

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
External beam radiotherapy (EBRT) is one of the main treatments for cervical cancer. Overall, approximately 80% of patients with cervical cancer have received EBRT. Sixty percent of the patients with radiotherapy (RT) failure were pelvic recurrence and 80% of them relapsed within two years after treatment [1]. The treatment for pelvic recurrent cervical cancer (PRCC) after EBRT has always been a challenging problem, without widely accepted treatment recommendations. Due to the dose limitation for normal tissue, it is difficult to deliver enough doses to recurrent lesion through pelvic re-irradiation. Encouragingly, radioactive 125I seed (RIS) implantation, which is a standard treatment for early low-risk prostate cancer, could overcome this problem. RIS is characterized by extremely high dose to tumor while sparing normal tissue. Accumulating evidence showed its good efficacy in various recurrent cancers, including rectal cancer, head and neck cancer, and pancreatic cancer [2345]. Our previous work, showed its encouraging efficacy as a salvage or palliative pain relief treatment for recurrent rectal cancer after multiple therapies [6]. Moreover, our previous work has been referenced by National Comprehensive Cancer Network (NCCN) as a recommended strategy for locally recurrent rectal cancer [7]. In this study, we analyzed the clinical efficacy of RIS on PRCC after EBRT, and further investigated the influence of dosimetric parameters on the efficacy, in order to give advises to treatment.
MATERIALS AND METHODS
1. Data collection
This retrospective study enrolled totally 36 patients from July 2005 to October 2015 in our hospital with approval by the Institutional Review Boards (IRB00006761-M2018195). The inclusion criteria: patients were pathologically or radiologically confirmed to be PRCC; the tumors were unresectable due to individual rejection or surgeon consultation; all of the patients were received image-guided radioactive 125I seed (IGRIS) implantation; the recurrent sites with IGRIS implantation were previously irradiated.
2. Procedure
Patients underwent pelvic enhanced computed tomography (CT) 1 week before implantation with 5 mm slice thickness. Then the image data was transmitted to Treatment Planning System (TPS; Beijing Feitian Industries Inc. and Beijing University of Aeronautics and Astronautics, Beijing, China) for preoperative plan. We gave the prescribed dose to gross tumor volume (GTV) and set the activity of 125I seeds. Then the number and distribution of seeds were determined and dose was calculated according to the TPS. All patients received intravertebral anesthesia or local infiltration anesthesia. We chose puncture point according to the preoperative plan and performed puncture guided by CT scan. Some patients, with vaginal stump recurrence, were punctured under guidance of real-time transvaginal or transrectal ultrasound. The implantation needles were placed 0.5–1.0 cm apart. RIS (CIAE-6711; Chinese Atomic Energy Science Institution, Beijing, China) was 0.8 mm × 4.5 mm, masked by nickel-titanium alloy. Seeds were implanted by Mick applicator (Mick Radio-Nuclear Instruments Inc., Mount Vernon, NY, USA) at a distance of 0.5–1.0 cm from each other. Finally, we ensured the distribution of seeds by ultrasound or CT scan, if not, we supplemented seeds. Patients whose seeds were implanted under ultrasound-guide received CT scan within 24 hours. The CT images transfer to TPS for postoperative plan (Fig. 1). All patients were discharged in 3 days or longer. All physicians who did this procedure were well trained and legally qualified and always wore lead clothes and gloves. All procedures abided by the criteria recommended by the International Commission on Radiological Protection [8].
3. Dosimetric parameters collection
In order to verify the treatment plan after implantation, we collected the dosimetric parameters of 33 patients who had postoperative CT image, including dose delivered to 90% (D90) and 100% (D100) of GTV, percentage of GTV receiving 100% (V100), 150% (V150) and 200% (V200) of the prescription dose, target area external index (EI), conformal index, and homogeneity index (HI). The volume exceeding the prescribed dose outside GTV was described by EI. The greater the value of the EI was, the greater the prescribed dose received outside GTV. The conformity of the dose distribution was evaluated by conformal index. The best conformal index was 1, which means GTV was just covered by the prescribed dose and the dose outside GTV was lower than the prescribed dose. HI was used to evaluate the uniformity of dose distribution. The closer to 100% the HI was, the more uniform dose distribution of GTV.
4. Evaluation criteria of clinical efficacy and side effect
Local tumor response was evaluated after one month from seed implantation according to the criteria of Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Numerical rating scale (NRS) was used to assess pain on 5 levels: 0 for no pain, 1 to 3 for mild pain, 4 to 6 for moderate pain, 7 to 9 for severe pain, and 10 for sharp pain. It was considered effective when the pain level was declined, after implantation. Side effect was evaluated according to the Radiation Therapy Oncology Group (RTOG) and European Organization for Research and Treatment of Cancer (EORTC) criteria [9].
5. Statistical analysis
SPSS version 21.0 (SPSS, Chicago, IL, USA) was used to perform all statistical analysis. Kaplan-Meier survival analysis was used to estimate local progression free survival (LPFS) and overall survival (OS). The comparisons between groups were performed by log-rank test. We analyzed the confounding factors that affected LPFS and OS using Cox proportional hazards regression model. The factors included in the multivariate analysis were eliminated the existence of multi-collinearity. We considered p value <0.05 as a significant difference.
RESULTS
1. General characteristic of patients
Until January 2017, 3 patients were lost to follow-up, 31 patients died, and 2 patients were still alive. Median follow-up was 11.5 (2–30) months.
The median age was 44 years (30–79 years). KPS score was ≥60. The median volume of lesion was 59.2 mL (2.5–116.5 mL). Among the patients, 15 (41.67%) cases were pelvic central recurrence and 21 (58.33%) cases were pelvic wall recurrence. All patients received pelvic EBRT, including radical RT (10/36, 27.8%) and postoperative adjuvant RT (26/36, 72.2%). Five (13.88%) patients received re-RT. The median cumulative RT dose at implantation site (equivalent dose in 2 Gy/f; EQD2) was 56 Gy (42–107 Gy) (Table 1). Thirty-two cases were guided by CT and 4 cases were guided by ultrasound. The median activity of 125I seeds was 0.7 mCi (0.5–0.8 mCi) (1 mCi=3.7×1010 Bq). The median of total numbers of seeds for 1 patient was 62.5 (10–140).
Table 1
General information

FIGO, International Federation of Gynecology and Obstetrics; EQD2, equivalent dose in 2 Gy/f; RT, radiotherapy; RIS, radioactive 125I seed; PFS, progress-free survival.
![]()
2. Local control
Among 36 patients, 19 (52.7%) achieved partial response. Thirteen (36.1%) patients showed stable disease and progressive disease in 4 (11.2%) patients. The local control rate was 88.9% (32/36). The LPFS rate was 34.9% for 1 year, 20% for 2 years, respectively. Median LPFS time was 7.5 (2–21) months. The progression-free survival (PFS) time of previous therapy of 4 patients with progressive disease was no longer than 12 months. All of them had central pelvic recurrence and received multi-courses therapy. Moreover, we performed univariate analysis for recurrent sites, pathological type, image-guided approach, PFS, previous RT dose, tumor volume and GTV D90. The results showed that recurrent sites (hazard ratio [HR]=0.413; 95% confidence interval [CI]=0.181–0.944), tumor volume (HR=1.012; 95% CI=1.00–1.024), and GTV D90 (HR=0.988; 95% CI=0.978–0.999) were significantly related with LPFS (all p<0.05). In terms of recurrent sites, 15 (41.67%) patients had recurrence at central pelvic cavity and 21 (58.33%) at pelvic wall. The median LPFS for those 2 groups were 6 and 12 months, respectively, and 1-year LPFS rates were 26.7% and 41.6% (χ2=5.195; p=0.023), respectively (Fig. 2A). According to receiver operating characteristic (ROC) curve, we divided the patients into 2 groups by tumor volume at 64 mL. The tumor volume of 19 (52.8%) patients was <64 mL, and that of 17 (47.2%) patients was ≥64 mL. Median LPFS of these 2 groups were 12 and 6 months, respectively, and 1-year LPFS rates were 48.2% and 20.6%, respectively (χ2=4.302; p=0.038) (Fig. 2B). Moreover, we divided the patients into 2 groups by GTV D90 at 105 Gy. GTV D90 of 12 (33.3%) patients was <105 Gy and that of 24 (66.7%) patients was ≥105 Gy. Median LPFS of these 2 groups were 6 and 13 months, respectively, and 1-year LPFS rates were 0% and 53.5%, respectively (χ2=9.145; p=0.002). And we performed a multivariate analysis for the 3 factors above, which suggested that recurrent sites (HR=0.294; 95% CI=0.121–0.718, p=0.007), the lesion volume (HR=2.898; 95% CI=1.139–7.372; p=0.026), and GTV D90 (HR=0.332; 95% CI=0.130–0.850; p=0.022) were the independent factors influencing LPFS (p<0.05 for all 3 factors).

3. Causes of death and survival
Thirty-one patients died during the follow-up period; 10 (32.26%) patients died of local progression, 12 (38.71%) patients died of metastases, and 9 (29.03%) patients died of non-tumor causes. Median OS was 11.5 (2–30) months. The 1- and 2-year OS rates were 52.0% and 19.6%, respectively. Recurrent sites, pathological type, surgery, chemotherapy, PFS after previous therapy, tumor volume, and GTV D90 were enrolled into univariate analysis, which indicated that only pathological type (HR=4.616; 95% CI=.290–16.515; p=0.019) was related with LPFS. Median OS of squamous carcinoma and adenocarcinoma were 13 and 4 months, respectively. One-year OS rate of these 2 pathological types were 57.5% and 0%, respectively (χ2=7.195; p=0.007). Moreover, recurrent sites, pathological type, tumor volume, and D90 were enrolled into multivariate analysis, which suggested that pathological type (HR=9.713; 95% CI=2.136–44.176; p=0.003) and recurrent sites (HR=0.358; 95% CI=0.136–0.940; p=0.037) were the independent factors influencing OS. For recurrent sites, median OS of pelvic central recurrence and pelvic wall were 8 and 13 months, respectively. One-year OS rate of the 2 groups were 49.5% and 54.7% (χ2=2.535; p=0.111). Median OS of 2 groups divided by tumor volume were 17 (<64 mL) and 12 months (≥64 mL). One-year OS rate of these 2 groups were 65.3% and 38.2% (χ2=0.625; p=0.429), respectively. For the 2 groups divided by D90, median OS were 12 (<105 Gy) and 14 months (≥105 Gy), respectively. One-year OS rate of those 2 groups were 0% and 65.1% (χ2=0.013; p=0.909), respectively.
4. Dosimetric factors
We considered LPFS and OS as the index representing clinical efficacy and we analyzed the influence of different dosimetric parameters on these 2 indices, including D90, D100, V100, V150, V200, EI, conformal index, and HI of GTV. Thirty-three patients got complete dosimetric data enrolled this part: GTV D90, 128.5±47.4 Gy; D100, 50.4±23.7 Gy; V100, 86.7%±12.9%; V150, 67.4%±17.4%; V200, 49.2%±18.6%; EI, 62.8%±42.9%; conformal index, 0.53±0.44; and HI, 23.0%±12.2%.
In terms of LPFS, the results of univariate analysis suggested that D100 was significantly related with LPFS (Table 2). The p value of D90 and V100 were near 0.05, but there was no statistic difference. According to ROC curve, we divided the patients into 2 groups by D100 at 105 Gy. D100 of 20 (60.6%) patients were <55 Gy and 13 (39.4%) were ≥55 Gy. Median LPFS were 6 months in <55 Gy group versus 13 months in ≥55 Gy group. One-year LPFS rates were 15.8% in <55 Gy group versus 49.2% in ≥55 Gy group (χ2=8.671; p=0.003) (Fig. 3A). Likewise, we divided the patients into 2 groups by D90 and V100 at 105 Gy, 91%, respectively. For D90, that of 11 (33.3%) patients was <105 Gy and 22 (66.7%) were ≥105 Gy. Median LPFS were 6 months in <105 Gy group versus 13 months in ≥105 Gy group. One-year LPFS rate was 0% in <105 Gy group versus 53.3% in ≥105 Gy group (χ2=8.180, p=0.004) (Fig. 3B). For V100, that of 15 (45.5%) patients were <91% and 18 (54.5%) were ≥91%. Median LPFS were 8 months in <91% group versus 18 months in ≥91% group. One-year LPFS rate was 15.6% in <91% group versus 55.0% in ≥91% group (χ2=8.671; p=0.003) (Fig. 3B). Then these 3 dosimetric parameters with no multi-collinearity were brought into the multivariate analysis. The result showed D100 was the major factor influencing LPFS (p<0.05) (Table 3).
Table 2
Cox univariate analysis of dosimetric parameters influencing LPFS
LPFS, local progression-free survival; HR, hazard ratio; CI, confidence interval; D90, D100, dose delivered to 90% or 100% of the volume; V100,V150,V200, percentage of the volume receiving 100%, 150%, 200% of the prescription dose; EI, external index; HI, homogeneity index.
![]()
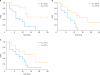 | Fig. 3LPFS rate of different dosimetric parameters. (A) LPFS rate of different GTV D100. (B) LPFS rate of different GTV D90. (C) LPFS rate of different GTV V100.LPFS, local progression-free survival; GTV, gross tumor volume; D90, D100, dose delivered to 90% or 100% of the volume; V100, percentage of the volume receiving 100% of the prescription dose.
|
Table 3
Cox multivariate analysis of dosimetric parameters influencing LPFS

| Parameters | HR | 95%CI | p |
|---|---|---|---|
| D90 (<105 Gy, ≥105 Gy) | 1.079 | 0.186–6.248 | 0.932 |
| D100 (<55 Gy, ≥55 Gy) | 0.207 | 0.052–0.824 | 0.025 |
| V100 (<91%, ≥91%) | 0.351 | 0.068–1.811 | 0.211 |
LPFS, local progression-free survival; D90, D100, dose delivered to 90% or 100% of the volume; V100, percentage of the volume receiving 100% of the prescription dose; HR, hazard ratio; CI, confidence interval.
![]()
However, for OS, the results of univariate analysis suggested that no significant differences were shown among these different dosimetric parameters.
5. Pain control
Before seed implantation, 24 patients had pain leading from tumor. Five (20.8%) patients got severe pain. Fifteen (62.5%) patients got moderate pain. Four (16.7%) patients got mild pain. After that, the pain of 19 (79.2%) patients downgraded.
6. Side effect
For puncture-related reaction, 2 (5.56%) patients had transient aggravated pain, which might be resulted from local tissue swelling after puncture. Three (8.33%) patients had fever after implantation. One patient suffered from needle tract metastases. After seeds implantation, 5 (13.89%) patients, who were central recurrence, encountered seeds dropping via vagina. For radiation-related adverse effects, 3 (8.33%) patients got grade 1 or 2 proctitis. Two (5.56%) patients had grade 1 urinary system reaction. Additionally, only 1 patient had vaginal fistula which was considered as radiation injury.
DISCUSSION
The 5-year survival rate was only 3.2%–13% for patients with recurrence after radical surgery or RT [1011]. The treatment for PRCC after RT includes three main methods: surgery, re-RT and chemotherapy. Patients, who had pelvic central recurrence after RT, with no pelvic wall invasion and no distant metastasis, were suitable for pelvic exenteration. Five-year OS rate is about 20%–60%. However, the challenging difficulty of operation and high incidence of postoperative complication limits this surgical method [12]. On the other hand, for patients with pelvic wall recurrence after RT, laterally extended endopelvic resection with or without intraoperative RT could be a choice. But severe intestinal and neurological side effects might occur on 25%–30% of patients or so [12]. The chemotherapy for patients with recurrence, metastasis and continued progress was based on cis-platinum. The combination of other drugs with cis-platinum increased the response rate to 36% and prolonged the PFS to 4.8 months, with no significant change on OS [1314]. Some reports suggested that conventional drug therapy combined with bevacizumab significantly extended the OS to 17 months [15].
In recent years, with the progress of RT technology, re-irradiation has achieved encouraging effects on recurrent cervical cancer after RT. Intensity modulated radiation therapy is highly conformal RT technique, but is still superseded by the stereotactic techniques and brachytherapy, and one must consider these options when considering re-irradiation [16]. The use of stereotactic body radiotherapy (SBRT) in the treatment of recurrent cervical cancer in pelvic irradiation field was limited to some studies with small samples, we should do further studies to confirm indications and dose. Proton therapy, for Bragg peak, is maybe one of the salvage treatment options for PRCC. But the clinical outcomes data of proton re-irradiation are too sparse [17]. High-dose-rate brachytherapy is the most widely used RT techniques in recurrent cervical cancer currently, but it is mostly used for central pelvic recurrence.
Radioactive seeds, as a way of continuous low-dose-rate RT, have close effective radiation range. It has been applied into the treatment of various solid tumor, due to its optimal dose distribution, minimal invasion and repeatability [46181920]. However, few clinical investigations reported its application in recurrent cervical cancer. A retrospective analysis reported the efficacy of radioactive 198Au seeds implantation on 15 patients with central pelvic recurrent uterine carcinoma [21]. The result showed that median follow-up time was 19 months, 2-year local control rate was 33% and 2-years OS was 64%. They concluded that permanent interstitial implantation with radioactive 198Au seeds was a feasible strategy for patients with recurrent gynecologic tumor, with a better efficacy for tumor volume <2 cm3 within vaginal wall or stump. Wang et al. [22] reported a study enrolling 15 patients with recurrent cervical cancer after RT who received RIS implantation. During the follow-up period (4–32 months), no patients had radiation injury or other complications. Six-month, 1-year, and 2-year local control rate were 64.1%, 29.4% and 14.7%, respectively. Median local control time was 6 months. Median survival was 12 months. However, in our study, 1-year LPFS rate was 34.9% and median LPFS time was 7.5 months. One-year OS rate was 52% and median OS time was 11.5 months. It is worth mentioning that the patients with tumor volume <64 mL had longer LPFS. In our study, all the patients had received RT or chemotherapy after recurrence and surgery was unavailable or unaccepted. The prognosis must be worse than the previous literatures.
We divided the patients into two groups by recurrent site. The result showed that LPFS of RIS implantation on pelvic wall recurrence was significantly better than central recurrence. The survival time of pelvic wall recurrence was slightly longer than central recurrence, though with no significant difference in statistics which maybe related to nonlarge sample size. But the multivariate analysis confirmed recurrent site was the independent factor both for LPFS and OS. Thus, compared with central recurrence, the efficacy and prognosis of RIS implantation were better than patients with pelvic wall recurrent cervical cancer. Furthermore, we analyzed potential causes resulted in this difference. First, for central recurrence, the vaginal wall was too thin to implant and keep the seeds. The implanted seeds were more likely to drop from vagina, which gave rise to local dose reduction. Second, the lesion relapsed in central pelvic cavity was prone to extend along vaginal wall, which brought the difficulty to define the tumor margin and cover the subclinical lesion. All above reasons suggested that RIS implantation was more suitable for pelvic wall recurrence, while patients with central recurrence might choose surgery or high-dose-rate brachytherapy.
RIS implantation is a way of brachytherapy, so the dose is basic. At present, there is no definite cure dose of 125I seed for other tumors excepted prostate cancer. Our previous work on RIS treating rectal cancer suggested that D90 and V100 might be considered as dosimetric predictors for clinical efficacy [2]. The patients of D90 >140 Gy group and V100 >90% had better local control time and OS time. The dose for cervical cancer was referred to prostate cancer, though different biological effect. In this work, we were the first one to analyze the impact of dosimetric parameters on clinical efficacy. Our data indicated that RIS implantation might bring a better local control when D90 ≥105 Gy or D100 ≥55 Gy or V100 ≥91%. D100, the independent dosimetric factor influencing LPFS, played a decisive role.
For patients with PRCC, RIS implantation could improve the quality of life by relieving pain and improving short-time effects. RIS implantation also has the advantages of short time, minimal invasion and less adverse. However, there are some problems in this study remaining to be further investigated. First, LPFS was short, maybe due to inadequate dose around tumor boundary, as uncertainty of target boundary and fast drop off of dose of 125I. Second, large volume of recurrent tumor or low dose of target will result in short LPFS time. Third, the enrolled patients were refractory patients after multiple therapies and had poorer prognosis. Finally, small sample size, short follow-up time and confounding factors might mask the results.
In conclusion, permanent RIS implantation could be a safe, feasible and minimal invasive strategy of re-irradiation for PRCC. It could improve the life quality of patients by pain relief and normal tissue protection. Compared with central recurrence, it is more suitable for patients with pelvic wall recurrent cervical cancer after RT. In line with previous reports, the tumor volume, dose and recurrent sites might influence the effect [212324]. Encouragingly, with the improvement of technology, we were the first brachytherapy center to incorporate 3-dimensional printing template into RIS implantation, in order to increase the accuracy of treatment [252627]. Furthermore, the combination with multiple modern image technologies helped us to define the tumor margin more precisely, which might overcome the problems of target area delineation and dose coverage. In the near future, RIS implantation would achieve better efficacy in patients with recurrent cervical cancer after multiple therapy, and we should do studies of multicenter, large sample and long-term follow-up to verify the results.
 XML Download
XML Download