

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Erectile dysfunction (ED) is the inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance [1]. The causes of ED are broadly divided into organic and psychological, but most of them are thought to be caused by organic components [1]. ED might be thought of as a natural consequence of the aging process; however, ED may occur as a result of specific illness. In fact, accumulated evidence suggests that ED may be another sign of cardiovascular disease [234].
According to the ‘artery size’ hypothesis, the clinical signs of atherosclerosis are likely to present earlier in small-sized arteries, such as the penile artery, than in relatively large-sized arteries, such as the coronary artery [56]. Applying the same logic, it is possible to detect vascular changes earlier in the smaller retinal or choroidal vessels of the eye than in the relatively larger penile artery [7].
The presence of diabetes mellitus increases the risk of ED [89]. Furthermore, a significant association has been shown between the severity of diabetic retinopathy and ED, suggesting a common microvascular compromise between the two conditions [10]. In patients with type 2 diabetes, narrower retinal arteriolar and wider venular diameters were independently associated with an increased risk of self-reported ED [11]. However, studies on the relationship between the status of the choroidal vessel and the severity of ED are scarce.
The choroid, like the corpus cavernosum, is a tissue with abundant vascularity [12], and phosphodiesterase type 5 (PDE5), which is associated with penile detumescence, is also found in the retinal and choroidal vasculature [13]. Thus, we hypothesized that there might be significant changes in the choroidal vascular structure of patients with ED. In this study, we investigated the morphological features of choroidal vasculature in patients with ED by analyzing choroidal thickness using optical coherence tomography (OCT).
MATERIALS AND METHODS
1. Participants
Between April 1, 2016 and December 31, 2016, patients who visited the urology clinic for the evaluation of ED were recruited for this study. Simultaneously, patients who visited the ophthalmology clinic for diabetic retinopathy screening, cataract evaluation, and symptoms of vitreous floaters or dry eye were also enrolled for the study.
2. Ethics statement
The study protocol was reviewed and approved by the institutional review board of Kangdong Sacred Heart Hospital (Seoul, Korea; IRB No. 2016-01-012). All study conduct adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all study participants after explanation of the nature and possible consequences of the study.
3. Inclusion and exclusion criteria
The study (ED) group consisted of male patients aged 20 to 70 years with ED, which was defined as an erectile function domain score of less than 26 on the International Index of Erectile Function (IIEF) questionnaire. Most of the patients in the ED group were recruited from the urology clinic; however, those who enrolled at the ophthalmology clinic and scored less than 26 on the IIEF questionnaire were also included in the ED group. The control group consisted of male patients aged 20 to 70 years who visited the ophthalmology clinic for one of the following: diabetic retinopathy screening, cataract evaluation, or symptoms of vitreous floaters or dry eye. Patients in the control group had an IIEF erectile function score greater than or equal to 26. The common exclusion criteria for both the ED and control groups were as follows: 1) previous history of PDE5 inhibitor intake within 3 months of study participation; 2) any diabetic retinopathy (e.g., microaneurysms, retinal hemorrhages, or hard exudates) on fundus examination; 3) retinal or choroidal disorders that might influence choroidal thickness, such as uveitis, central serous chorioretinopathy, or retinal vein occlusions; and 4) intraocular surgery, except for uncomplicated cataract surgery.
4. International Index of Erectile Function questionnaire
The IIEF is a 15-item self-administered questionnaire that was developed for assessing erectile function. It is a brief, reliable, and valid questionnaire containing questions in five domains: erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall sexual satisfaction [14]. The erectile function domain is calculated as the sum of the scores of questions 1 through 5 and question 15. For a 0.5 prevalence rate of ED, the cutoff point for ED was 25, with men scoring less than or equal to 25 being classified as having ED [15]. The erectile function domain is known to be a good diagnostic tool, not only in distinguishing the presence or absence of ED, but also in classifying levels of ED severity [15].
5. Ophthalmologic examinations and choroidal thickness measurements
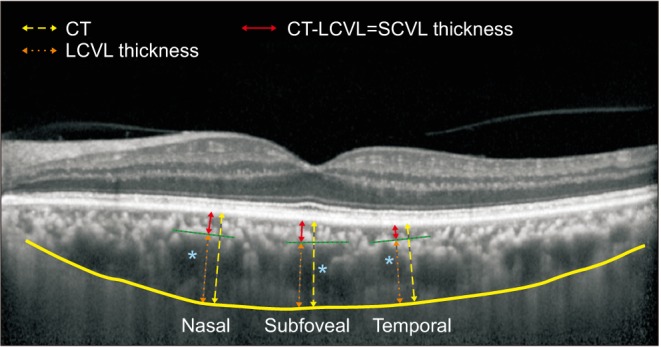
Patients underwent routine ophthalmologic examinations, including slit-lamp examination, fundoscopy, and OCT. Best-corrected visual acuities were measured using the Snellen chart and converted to logarithm of minimal angle resolution for statistical evaluation. Refractive errors were evaluated using an auto keratorefractometer (KR-8900; Topcon Corporation, Tokyo, Japan). Patients underwent indirect ophthalmoscopic examination and OCT (Spectralis OCT; Heidelberg Engineering, Heidelberg, Germany) to rule out any retinal disorders. Choroidal thickness and choroidal sublayer thickness were measured according to methods described in a previous study [1617]. In brief, choroidal thickness was measured using horizontal OCT scan centered on foveal center, which was taken by enhanced depth imaging mode with 100-line scan images averaged. Choroidal thickness was measured perpendicularly from the outer border of the hyperreflective retinal pigment epithelium to the inner sclera at three locations: at the fovea, 750 µm temporal to the fovea, and 750 µm nasal to the fovea. At the same locations, large choroidal vessels measuring 100 µm or more, located close to the choroid-sclera border, and closest to the choroidal thickness measurement locations were selected (Fig. 1, blue asterisks). Perpendicular lines from the innermost point of the large choroidal vessels were drawn (Fig. 1, green dashed lines), which intersected the choroidal thickness measurement lines (Fig. 1, yellow dashed arrows). Large-choroidal-vessel-layer (LCVL) thickness, which corresponded to Haller's layer, was defined as the distance between the intersection point on the choroidal thickness measurement line and the inner border of the sclera (orange arrows). Small-choroidal-vessel-layer (SCVL) thickness, which corresponded to the complex formed by the choriocapillaris layer and Sattler's layer, was defined as the difference between total choroidal thickness and LCVL thickness (Fig. 1, red arrows). The ratio of LCVL thickness to total choroidal thickness was also calculated. Two observers (YKK, JHL) independently measured choroidal thickness masked to the patient information, and data from the left eyes of the patients were used for evaluation. If there was more than a 30-µm difference between each measurement exceeding the previously reported value of interobserver coefficients of repeatability [18], the choroidal thickness measurement was re-reviewed and reassessed. The average values of the two observers were used in analyses. We averaged the choroidal thickness measurements at three different locations, i.e., subfoveal, temporal, and nasal locations, and this average value was used for analysis.
6. Statistical analyses
We compared average choroidal thickness and choroidal sublayer thickness between the ED and control groups by using Student t-test. In a previous study, subfoveal choroidal thickness was significantly lesser in patients with proliferative diabetic retinopathy or diabetic macular edema than in healthy controls. Although there were no significant differences in choroidal thickness between patients with nonproliferative diabetic retinopathy and healthy controls [17], we assumed that the presence of diabetes even without any diabetic retinopathy might also influence choroidal thickness. Thus, we compared the average choroidal thickness between patients with and without diabetes. We also divided the patients into subgroups according to the presence or absence of diabetes, and compared the choroidal thickness and its sublayer thickness between patients with ED and the controls in each subgroup by using the Mann-Whitney U-test. We performed multiple linear regression analysis for factors associated with SCVL thickness by using clinical factors such as age, refractive errors which is known to be associated with choroidal thickness, hemoglobin A1c level and duration of diabetes, which represented the severity of diabetes, anti-hypertensive drug use which may have vasodilatory effect and IIEF erectile function domain scores representing the severity of ED by using a stepwise regression approach. Statistical analyses were performed using statistical software (Stata ver. 14.0; Stata Corp., College Station, TX, USA) and statistical significance was defined as p<0.05.
RESULTS
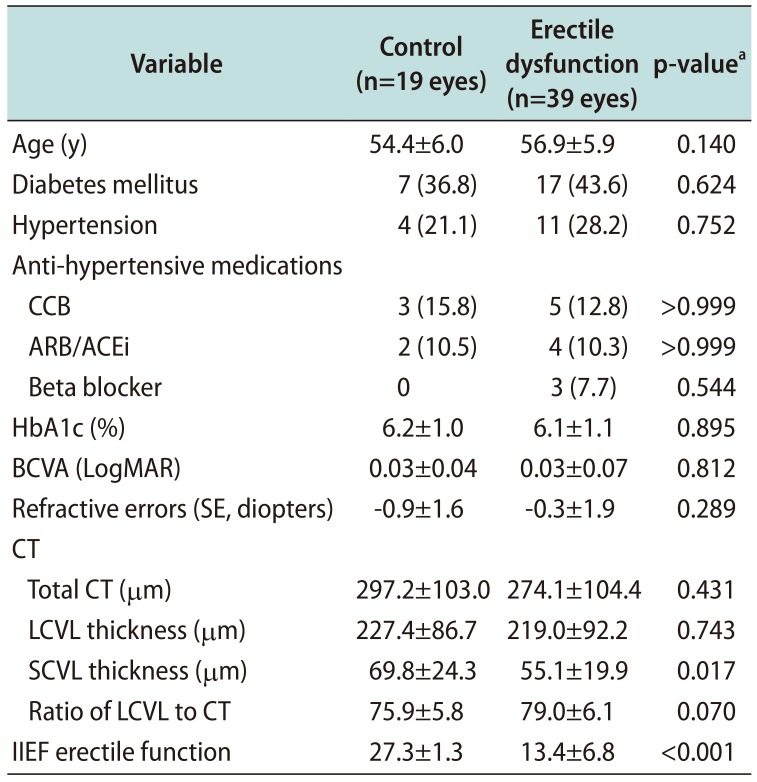
In this study, we enrolled 39 patients with ED into the ED group, and 19 patients without ED into the control group. Demographics, clinical characteristics, and choroidal thickness were compared between the two groups (Table 1). Interobserver reproducibility of the choroidal thickness measurements was excellent, with intraclass correlation coefficients ‘(2,1)’ values were 0.990, 0.990, 0.992 for subfoveal, temporal and nasal total choroidal thickness, respectively and 0.838, 0.871, 0.850 for subfoveal, temporal and nasal LCVL thickness, respectively. No significant intergroup differences were observed in terms of age, underlying diabetes or hypertension, use of anti-hypertensive drugs, visual acuity, and degree of refractive errors. No significant intergroup difference was observed in total choroidal thickness or LCVL thickness. However, SCVL thickness was significantly lesser in the ED group than in the control group (control, 69.8±24.3 µm vs. ED, 55.1±19.9 µm; p=0.017).
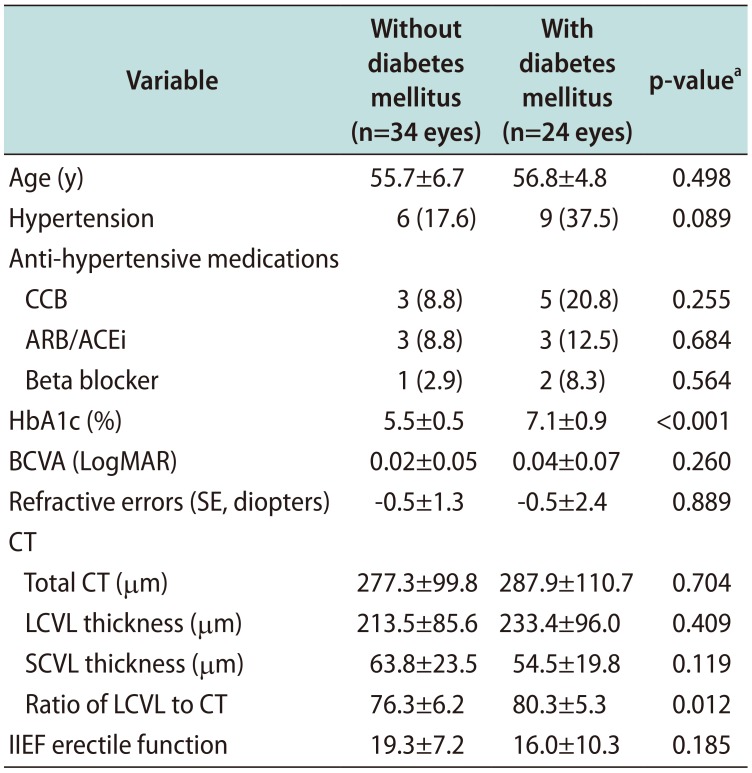
The comparison between patients with and without diabetes revealed no significant differences in terms of age, visual acuity, degree of refractive errors, and the IIEF erectile function score. Although no significant intergroup differences were observed in total choroidal thickness, LCVL or SCVL thickness, patients with diabetes showed significantly larger ratio of LCVL to total choroidal thickness (no diabetes, 76.3±6.2 vs. diabetes, 80.3±5.3; p=0.012; Table 2).
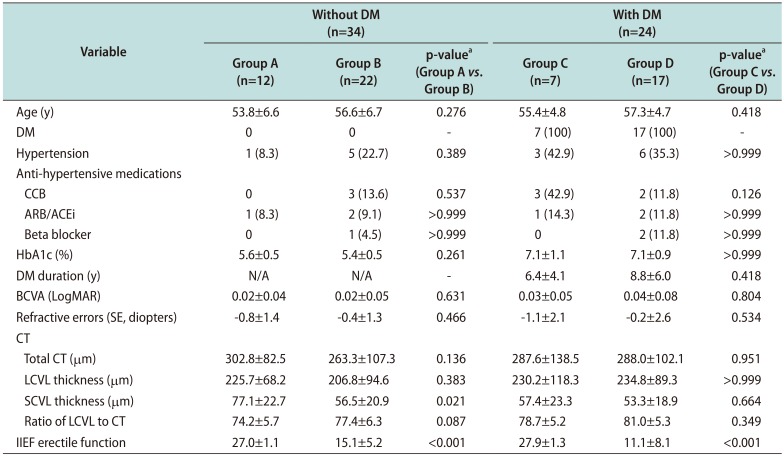
Among patients without diabetes, the ED group showed significantly lesser SCVL thickness (control, 77.1±22.7 µm vs. ED, 56.5±20.9 µm; p=0.021). In contrast, among patients with diabetes, no significant differences in choroidal thickness were observed between the control and ED groups (Table 3).
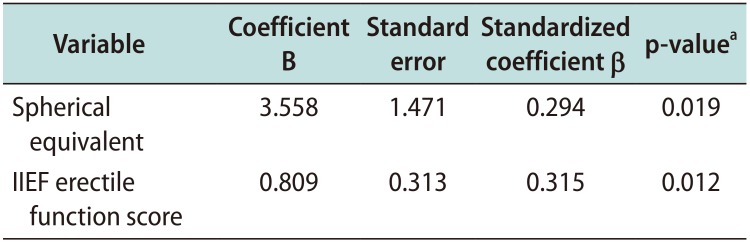
On multiple linear regression analysis, only refractive errors (spherical equivalent: standardized coefficient β=0.294; p=0.019) and the IIEF erectile function score (standardized coefficient β=0.315; p=0.012) showed a significant association with SCVL thickness (Table 4).
DISCUSSION
In this study, we investigated the morphological features of choroidal vasculature in patients with ED by measuring choroidal thickness using OCT. Our findings revealed no difference in overall choroidal thickness between the ED and control groups. However, the SCVL, which is thought to include the choriocapillaris layer and medium-sized choroidal vessels, was thinner in the ED group than in the control group, and SCVL thickness decreased in proportion to ED severity represented by the IIEF erectile domain function scores. Studies have shown that diabetes is a major risk factor for ED [81920], and ED severity is closely related to the severity of diabetic retinopathy [10]. Thus, in this study, we only included those patients with diabetes who did not have any diabetic retinopathy in order to reduce the effect of diabetic microvascular complication on the evaluation of ED and choroidal measurements. We also performed subgroup analysis according to the presence or absence of diabetes. Our results showed that SCVL thinning in the ED group was more evident among patients without diabetes.
The average SCVL thickness of subfoveal, nasal and temporal area was 69.8±24.3 µm in control group and 55.1±19.9 µm in ED group. Branchini et al [16] reported that the combined subfoveal medium-sized choroidal vessel layer and choriocapillaris layer thickness which is corresponded to our measurement of SCVL thickness was 52.9±20.6 µm in healthy eyes, which was lesser than that of our control group. This is thought to be due to the thicker overall choroidal thickness of our subject group and the ratio of LCVL to total choroidal thickness was similar between 0.7 to 0.8. In another study by the same group, SCVL thickness was significantly lesser in patients with proliferative diabetic retinopathy or diabetic macular edema than in healthy controls, but not significantly different between patients with nonproliferative diabetic retinopathy and controls [17]. Our study showed that there were no statistically significant differences in total choroidal thickness, LCVL or SCVL thickness between patients with and without diabetes, however, diabetic patients showed larger ratio of LCVL to total choroidal thickness, suggesting there is a tendency of lesser SCVL thickness in diabetic patients. Our results suggest that microvascular changes in choroidal vasculature may already occur in patients with diabetes but without retinopathy. A recent study using OCT angiography also revealed that choriocapillaris layer alterations were common not only in patients with diabetic retinopathy but also in patients with diabetes but without retinopathy [21].
In subgroup analysis, a significant difference in SCVL thickness was observed between the ED and control groups among patients without diabetes. However, no significant difference in choroidal thickness was observed between the ED and control groups among patients with diabetes. Thinning of the SCVL observed in the current study might appear as part of the microvascular complication manifested by ED or diabetes. However, the choriocapillaris layer accounts for only 5% to 10% of the total choroid [22]. Thus, in patients with diabetes whose SCVL has already been compromised, further SCVL damage caused by comorbid ED might be limited, and a larger number of patients will be needed to demonstrate the difference in SCVL thickness between those with and without ED. In contrast, among patients without diabetes, the ED group showed significantly lesser SCVL thickness than did the control group. This suggested that choroidal vasculopathy had already occurred in patients with ED without obvious ocular disorders, and that SCVL thickness could be a predictive factor of early vasculogenic ED. The results of multiple linear regression showed that only refractive errors and the IIEF erectile domain function score were significantly associated with SCVL thickness, thereby suggesting that SCVL thickness is associated with ED severity.
It is noteworthy that ED can be an early sign of cardiovascular disease as well as a disease in itself. The presence of ED predicted subsequent cardiovascular events to a degree either equal to or greater than that of current smoking or a family history of myocardial infarction [623]. Endothelial dysfunction is considered the common mechanism underlying ED and cardiovascular disease [462425], and the ‘artery size’ hypothesis posits that the symptom of atherosclerosis is likely to manifest earlier in arteries with a smaller diameter [5]. Because the present study was cross-sectional, we could not confirm whether patients with thin SCVLs subsequently developed ED or other systemic vascular diseases. However, there are possibilities that vascular compromise could be detected earlier in choroidal vessels with smaller diameters. The blood vessels of the eye are relatively easy to observe and evaluate than the blood vessels in other body parts; this factor needs to be investigated further.
Several studies have investigated the influence of systemic sildenafil on choroidal perfusion and thickness. Both choroidal perfusion and thickness are known to increase following ingesting systemic sildenafil, although it seems have no significant visual effects or even associated with ischemic complication [2627]. It will be noteworthy to evaluate the change in the thickness of each layer of the choroid after administration of sildenafil to fully investigate its effect on the eye.
This study has several limitations. The sample size is small, in particular, the number of patients in the group with diabetes but without ED was small because of the nature of this disease. We were not able to consider underlying medical conditions thoroughly, especially psychological factors, which are known to be associated with ED. Although there were no significant differences in terms of proportion of anti-hypertensive drug use between control and ED groups, it is difficult to know how these drugs have affected choroidal thickness. There might also be some errors in choroidal thickness measurement. Although we referred to a previous research method [1617], we used the average value measured at three macular points to reduce measurement errors. In addition, two observers independently measured choroidal thickness and showed good interobserver reproducibility. In this study, we excluded patients with any retinal or choroidal pathology that might affect choroidal measurements, such as patients with pachychoroid diseases, wherein the choriocapillaris layer might be reduced because of choroidal congestion in larger choroidal vessels [282930]. The choriocapillaris layer and medium-sized choroidal vessel layer could not be analyzed separately by using the current imaging device, and further studies using recent OCT angiography techniques might be warranted.
CONCLUSIONS
The thickness of the SCVL including the choriocapillaris layer and medium-sized choroidal vascular layer decreased in proportion to ED severity, and this phenomenon was more evident in patients without diabetes. These findings suggest that microvascular changes in the choroidal vessels may have already occurred in patients with ED without specific ocular diseases and that SCVL thinning may be an early sign of ED.
 XML Download
XML Download