

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Varicocele is an abnormal dilatation and tortuosity of the internal spermatic veins within the pampiniform plexus of the spermatic cord [1]. The reported prevalence of varicocele varies; however, it is generally estimated at approximately 15% [2]. Although most men remain asymptomatic, the most common clinical symptoms include infertility and chronic scrotal pain [1]. Varicocele is a major cause of impaired spermatogenesis and the most common correctable cause of male infertility [3]. It is found in approximately 40% of men with primary infertility and in 80% of men with secondary infertility [4]. About 2% to 10% of men with varicocele complain of pain, mainly in the scrotum or in the inguinal area [5]. Varicocelectomy for male infertility has been investigated far more than pain. The cause of pain due to varicocele is not well understood. Hence, we conducted this review focused on pain in varicocele.
Go to : 
ETIOLOGY
The etiology of pain associated with varicocele is not completely understood. However, infertility due to varicocele is a possibility, as varicocele affects spermatogenesis and the function of Leydig cells, by increasing the testicular temperature, venous pressure, hypoxia, oxidative stress, hormonal imbalances, and/or the reflux of toxic metabolites of adrenal or renal origin [67891011]. These testicular injuries not only lead to infertility but also testicular pain. Compression of surrounding neural fibers by the dilated venous complex is an additional factor causing pain associated with varicocele [12].
Go to :
PRESENTATION AND EVALUATION
Testicular pain associated with varicocele is typically described as a dull, aching, or throbbing pain in the testicle, scrotum, or groin; rarely, it can be acute, sharp, or stabbing. Varicocele is also described as scrotal heaviness that worsens with exercise, activity, or after standing for a prolonged duration. The patient's history should also reveal details of the pain including acuity of onset, severity, location, quality, timing, and radiation to other locations. Aggravating and alleviating factors should be discussed as well, with an emphasis on urinary habits, bowel movements, and sexual and physical activities.
Varicocele is typically asymptomatic although a few men complain of testicular pain. Usually, adult men with varicocele are diagnosed during evaluation of infertility, and varicocele in adolescents is discovered incidentally on physical examination. Therefore, physical examination is the most important diagnostic test for varicocele. Scrotal inspection and palpation should be performed with the patient in standing and supine positions, with and without a Valsalva maneuver, in a warm room, to facilitate relaxation of the cremaster and dartos muscle fibers of the scrotum. The standard grading system used for varicocele is: grade 1, palpable only during Valsalva maneuver; grade 2, easily palpable but not visible; and grade 3, easily visible [13]. Grade 0 (subclinical) varicocele is visualized using Doppler ultrasonography but is nonpalpable.
The use of imaging workup is not recommended in all varicocele patients with testicular pain. However, varicocele can be evaluated on a numerical scale and detected clearly in case of indeterminate or difficult physical examination, by imaging study. Additionally, the examination allows exclusion of other potential intrascrotal or abdominopelvic pathologies and facilitates the accurate measurement of the size of both testicles. Pelvic doppler ultrasonography is the most common and important imaging workup for men with testicular pain. It is an economical and non-invasive tool with high sensitivity, and can be used in the outpatients' room. Additionally, computed tomography or MRI of the abdomen and pelvis provide comprehensive anatomical views of areas that contribute to referred testicular pain.
It is essential to conduct a diagnostic workup for any male with testicular pain to rule out other possible causes of pain, even when a clinically palpable varicocele is present on physical examination. A broad differential diagnosis for chronic testicular pain includes pain due to scrotal condition, post-procedural pain and referred pain (Table 1) [14]. Scrotal conditions causing testicular pain include testicular tumors, varicocele, spermatocele and hydrocele. Iatrogenic injury following vasectomy or hernia repair may trigger post-procedural testicular pain. Referred pain from a variety of causes such as a mid-ureteral stone, and indirect inguinal hernia are also considered in the differential diagnosis of orchalgia.
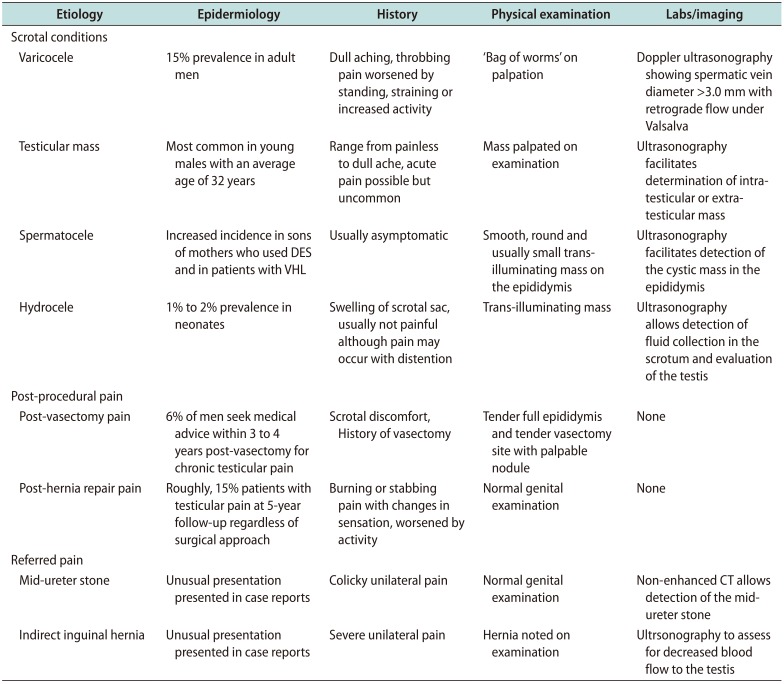
Table 1
Differential diagnosis of chronic testicular pain
![]()
Go to :
TREATMENTS
1. Medical management
The management of varicocele with testicular pain should begin with conservative treatment and a period of observation, which are effective in a few patients. A prolonged period of observation allows alleviation of other potential sources of pain (e.g., minor trauma, and strained groin muscle) [1516]. Conservative treatments include scrotal elevation, non-steroidal anti-inflammatory drugs, and limited physical activities. Efficacy of conservative treatment for painful varicocele varies in reports. Yaman et al [15] reported that 5/119 (4.2%) men had pain resolution with conservative treatment. However, Chen [16] reported 15/99 (15.2%) men experienced pain relief after 4 weeks of conservative treatment.
Antioxidants, hormonal agents and a few Chinese medicines were used as medical therapy for varicocele-associated male infertility. These agents are potential therapeutic options based on findings reported in preclinical studies, and lack of major side effects; however, there is no study investigating these medications in varicocele-associated testicular pain [17].
Recent data have reported the use of phlebotrophic drugs in patients with varicocele. Micronised purified flavonoid fraction (MPFF) is an oral phlebotrophic drug that improves the venous tone and elasticity and reduces distension of the veins as well as venous emptying time in patients with chronic venous insufficiency. Kiliç et al [18] that 6 months oral MPFF therapy was safe and effective in a study including 16 patients with painful varicocele. However, no recommendation for the use of MPFF can be made until these preliminary results are confirmed by a randomized, placebo-controlled trial.
2. Surgical management
Procedural intervention is indicated for patients with resistance to conservative treatments or persistence of symptoms despite a reasonable period of observation and inability to perform limited activity.
Varicocele ligation commonly known as varicocelectomy is an effective treatment for painful varicocele. Varicocele repair was initially described using a scrotal incision, which however, has lost favor due to the high rate of injury to testicular artery, as well as recurrence [19]. The Scrotal approach had the difficulty of preserving the arterial supply of the testis, because the pampiniform plexus of veins encoils the testicular artery at the level of the scrotum. Various techniques for venous ligation to prevent retrograde flow within the internal spermatic veins have been developed, including retroperitoneal (Palomo), inguinal (Ivanissevich), subinguinal, and scrotal approaches [202122]. Additionally, these techniques have been augmented with laparoscopy, loupe magnification, and operating microscope for enhanced visualization. Each approach carries different degrees of complexity, success rates, complications, and recurrence rates. Palomo technique entails retroperitoneal high ligation of the testicular artery and vein above the internal inguinal ring. The technique facilitates ligation at high level where only 2 to 3 veins are found usually. However, the surgeon cannot assess the collateral veins that branch out of the bundle inferior to the operating field. Therefore, this technique has a higher incidence of recurrence.
The open retroperitoneal approach involves splitting the oblique abdominal musculature to expose the internal spermatic veins at the proximal end of the internal inguinal ring within the retroperitoneum. In this approach, the testicular artery is not usually dissected; however, if located, all efforts must be made to preserve the artery. Loupes or surgical microscope can be useful for this step. In recent studies under magnification, complete and partial pain resolution rates were reported to be 82.8% and 9.3%, respectively [23]. Due to technological advances, a retroperitoneal approach is feasible with laparoscopy, which involves ligation of the spermatic veins near the point of entry into the left renal vein. Laparoscopic method is less invasive compared with the open method and at this level fewer veins need ligation [2425]. Additionally, since the testicular artery is not branched at this level, there is no risk of an injury [26]. Laparoscopic high ligation leads to preservation of the testicular artery and a few lymphatics. However, it is not used frequently because of the need for general anesthesia, the need for an experienced laparoscopic surgeon, the invasiveness, and the higher complication rate. The higher rate of recurrence and hydrocele formation is another concern.
The inguinal approach entails a skin incision over the inguinal canal, superior to the external ring, and incision of the external oblique fascia. The subinguinal approach is performed below the external inguinal ring, to save the oblique fascia. Thus, to identify and preserve the arteries and the lymphatics, both approaches should use a loupe or preferably an operating microscope. Due to fewer veins and fewer, larger arteries present within the cord in the inguinal canal compared with the subinguinal approach, the inguinal approach facilitates safer identification and ligation of the internal spermatic veins. Using the inguinal approach, the surgeon can ligate the collateral veins including the external spermatic veins. However, it is more invasive as it involves musculofascial incision. The advantages of subinguinal approach compared with the inguinal approach is the less postoperative pain, lower risk of complications and lower rates of recurrence due to ligation of the external spermatic and cremasteric veins at this level [27]. However, the disadvantages of subinguinal approach include a larger number of veins requiring ligation than the more proximal approaches, and a greater risk of arterial injury, since the testicular arteries below the external inguinal ring often strongly adhere to the spermatic veins at this location [27]. This risk is minimized with the use of the operating microscope [28]. Inguinal and subinguinal microsurgeries are innovative techniques for the ligation of all the veins except the vasal vein while sparing the testicular artery and lymphatics, resulting in a decreased recurrence rate and complication. The recurrence rate of microsurgical varicocelectomy is reported as low as 1% to 2%, lower than that of open approach [29]. Scrotal hydrocele, the most common complication of varicocelectomy ranges in frequency from 3% to 33%, hardly occurs after microsurgery because lymphatics can be observed and saved easily under a magnified visual field. However, the use of microsurgical repair requires training and expertise, and the duration of surgery is also longer with this method. Studies comparing the inguinal to subinguinal approaches have shown that opening the external oblique aponeurosis during inguinal repair leads to additional pain and longer recovery times but shorter surgical duration [27]. Kim et al [30] operated on 114 patients of painful varicocele using the microsurgical inguinal approach. The overall response rate was 91.2%, with only 8.8% patients reporting pain postoperatively. Park et al [31] used microsurgical inguinal or subinguinal approach and reported complete and partial response in 52.8% and 41.5% of patients, respectively.
Practice considerations among urologists vary widely in the adult and adolescent populations, depending on the surgeon's preference and the hospital condition [32]. Other comparative reports have assessed different techniques, and currently, there is no consensus on the surgical method that is most appropriate for varicocele treatment, although microsurgical techniques have gained popularity with minimal complication rates and satisfactory outcomes (Table 2) [30].
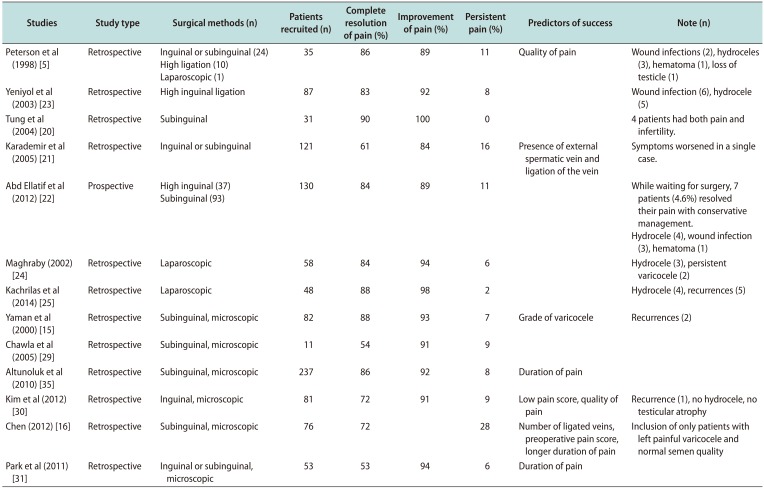
Table 2
Procedural outcomes of varicocele repair for pain
| Studies | Study type | Surgical methods (n) | Patients recruited (n) | Complete resolution of pain (%) | Improvement of pain (%) | Persistent pain (%) | Predictors of success | Note (n) |
|---|---|---|---|---|---|---|---|---|
| Peterson et al (1998) [5] | Retrospective | Inguinal or subinguinal (24) | 35 | 86 | 89 | 11 | Quality of pain | Wound infections (2), hydroceles (3), hematoma (1), loss of testicle (1) |
| High ligation (10) | ||||||||
| Laparoscopic (1) | ||||||||
| Yeniyol et al (2003) [23] | Retrospective | High inguinal ligation | 87 | 83 | 92 | 8 | Wound infection (6), hydrocele (5) | |
| Tung et al (2004) [20] | Retrospective | Subinguinal | 31 | 90 | 100 | 0 | 4 patients had both pain and infertility. | |
| Karademir et al (2005) [21] | Retrospective | Inguinal or subinguinal | 121 | 61 | 84 | 16 | Presence of external spermatic vein and ligation of the vein | Symptoms worsened in a single case. |
| Abd Ellatif et al (2012) [22] | Prospective | High inguinal (37) | 130 | 84 | 89 | 11 | While waiting for surgery, 7 patients (4.6%) resolved their pain with conservative management. | |
| Subinguinal (93) | Hydrocele (4), wound infection (3), hematoma (1) | |||||||
| Maghraby (2002) [24] | Retrospective | Laparoscopic | 58 | 84 | 94 | 6 | Hydrocele (3), persistent varicocele (2) | |
| Kachrilas et al (2014) [25] | Retrospective | Laparoscopic | 48 | 88 | 98 | 2 | Hydrocele (4), recurrences (5) | |
| Yaman et al (2000) [15] | Retrospective | Subinguinal, microscopic | 82 | 88 | 93 | 7 | Grade of varicocele | Recurrences (2) |
| Chawla et al (2005) [29] | Retrospective | Subinguinal, microscopic | 11 | 54 | 91 | 9 | ||
| Altunoluk et al (2010) [35] | Retrospective | Subinguinal, microscopic | 237 | 86 | 92 | 8 | Duration of pain | |
| Kim et al (2012) [30] | Retrospective | Inguinal, microscopic | 81 | 72 | 91 | 9 | Low pain score, quality of pain | Recurrence (1), no hydrocele, no testicular atrophy |
| Chen (2012) [16] | Retrospective | Subinguinal, microscopic | 76 | 72 | 28 | Number of ligated veins, preoperative pain score, longer duration of pain | Inclusion of only patients with left painful varicocele and normal semen quality | |
| Park et al (2011) [31] | Retrospective | Inguinal or subinguinal, microscopic | 53 | 53 | 94 | 6 | Duration of pain |
![]()
3. Percutaneous embolization
Percutaneous transcatheter embolization involves percutaneous vascular access via an antegrade or retrograde approach. A venogram delineates the venous anatomy, following by embolization with coils, balloons or sclerotherapy. The major advantage of this technique is that it can be accomplished under local anesthesia. However, it is usually performed only at centers with expertise in interventional radiology, and has been less successful than surgical treatment due to significant radiation exposure. Therefore, it has not been as effective as the microsurgical approach for primary treatment; however, its role in recurrent and persistent varicocele is better established [33]. Recent data show improved effectiveness of percutaneous transcatheter embolization for the primary treatment for painful varicocele [34]. However, recurrence rates continue to be higher compared with the microsurgical approach.
4. Predictors of success
Grade of varicocele, character of pain, duration of pain, and body mass index (BMI) as well as prior conservative management and the type of surgical method used, are factors correlated with surgical success. However, these preoperative indicators are not ubiquitously reported in the literature because pain is difficult to describe subjectively and accurately, and can lead to incorrect diagnosis and wrong selection for surgery.
1) Grade of varicocele
High grade of varicocele is a predictor of poor outcome. Yaman et al [15] reported outcomes in 82 patients after varicocelectomy: 87.8% (72/82) showed complete response while 11.0% showed no response (9/82). Non-responders with varicocele grade 3 constituted 6.1%, (5/82), grade 2 3.7% (3/82), and grade 1 1.2% (1/82). However, no significant difference was found in the varicocele grade between responders and non-responders in another study [16].
2) Character of pain
Dull pain associated with varicocele is a predictor of good outcome. Kim et al [30] reported that the quality of pain is an independent predictor of success. They reported 100% (24/24) success when pain was dull in nature, although the success rates were 78.4% (29/37) in men with aching pain, and 96.2% with dragging pain (51/53). None of the patients reported sharp pain. Other studies did not find significant correlation between the nature of pain and response to surgery [31].
3) Duration of pain
Patients with longer duration of pain before surgery showed better outcomes. Kim et al [30] reported that the mean duration of pain in the entire cohort and in non-responders was 13.7 months and 4.2 months, respectively. This study did not group the patients according to their duration of pain. Other studies using a cut-off pain duration of 3, 6, and 9 months, found a significant difference in the response rates. Patients with a longer duration of pain before surgery had better outcome [15]. Success rate was 98.6% in the group that reported pain for more than 3 months, while 7.7% with pain duration less than 3 months failed treatment [35].
4) Body mass index
Higher BMI is a factor associated with poor outcomes in painful varicocele. Park et al [31] reported that all failures occurred in patients with BMI >22 kg/m2. However, in another study BMI in responders and non-responders was 21.3 and 22.1 kg/m2, respectively, though the difference was not statistically significant [16].
5. Expert opinion
Various surgical approaches for painful varicocele resulted in similar rates of pain resolution. Therefore, varicocelectomy is accepted as a standard treatment for varicocele with pain. However, about 10% of patients experienced persistent pain following varicocelectomy. Therefore, informed consent before surgical treatment should consider the possibility of non-response. In addition, adequate conservative treatment is indicated before surgical treatment because several studies reported that long-term duration of pain is a predictor of successful outcome postoperatively. Among various surgical approaches, microsurgical inguinal or subinguinal approaches are recommended because of low recurrence rates and fewer complications such as hydrocele. In the hands of an experienced surgeon, microsurgical subinguinal approach reduces pain by saving the external oblique aponeurosis and facilitating ligation of gubernacular collateral veins.
Go to :
CONCLUSIONS
Chronic testicular pain is a common complaint, affecting up to 2% to 10% of patients with varicocele. Varicocelectomy is still the most preferred treatment option and is associated with approximately 80% success for amelioration of pain. However, various surgical methods including retroperitoneal, inguinal, subinguinal and scrotal approaches with or without laparoscopic, microscopic assistance are available.
Microsurgical techniques of varicocelectomy have gained popularity with minimal complication rates and favorable outcomes. Grade of varicocele, character of pain, duration of pain, BMI, prior conservative management, and the type of surgical approach are predictors of success in varicocelectomy. Nevertheless, continued investigation and randomized studies with longer follow-ups are necessary.
Go to :
 XML Download
XML Download