

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obstructive sleep apnea (OSA) is a relatively common chronic sleep disorder characterized by repeated episodes of complete or partial upper airway obstruction during sleep, resulting in oxygen desaturation, sleep fragmentation, and daytime sleepiness [1]. Population-based studies suggest that 2% of women and 4% of men over the age of 50 years have symptomatic OSA [2]. A number of negative health effects have been attributed to untreated OSA including increased rates of mortality, cardiovascular disease, and neurocognitive difficulties. Untreated OSA has been demonstrated to be an independent risk factor for cardiovascular morbidity including hypertension, coronary heart disease, congestive heart failure, arrhythmias, pulmonary hypertension, stroke, sudden death, insulin resistance, and gastroesophageal reflux disease [234].
OSA has also been associated with altered pituitary-gonadal function and sexual dysfunction, manifested primarily as erectile dysfunction (ED) and decreased libido [5]. Testosterone, the primary androgenic hormone in males, is stimulated through pulsatile secretion of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) [6]. The amount of testosterone synthesized is regulated by the hypothalamic-pituitary-testicular axis [67]. Serum testosterone has been shown to be lower in men with OSA and treatment of OSA may help improve hypogonadism and sexual function [789]. This article reviews recent investigations on the relationship between OSA and testosterone deficiency.
Go to : 
NORMAL SLEEP AND TESTOSTERONE
Normal sleep is basically divided into non-rapid eye movement (NREM) and rapid eye movement (REM) sleep [10]. NREM sleep accounts for 75% to 80% of total sleep time, and REM sleep accounts for the remaining 20% to 25% [11]. These two categories of sleep have a 90 minutes cycle, and normal adults repeat this cycle four to six times during the night. The cycle becomes longer and more frequent over the course of sleep. NREM sleep can be divided into three stages depending on the depth of sleep; the first two stages (stage 1 and 2) are characterized by brief waking episodes, and are shallow. The last and deeper stage of NREM sleep (stage 3) occurs predominantly during the early stage of the sleep cycle and becomes shorter thereafter [1011]. REM sleep appears behind NREM sleep and is predominant in the late stage of the sleep cycle. The first REM sleep appears 80 to 100 minutes after the start of sleep, and the time between the first REM sleep and sleep onset is termed the REM latency [1011]. Sleep architecture changes naturally with aging so that the relative amount of stage 1 and 2 of NREM sleep increases and that of stage 3 decreases, especially in men [12]. Furthermore, the frequency of awakening and REM latency also increase during sleep with aging [1213].
The endogenous rhythm of testosterone production is similar to that of cortisol [14]. Serum testosterone levels vary in a circadian manner, being higher during waking hours and the decreasing to a low level at the end of the day [15]. Testosterone levels begin to rise upon falling asleep, peak at about the time of the first episode of REM sleep, and remain at the same level until awakening [16]. A previous study demonstrated that the sleep-related increase in serum testosterone levels is linked with the appearance of the first REM sleep episode after about 90 minutes, and the REM latency [17]. The increase in testosterone level is slower when the REM latency is longer [17]. Although mean nocturnal testosterone levels are not correlated with the number of REM episodes [16], sleep fragmentation disrupts the testosterone rhythm, with considerable attenuation of the nocturnal increase in testosterone [17]. The increase in testosterone at the time of sleep, the decrease during the time of awakening, is stable within an individual, although there is large variability among individuals [18]. Aging is an important factor associated with the morning testosterone level. Generally, middle-aged men have lower morning testosterone levels than healthy younger men, due to a decline in nocturnal testosterone secretion and the amount of nighttime sleep in older men [1920].
Go to :
OBSTRUCTIVE SLEEP APNEA AND LOW TESTOSTERONE
Several studies have confirmed a strong relationship between OSA and low testosterone. Testosterone is associated with pituitary-gonadal function, and OSA is a direct cause of decreased pituitary gonadal function [21]. Both the quantity and quality of sleep affect testosterone levels. Patients with OSA have less REM sleep, reduced deep sleep time, increased nighttime awakenings, sleep fragmentation, and reduced sleep efficiency, which leads to a low testosterone level [6]. Furthermore, several factors, including the apnea-hypopnea index (AHI), the oxygen desaturation index (ODI), nadir oxygen saturation, obesity, and advanced age are associated with the lower testosterone secretions of middle-aged men with OSA [22].
The severity of OSA is classified according to the AHI value and the lowest oxygen saturation value. A normal AHI is defined as ≤5, and OSA can be classified as mild (AHI, 5–15), moderate (AHI, 15–30), or severe (AHI, >30) [23]. A negative correlation has been observed between OSA severity and testosterone level; a higher AHI score correlates with a lower testosterone level, suggesting that the severity of apnea is related to decreased testosterone secretions in patients with OSA [2425]. Furthermore, the severity of hypoxia during sleep, as indexed by the ODI and O2 nadir, is strongly correlated with the reduction in testosterone [8]. However, this concept remains controversial; lower testosterone levels have been found not only in patients with mild OSA, but also in elderly obese patients with severe AHI [26].
Obesity is common among patients with OSA, and is associated with increased severity of the disorder. Therefore, body mass index (BMI) may be the primary determinant of testosterone levels in men with OSA [27]. Obesity is strongly linked to low testosterone levels in men, as is increased fat mass, especially abdominal fat. This may be because adipose tissue, especially when inflamed and in an insulin-resistant state, expresses aromatase, which converts testosterone to 17β-estradiol [28]. Furthermore, obesity reduces the levels of sex hormone-binding globulin (SHBG), which carries testosterone in the bloodstream, due to obesity-associated hyperinsulinemia [2930]. Although obesity leads to a lower testosterone level, low testosterone may also promote obesity [31]. A bidirectional relationship between obesity and low testosterone underpins this association, as indicated by the hypogonadal-obesity cycle and weight loss leading to increased testosterone levels (Fig. 1).
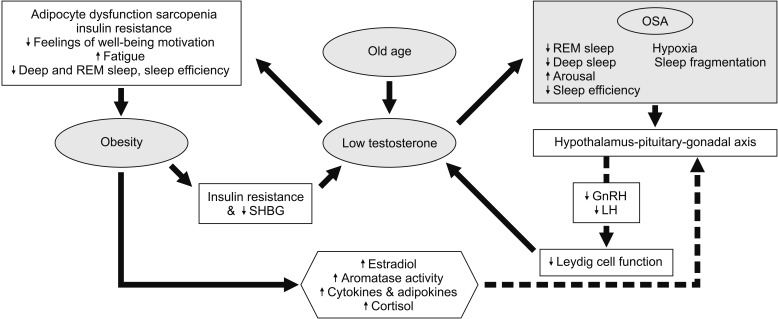 | Fig. 1Potential mechanisms linking obstructive sleep apnea (OSA) and obesity to low testosterone. A bidirectional relationship between testosterone and obesity or OSA is shown. While OSA and obesity lead to lower testosterone, low testosterone promotes obesity and affects sleep quality. REM: rapid eye movement, SHBG: sex hormone binding globulin, GnRH: Gonadotropin-releasing hormone, LH: luteinizing hormone.
|
Go to :
EFFECT OF LOW TESTOSTERONE ON SLEEP QUALITY AND FATIGUE
While the quantity and quality of sleep lead to reduced testosterone levels, there is also evidence to suggest the reverse. In a cohort study of men aged ≥65 years, those with low testosterone levels experienced decreased sleep efficiency, increased frequency of nighttime awakenings, and reduced deep sleep time [32]. A mouse study showed that loss of testosterone after gonadectomy results in a significant decrease in the amount of deep sleep, which can be treated by testosterone replacement therapy (TRT) [33].
In addition to lower serum testosterone, patients with severe OSA also have higher levels of general fatigue, physical fatigue and mental fatigue, and reduced physical activity. Nadir oxygen saturation is not a significant predictor of fatigue, but a multivariate analysis revealed that testosterone level was the only independent predictor of physical fatigue and reduced activity in patients with OSA [7].
Go to :
EFFECT OF OBSTRUCTIVE SLEEP APNEA TREATMENT ON TESTOSTERONE
The effects of OSA treatment on testosterone levels are controversial. A prospective controlled study of uvulopalatopharyngoplasty therapy for OSA showed increased testosterone levels, and improved libido and sexual function, at 3 months post-surgery without significant changes in BMI, serum prolactin, LH, or FSH [34]. Another longitudinal study, of 43 men with severe OSA treated with continuous positive airway pressure (CPAP) therapy, showed a significant increase in total testosterone and SHBG at 3 months after treatment [35]. Although these studies suggest that OSA treatment by CPAP or surgery increases morning plasma testosterone levels within 3 months, the majority of other studies show that CPAP therapy for 1 to 39 months does not affect LH, FSH, or testosterone [36373839]. Unlike the effects of CPAP, there is a linear relationship between weight loss and increased plasma testosterone in obese men [40].
Go to :
EFFECT OF EXOGENOUS TESTOSTERONE ON OBSTRUCTIVE SLEEP APNEA
Although its effect on OSA remains unclear, exogenous testosterone has been considered to have a noxious effect on OSA. Despite a lack of convincing evidence that TRT aggravates OSA, in current guidelines TRT is contraindicated in the presence of untreated OSA [41]. Although low testosterone may affect overall sleep quality, which is improved by replacement doses, large doses of exogenous testosterone are associated with abnormalities in sleep duration and architecture. Several studies have shown that TRT exacerbates OSA symptoms, the increase in the AHI, and the decrease in oxygen saturation [424344454647]. The effect of testosterone on OSA is not exerted by changing the dimensions of the upper airway; instead, testosterone most likely contributes to OSA via central mechanisms.
There are a variety of possible physiological mechanisms by which TRT exacerbates OSA, including morphological and neuromuscular changes to the airway, changes in metabolic requirements, and changes in physiological responses to hypoxemia and hypercapnia. Dilatation of the upper airway depends on contraction of the airway dilator muscles (e.g., the genioglossus), an effect mediated by parallel serotoninergic and noradrenergic neurons; both types of neuron may be impacted by age and testosterone level [2248]. Alternative explanations include the possibility of higher metabolic requirements with elevated testosterone levels, which may result in greater oxygen consumption that in turn could lead to hypoxia [41]. Other plausible explanations include a role for testosterone in the neural response pathways to hypoxia and hypercapnia [49]. Fluctuating testosterone levels may also impact on the ventilatory response to hypoxia and hypercapnia, which could explain the higher rates of OSA seen in men on TRT [4750] (Fig. 2).
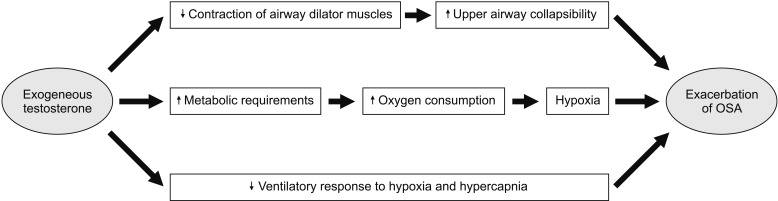 | Fig. 2The plausible mechanisms by which testosterone replacement therapy (TRT) worsens obstructive sleep apnea (OSA). TRT aggravates OSA by several physiologic mechanisms including neuromuscular changes to the airways, changes in metabolic requirements, and changes in the physiologic response to hypoxia and hypercapnia.
|
Development of the signs and symptoms of OSA during TRT requires assessment by polysomnography and, potentially, treatment with CPAP. If the patient is unresponsive or cannot tolerate CPAP, the testosterone dose must be reduced or discontinued. Furthermore, OSA has been proposed to be a risk factor for secondary polycythemia [51] and TRT exacerbates polycythemia in some patients [52]. This should be kept in mind in patients with OSA and hypogonadism who are considering TRT.
Go to :
OBSTRUCTIVE SLEEP APNEA AND SEXUAL DYSFUNCTION
The men with OSA are also more prone to suffering from associated complications like low libido, impotence, and ED. Severe OSA was clearly associated with ED, although this relationship was very weak in patients with mild or moderate OSA [53]. A recent meta-analysis reported that the relative risk of ED in OSA patients was 1.82 [54]. Although the effects of OSA treatment on testosterone levels remain unclear, there are more positive data for the improvement in sexual dysfunction with OSA treatment regardless of testosterone level. CPAP resolved ED in 75% of OSA patients, resulting in significant improvement in quality of life [55]. A pilot study showed that positive additive effects of TRT to phosphodiesterase type 5 inhibitors in hypogonadal men with OSA receiving CPAP therapy. However, it is not yet clear whether similar benefits can be achieved with CPAP alone without TRT, which should be confirmed in larger controlled studies.
Go to :
CONCLUSIONS
Testosterone shows circadian variation, but its pattern is not as same as cortisol. Sleep-related increase in serum testosterone is linked with the appearance of first REM sleep and requires 3 hours of deep sleep. Although the relationship between testosterone and OSA are complex and not yet completely understood, OSA may contribute to low testosterone because hypoxia and sleep fragmentation. Furthermore, obesity and advanced age may account for lower testosterone secretion levels in middle-aged men with OSA. Although the effects of OSA treatment on testosterone levels remain unclear, OSA treatment may help improve sexual function, especially in men with severe OSA. However, TRT should be probably avoided in patients with severe untreated OSA because TRT may worsen OSA in some patients.
Go to :
 XML Download
XML Download