

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Androgen receptor (AR) is the cornerstone of prostate cancer (PCa) development and progression [1]. Altered AR status is the most important mechanism by which PCa develops into castration resistant prostate cancer (CRPC), the last stage of PCa [234]. Recently, new AR modulators have been developed for CRPC treatment that overcome the altered AR expression and can predict the treatment response [567].
AR variants (ARVs) in circulating tumor cells, not prostate tissue, have been studied as a prognostic predictor [5]. In clinical practice, liquid biopsy is more valuable than target organ biopsy; however, changes in the expression of AR and other markers must be evaluated in target organs to accurately understand the disease mechanism. Unfortunately, studies using human PCa tissue have been limited; thus, to evaluate AR expression in PCa, most studies have used cell lines rather than human prostate tissue [89]. It is unclear how AR expression increases or decreases or how it affects the progression of PCa in the prostate.
AR or ARV status is widely known to be important for the therapeutic response and prognosis of PCa progression to metastatic CRPC [35]. However, in localized PCa, the role of AR is considered to be less important because local therapy, such as radical prostatectomy (RP) or radiation is used rather than systemic androgen deprivation therapy (ADT). High-risk PCa can recur after local treatment, eventually leading to metastasis and CRPC. AR plays an important role in this process and may be an ideal prognostic factor in localized PCa. Several studies have reported AR and ARV expression in localized PCa following RP [10111213141516]. In these studies, AR expression in RP specimens was inconsistent. Several studies have reported that AR expression is increased, but in other studies, this change was neither prominent nor proven [12]. No specific conclusions have been drawn regarding the effect of AR on biochemical recurrence free survival (BCRFS) following RP. Most of the previous studies have used immunohistochemistry (IHC) or quantitative real-time polymerase chain reaction (qPCR) with microdissection, and no attempt has been made to quantitate AR, or ARV, protein in human PCa tissues.
To evaluate the role of AR and its ARVs in PCa progression, we compared the expression of those among human benign, localized PCa, and metastatic CRPC tissues. In addition, the relationship between AR expression and BCRFS following RP was investigated using qPCR and Western blotting (WB) techniques.
Go to : 
MATERIALS AND METHODS
1. Ethics statement
This study was approved by Institutional Review Board of Pusan National University Yangsan Hospital (IRB Number: 05-2016-094) and proceeded through a legitimate procedure from the regional tissue bank. Informed consent was waived by the IRB based on tissue bank approval.
2. Tissue preparation
A total of 282 cases were evaluated, including 252 localized PCa, 8 metastatic CRPC, and 22 benign prostatic hyperplasia (BPH) cases. Among the metastatic CRPC patients, 3 received docetaxel chemotherapy and post-chemo enzalutamide, 3 received chemotherapy, and other 2 received ADT only. From 2013 to 2015, fresh tissues were collected from patients who underwent RP or transurethral resection of the prostate in Pusan National University Yangsan Hospital and were stored in ethically approved tissue banks. Immediately after arriving at the pathology department, small samples from the putative tumor area were dissected and snap frozen in liquid nitrogen.
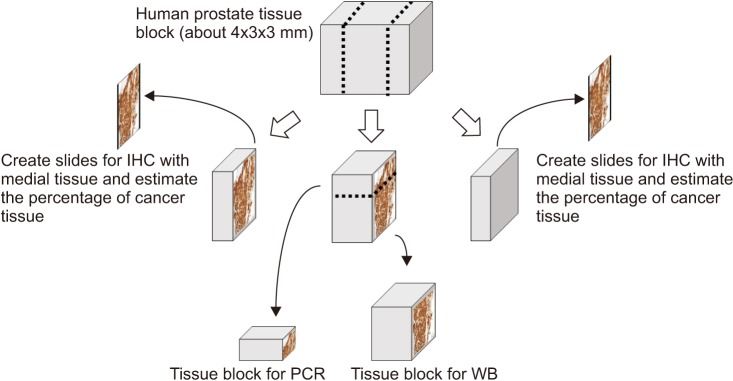
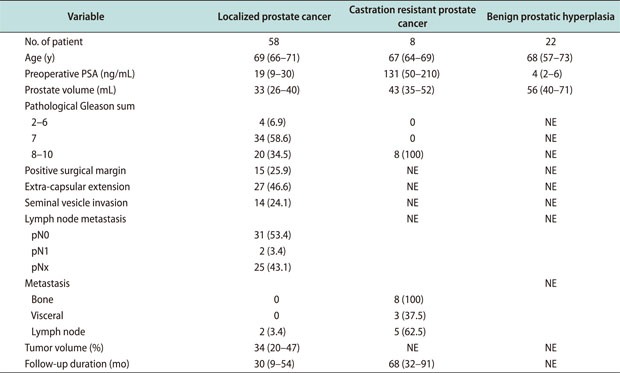
Each fresh tissue block from men with PCa was divided into three sections: the two ends were made into paraffin blocks for IHC, and the middle section was divided into two sections for WB and qPCR (Fig. 1). Histopathological evaluation including Gleason scoring was used to determine the type of lesion. Each tissue was confirmed again as cancerous tissue (greater than 80%) using H&E staining on both ends of the paraffin block. All prostate cancers were identified by two experienced uro-pathologists (SDH & LHJ). Among the 252 localized PCa cases, only 58 cases were identified as sufficient tumor tissue to include in the analysis. Benign prostate tissue extracted with the transurethral resection of the prostate was selected randomly by the whole tissue and included in this study. Their demographics and pathological characteristics were described in Appendix.
qPCR and WB were performed for AR and ARV7 expression in fresh tissue prepared by the above method. The RNA integrity number was used to evaluate the stability of the fresh tissue block, and sample specimen values were maintained above 7.5.
3. Quantitative real-time polymerase chain reaction
Total tissue RNA was extracted using Trizol reagent (Invitrogen, Life Technologies, Carlsbad, CA, USA) according to the manufacturer's instructions. Synthesis of cDNA was performed on 2 µg RNA using PrimeScript™ 1st strand Synthesis Kit (TAKARA, Shiga, Japan) according to the manufacturer's instructions. The AR, ARV7, and ARV1 primer sequences are as follows: 5′-CTTACACGTGGACGACCAGA-3′ (AR forward), 5′-GCTGTACATCCGGGACTTGT-3′ (AR reverse), 5′-CACCATGGAAGTGCAGTTAGGGCTGGGAAGGGTCTACCCT-3′ (ARV7 forward), 5′-TCAGGGTCTGGTCATTTTGAGATGCTTGCAATTGCC-3′ (ARV7 reverse), 5′-CCATCTTGTCGTCTTCGGAAATGTTATGAAGC-3′ (ARV1 forward), and 5′-CTGTTGTGGATGAGCAGCTGAGAGTCT-3′ (ARV1 reverse). Gene expression levels were measured by relative quantification between RNA samples, and fold expression changes were determined. All qPCR experiments were performed in triplicate, and the housekeeping gene glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as a normalization control.
4. Western blot
Total 60 µg protein was separated by polyacrylamide gel electrophoresis, transferred onto a nitrocellulose membranes and were blocked with 5% nonfat milk in Tween 20 in tris-buffered saline buffer. The membranes were then incubated with goat anti-mouse antibodies for AR (Cell Signaling, Danvers, MA, USA), ARV7 (Precision, Columbia, MD, USA) and β-actin (Santa Cruz, Dallas, TX, USA). Immuno-detection was performed using an enhanced chemiluminescent Western blot detection system (Pierce, Waltham, MA, USA). The intensity of the bands was assessed relative to their respective β-actin bands with LAS-3000 software (Fujifilm Medical Systems, Stamford, CT, USA). These tests were repeated at least two times per sample and analyzed as averages.
5. Immunohistochemistry
IHC was conducted with a rabbit monoclonal antibody against recombinant human AR (Cell Signaling) and a mouse monoclonal antibody raised against recombinant human ARV7 (Precision). The human prostate tissues that has undergone the abovementioned processes were cut into five-micron-thick sections; these sections were deparaffinized and subjected to antigen retrieval using 10 mM citrate buffer at 92℃ for 30 minutes. After deparaffinization and rehydration, the endogenous peroxidase activity was quenched in 3% hydrogen peroxide/methanol for 10 minutes, and the sections were incubated with primary antibody for 2 hours at room temperature. A dilution of 1:200 was used for AR and ARV7. For Gleason grading, all cases were stained with H&E. The number and intensity of immunoreactive nuclei was assessed by one pathologist (LHJ) without any knowledge of the clinical data. Intensity was scored on the following scale: 0 (negative staining), 1 (weak staining), 2 (moderate), and 3 (strong) [17]. Only grades 2 and 3 were classified as positive. The proportion of positive cases in each group was compared and analyzed.
6. Statistical analysis
Statistical calculations were performed using the Statistical Package for Social Sciences (SPSS) for Windows software ver. 13.0 (SPSS Inc., Chicago, IL, USA). The mean AR/ARV expression from qPCR and WB results was compared to the disease status (BPH vs. localized PCa vs. CRPC).
BCRFS was analyzed in 58 patients with localized PCa according to AR and ARV7 expression via PCR, WB, and IHC. AR or ARV7 positivity in qPCR or WB was defined as an expression level exceeding that of GAPDH or β-actin, respectively. BCRFS in 58 patients with localized PCa was analyzed according to the expression of AR and ARV7 in qPCR and WB using the Kaplan-Meier curve. All tests were two-sided, and significance was set at 0.05.
Go to :
RESULTS
1. Androgen receptor and its variant expression according to disease status
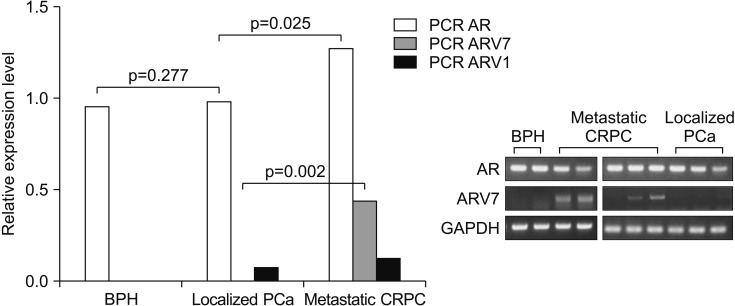
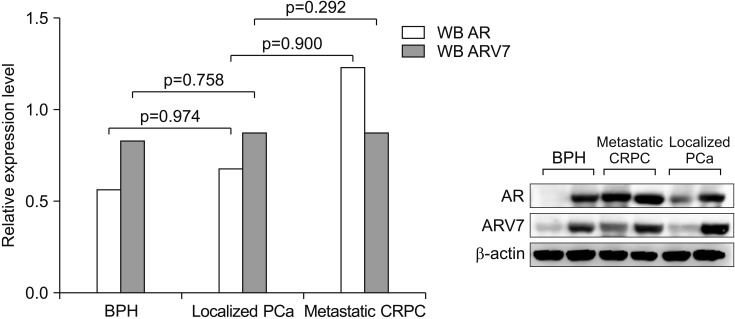
qPCR results revealed that AR and ARV7 mRNA expression was higher in CRPC tissues than in localized PCa tissues (p=0.025, p=0.002, respectively) (Fig. 2). However, AR and ARV7 mRNA expression between localized PCa and BPH tissues was not different. In CRPC tissues, AR protein expression was high, as determined via WB, but was not statistically significant (Fig. 3). ARV7 protein expression among the groups was not significant due to the severe expression heterogeneity in each group.
The nuclear expression of AR via IHC was uniformly high in all groups (Fig. 4, 5, 6). AR expression in the stroma was so heterogeneous that, in each case, AR expression was determined with epithelial AR expression. ARV7 positivity as determined by IHC was more common in CRPC tissues than in localized PCa tissues. However, clear nuclear ARV7 immunoreactivity was confirmed not only in cancer tissue but also in adjacent benign tissues. In addition, in BPH tissue, nuclear ARV7 immunoreactivity was weak but detectable.
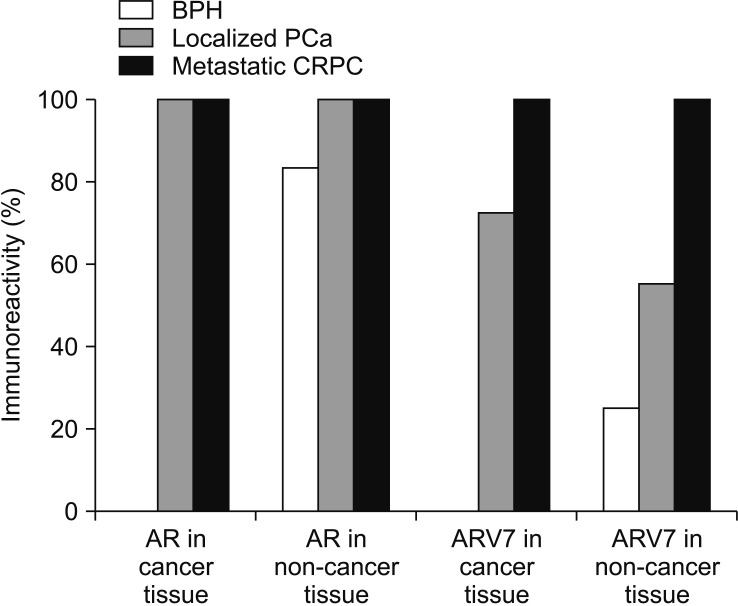 | Fig. 4Although the nuclear expression of androgen receptor (AR) via immunohistochemistry was uniformly high in all groups, the immunoreactivity of AR variant 7 (ARV7) was higher in the metastatic castration resistant prostate cancer (CRPC) tissues than in the other diseased tissues. BPH: benign prostatic hyperplasia, PCa: prostate cancer.
|
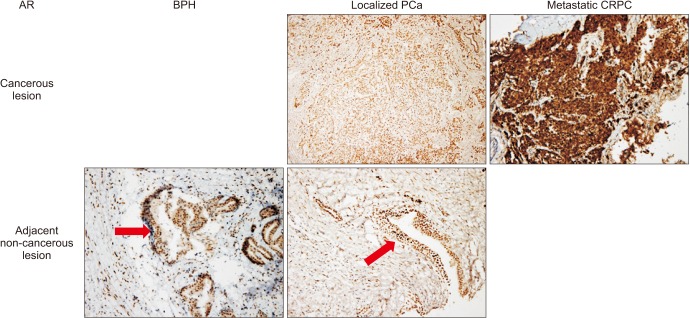 | Fig. 5Androgen receptor (AR) (brown) expression in benign prostatic hyperplasia (BPH), localized prostate cancer (PCa) and metastatic castration resistant prostate cancer (CRPC) tissue. Arrows indicate AR nuclear immunoreactivity in non-cancerous tissue at 10× magnification (immunohistochemical stain).
|
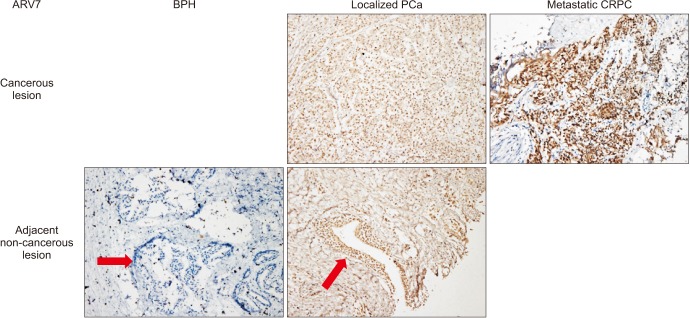 | Fig. 6Androgen receptor variant 7 (ARV7) (brown) expression in benign prostatic hyperplasia (BPH), localized prostate cancer (PCa) and metastatic castration resistant prostate cancer (CRPC) tissue. Arrows indicate androgen receptor nuclear immunoreactivity in non-cancerous tissue at 10× magnification (immunohistochemical stain).
|
There was no significant association between AR or ARV7 expression and Gleason score in localized PCa (p=0.688, p=0.233, respectively).
2. The relationship between biochemical recurrence free survival and androgen receptor expression following radical prostatectomy
The median age, preoperative prostate specific antigen (PSA), and follow-up duration in men, who had localized PCa and analyzed for BCRFS, was 69 years old (interquartile range [IQR], 66–71 years old), 13.3 ng/mL (IQR, 9.1–29.9 ng/mL), and 35 months (IQR, 19–30 months), respectively. The number of high (8–10) and low (6, 7) Gleason grade was 38 (65.5%) and 20 (34.5%), respectively. Twenty-four patients (41.4%) underwent biochemical recurrence after RP.
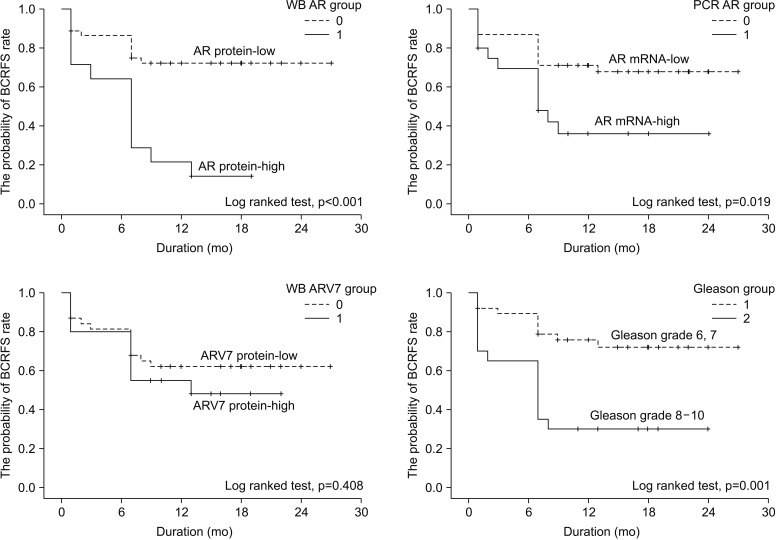
The high AR expression determined with PCR and WB was associated with a low BCRFS rate (log-ranked, p=0.019, p<0.001, respectively) (Fig. 7). The ARV7 expression level from qPCR and WB results was not associated with BCRFS. A high Gleason grade (8–10) was also associated with a low BCRFS rate (log-ranked, p=0.001).
Go to :
DISCUSSION
To investigate the expression of AR in PCa samples, AR protein and gene expression has been examined using several research models. Previous studies have shown a heterogeneous expression of AR and histological changes [101112141618]. Particularly, existing studies have used a wide variety of research methods, such as cell line, xenograft, and human specimen study models. The results were also conflicting due to the PCa and experimental method heterogeneity. Most studies on AR expression that have used human prostate tissues are mainly based on qPCR and IHC detection methods. qPCR has even been used as a method with recent laser microdissection techniques [1416]. The collection of fresh human tissue is limited, and WB has many obstacles because of necessary time constraints and the required cooperation of various experts. This study is the first to analyze AR protein expression in human PCa specimens using WB. In the present study, immediately after surgery, tumor tissues and normal tissues were separated and stored at the human tissue bank with the help of a uro-pathologist. At the start of this study, the distribution of the tumor in the collected tissue blocks was re-checked. WB can compensate for the shortcomings and heterogeneity of previous qPCR and IHC results. Quality control of the specimens used in the experiments was also performed. To assess RNA degradation, the present study used the RNA integrity number, a numerical representation of electrophoretic measurements of RNA integrity.
The results of previous studies on the effect of AR expression on PCa prognosis were inconsistent, and some studies even presented opposite results [101112141618]. Among the studies using human PCa specimens, several classic studies found that patients with high AR expression had improved responsiveness to androgen deprivation and therefore had higher survival rates [1018]. However, since then, the results from investigating BCRFS following RP have changed the interpretation of AR expression. Sweat et al [11] evaluated AR expression in the prostate and extracted lymph nodes in 197 RP and lymphadenectomy specimens. In that study, high AR immunoreactivity in lymph node metastases was predictive of poor cancer specific survival. Li et al [12] reported IHC results for AR immunoreactivity in 640 RP specimens. This research group found that high AR expression levels are associated with aggressive disease and are independently predictive of decreased BCRFS. Using qPCR, Rosner et al [14] reported that the quantitative determination of AR gene expression levels in prostate epithelial cells may be useful for predicting BCRFS after RP. Finally, the study by Minner et al [16] was the largest study, including 2,805 RP specimens, and showed no association between AR expression via IHC with BCRFS following RP. Because of these inconsistent results, the association between AR expression and PCa prognosis has not been clarified.
Similar to previous other studies, the present study also showed that AR expression has high immunoreactivity in benign and malignant tissue including metastatic CRPC tissues. Although AR expression is relatively high in CRPC tissues compared with benign and localized PCa tissues, this difference was not significant. One thing to note is that AR expression was heterogeneous even within the same group. To determine the significance of this heterogeneity, we analyzed the association between prognosis and AR expression in localized PCa. In localized PCa, high AR protein expression via WB was related to poor BCRFS. High AR gene expression using qPCR also confirmed this relationship with poor BCRFS. However, high IHC AR immunoreactivity was not associated with survival after surgery since AR immunoreactivity was high in all tissues. This study is the first to analyze the association between prognosis and AR protein expression in human PCa tissues using WB.
The conflicting clinical study results using human PCa specimens might be explained by AR from the stromal or epithelial compartments playing different roles in PCa progression. Most previous studies were performed using total (stromal & epithelial) PCa specimens without knowing the relative contribution of the stroma and epithelium within the sections. Several studies have analyzed AR expression in each area. For over a decade, stromal AR expression has been inversely related to Gleason score, treatment response, metastasis, and biochemical recurrence after RP [131519]. Recently, Leach [20] reported the association between the decrease in stromal AR levels and the increase in PCa-related death. Rosner et al [14] quantified AR mRNA expression in microdissected paired malignant and benign prostate epithelial cells from a large cohort of RP specimens. AR mRNA expression was lower overall in tumor cells; however, patients with increased AR mRNA expression in tumor cells compared to benign cells had a lower BCRFS rate. The increased AR mRNA expression level may contribute to PCa progression. The Rosner et al [14] suggested that the quantitative determination of AR mRNA expression in prostate epithelial cells may be useful for predicting PSA recurrence. This suggestion is supported by experimental evidence that PCa growth in vitro and in vivo is inhibited by antisense oligonucleotides that downregulate AR mRNA and protein expression [21]. Henshall et al [19] was the first to report that the concurrent overexpression of AR in the malignant epithelium and the loss of AR immunoreactivity in the adjacent stroma were associated with higher clinical stage and earlier biochemical recurrence after RP. Similarly, Ricciardelli et al [13] reported that the shortest time to relapse and the highest relapse rate was for patients presenting with both high AR in the malignant epithelial cells and low AR in the peritumoral stromal cells.
Collectively, patients with high AR expression in the epithelial cancer tissue are assumed to have poor BCRFS, whereas low AR expression in the surrounding benign and cancer-associated stromal tissues correlates with low BCRFS. Most PCa tissues are composed of more epithelial cancer cells than stromal cells. Therefore, AR expression in the whole tumor tissue depends on epithelial cancer tissue AR expression. This is consistent with results showing that men with high AR expression in only PCa tissue have poor BCRFS. In other words, high AR expression in tumor tissue alone can be considered a poor prognostic factor. This is the first study to show that the inverse correlation between AR mRNA expression and BCRFS after RP is also consistent at the protein.
Several previous studies revealed that increased ARV expression was associated with a low BCRFS after RP in hormone-naïve PCa patients [2223]. Among the ARVs, Hu et al [22] emphasized the significance of ARV7 and ARV1. ARV1 and ARV7 mRNA expression was on average 20-fold higher in CRPC tissues (n=25) compared with hormone-naïve PCa tissues (n=82; p<0.001). This study group also suggested that increased ARV7 expression predicted BCRFS in men with localized PCa following RP (p=0.012). Guo et al [23] reported results from an IHC analysis of tissue microarrays for ARV3. This study used 429 human prostate samples, including 40 BPH, 371 hormone-naïve PCa, and 18 CRPC samples. These results reveal that ARV3 is significantly up-regulated during PCa progression and that ARV3 expression is correlated with low BCRFS after RP. In our results, ARV expression was higher in CRPC patients than in hormone-naïve patients, but the prognostic value of ARV expression was not significant. This difference is presumably due to the rare expression of ARV7 in localized PCa tissues in our results. Other studies have also failed to prove that ARVs are significant predictors of BCRFS. Zhao et al [24] measured ARV7 and ARV1 expression using a branched chain DNA assay in a localized PCa cohort (n=52). This group concluded that the ARV1 or ARV7 transcript level does not predict BCRFS in patients with localized PCa following RP.
There are several inevitable limitations. First, only 58 RP specimens out of 252 localized cases were available for analysis because of insufficient tumor tissue for WB. It is possible that this analysis focused on patients with large tumor masses. However, it would be impractical to collect large fresh tumors in RP specimen with small tumor volume. Second, the follow-up period for analyzing BCRFS was relatively short. Lastly, we evaluated only ARV7 and ARV1 via qPCR. To evaluate the diversity and complexity of human AR splice variants, future studies must focus on better understanding the aggregate effects of full-length AR and its ARVs, which all together may be relevant to PCa progression or prognosis.
Go to :
CONCLUSIONS
Although AR nuclear immunoreactivity was highest in human metastatic CRPC tissue, it was consistently present in all BPH and localized PCa tissue. The expression of ARV7 was heterogeneous, specifically in PCa specimens. Although ARV7 mRNA expression is increased in human metastatic CRPC tissue, the protein level is not. When ARV7 expression was positive in cancer tissues, it was also positive in the adjacent benign tissues.
Although the high AR protein and mRNA expression in the tumor tissue of RP specimens was associated with a low BCRFS rate, those with high ARV7 expression were not.
Go to :
 XML Download
XML Download