied to the surface of the breast, which tends to stretch and flatten the surface of the breast over time. Capsules around the implant also provide contractile forces, which leads to further projection loss. The closure of local defects would also create distorting forces onto the reconstructed nipple. Inadequate subcutaneous fat, external pressure, poor flap design, delayed healing, and tissue memory can also induce nipple shrinkage [2].
In autologous-based mound reconstructions, nipples reconstructed from the thicker dermis of the back skin associated with a LD skin island is far more resistant to contraction than are nipples reconstructed from the thinner dermis of a transverse rectus abdominis flap skin island. This is thought to be related to the natural progression of wound contraction during the healing process. Local flaps are elevated from the tissue of the breast mound, including the skin and subcutaneous tissue. Transplanted fatty tissue shrinks over time, whereas the dermal component shows less volume change; thus, flaps from a thick dermal region can better resist flattening. In a previous study on skin thickness in Korean adults, back skin was shown to be the thickest in the body, and chest skin was thicker than abdominal skin [26]. Dermal thickness followed the same pattern, while epidermal thickness was greatest in the chest, followed by the abdomen and back.
External pressure, such as wearing a bra, may aggravate the shrinkage. Previous radiation, wound infection, and inappropriate flap design may also compromise the flap circulation, resulting in delayed wound healing and further flattening of the reconstructed nipple. As many circumstances contribute to this unfavorable tendency of reconstructed nipple shrinkage, preoperative plans should be made with great care. Designing the flap as bigger than desired may be the first step in overcoming shrinkage. In our experience, when determining the size of the neo-nipple, all dimensions should be designed larger than those of the opposite side, regardless of the type of breast mound reconstruction. In terms of the nipple projection, if the breast mound is reconstructed with an implant after expansion, a larger design should be considered than that for an autologous-based reconstruction to compensate for future losses. In addition, delicate postoperative care, such as a soft plastic nipple cap, is essential for avoiding secondary dimensional loss.
In conclusion, breast mound reconstruction with autologous musculocutaneous flap techniques achieves better long-term maintenance of the neo-nipple projection compared to that achieved with expanded tissue and implantation. However, as the shrinkage of the neo-nipple is inevitable, the preoperative design should be oversized in accordance with the type of reconstruction of breast mound.




 XML Download
XML Download