

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Craniometaphyseal dysplasia (CMD) is a rare hereditary bone disorder.1 It is confirmed through a genetic analysis, and is characterized by hyperostosis of the craniofacial bones and flared metaphyses of the long bones.2 Hyperostotic bone formation leads to protrusion of the frontal and paranasal regions, hypertelorism, a flat nasal bridge, and obliteration of the paranasal sinus and the mastoid.34 Bony compression of cranial nerves caused by hyperostosis of the cranial base results in symptoms such as blindness, deafness, and facial paralysis.5
Although some reports have described the dentomaxillofacial characteristics of CMD, such as increased density of the jaw, malocclusion, prolonged retention of deciduous teeth, and delayed eruption of the permanent teeth,67 only a few studies have reported the distinct imaging features of CMD on panoramic radiography. Hayashibara et al.7 reported a markedly increased radiopacity of the maxillary and mandibular bones on panoramic radiography, due to hyperostosis and sclerosis of the jaw. Lamazza et al.8 reported anomalies of the developing permanent dentition.
CMD occurs in an autosomal dominant and an autosomal recessive form. Sclerosis of cranial bones is usually much more severe in the autosomal recessive form.8 Craniometaphyseal dysplasia is more often inherited in an autosomal dominant pattern.7
The aim of this report was to further report the imaging features of CMD on panoramic radiography.
Case Report
The images of 2 CMD patients referred to our dental hospital were investigated retrospectively.
Case 1
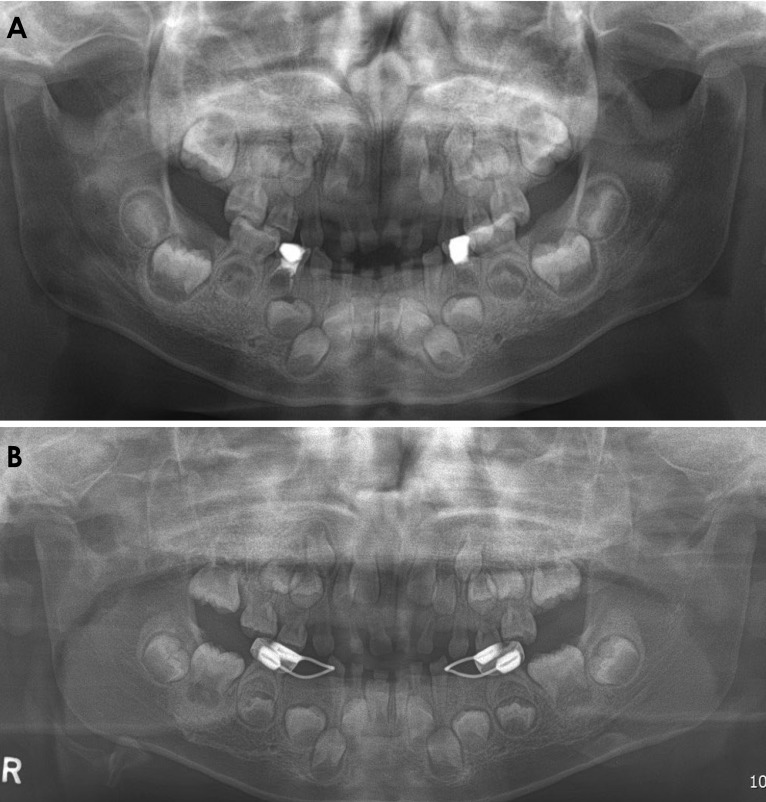
A 5-year-old female patient was referred to the Department of Pediatric Dentistry for an evaluation of facial bone overgrowth and malocclusion. The patient had been diagnosed with autosomal dominant CMD through a genetic analysis in another hospital. Clinically, she showed anterior open bite and generalized spacing. She presented with a small nose, a wide and thickened bony nasal bridge, and prominent zygomatic arches. Panoramic radiography was performed to evaluate facial bone overgrowth and tooth germ development (Fig. 1A). The image revealed that the patient had hyperostosis and sclerosis of the alveolar bone of the maxilla and mandible, especially around the developing tooth germs. There was no definite sclerosis at the basal bone of the mandible, while the maxilla appeared to exhibit severe hyperostosis with maxillary sinus obliteration. The development of the permanent teeth was within normal limits. The shape of the condyle was stubby, while the coronoid process showed slight hyperplasia. The antegonial notch was less developed than was age-appropriate.
Two years later, the patient revisited the Department of Pediatric Dentistry complaining of delayed eruption. A panoramic radiograph was obtained, and revealed delayed development of both maxillary second molars (Fig. 1B). Compared with previous radiographic images, sclerosis around the erupting teeth (such as the mandibular first and second molar) had increased, but sclerosis had decreased around the mandibular premolars, and the border of the bony crypts could be distinguished clearly. There was no detectable change in the shape of the condyle or the underdeveloped antegonial notch. There was no significant dental lesion suitable for treatment, so she only received treatment with dental sealants. She recently visited the Department of Pediatrics for a regular checkup, but exhibited no discomfort or progressive abnormalities. She was not referred to the dental hospital.
Case 2
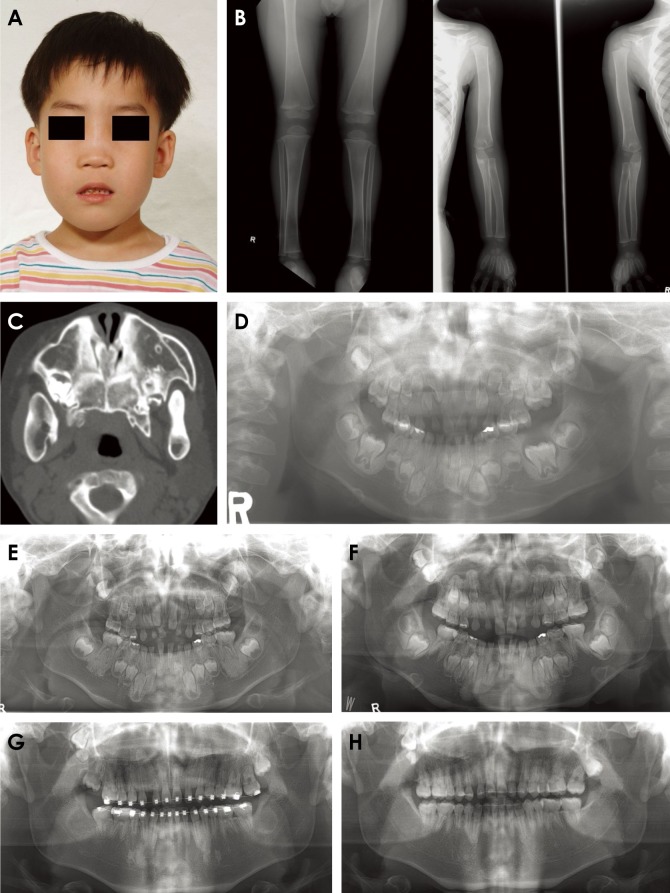
A 6-year-old male patient was referred to the Department of Orthodontics due to malocclusion and delayed eruption. The patient had been diagnosed with autosomal dominant CMD through a genetic analysis when he initially visited the clinic of Pediatric Plastic Surgery of another hospital complaining of progressive facial deformity. Clinically, the patient had a small nose, with a wide and thickened bony nasal bridge and prominent zygomatic arches (Fig. 2A). A lateral radiograph of the ankle showed mild widening of the tibial metaphyseal plate (Fig. 2B). Previous computed tomography from another hospital revealed multiple areas of hyperostosis of the facial bone, including the maxilla and mandible, with bilateral obliteration of the maxillary sinus (Fig. 2C).
A panoramic radiograph was taken to evaluate facial bone overgrowth and tooth development (Fig. 2D). There was severe sclerosis of the maxilla and obliteration of the maxillary sinus. Sclerosis of the tooth-bearing areas was remarkable, and some sclerotic portions had clear boundaries. Sclerosis predominated around the erupting teeth, such as the mandibular first molars. The shape of both condyles was stumpy, and the antegonial notches were underdeveloped.
Serial panoramic radiographs were then collected during 12 years of orthodontic treatment, extending up to the present, and they revealed decreases in the characteristic panoramic imaging features of the patient (Figs. 2E–H). Sclerosis of the alveolar bone decreased significantly after eruption of the permanent teeth. After the completion of eruption of the permanent teeth, there was no significant sclerosis of the alveolar bone. However, sclerosis of the sinus remained. There were 3 impacted tooth in the maxilla: 2 maxillary third molars and 1 supernumerary tooth. There was no detectable change in the shape of the condyle or antegonial notch.
Discussion
The term ‘craniometaphyseal dysplasia’ (CMD) was first introduced by Jackson in 1954 in reference to a rare hereditary bone disease.9 CMD consists of 2 distinct entities. The first is an alteration of the long bones in the metaphyseal regions similar to, but less severe than, the changes seen in metaphyseal dysplasia or Pyle disease. The second feature is an overgrowth of the craniofacial skeleton, similar to the changes described in leontiasis ossea.9
CMD occurs spontaneously or is transmitted in an autosomal dominant or autosomal recessive form.10 Mutations of the autosomal dominant form of CMD have been found in the human ANK gene as in-frame point mutations or as single amino acid insertions or deletions.11 The autosomal recessive form of CMD usually exhibits more severe hyperostosis than the autosomal dominant form.10
CMD can be diagnosed early in infancy due to difficulties in feeding and breathing caused by obstruction of the nasal cavity.12 Both CMD patients in this report initially visited the hospital complaining of difficulties in breathing. Patients with CMD frequently complain of hearing loss, visual disturbance or blindness, and facial palsy, possibly due to nerve compression.10
According to the literature, management of CMD is difficult, and treatment by medical or surgical methods is not satisfactory. Calcitriol, low calcium intake, bisphosphonates, and somatostatin have been suggested as treatments for CMD, but with varying results.13 Surgical treatment including decompression has also been reported, but multidisciplinary support for this treatment is necessary.14
In this report on 2 CMD patients, some common features of CMD were clearly detected on panoramic radiography. Severe sclerosis of the jaw bone, except for the mandibular basal bone, was present. Stubby condyles and underdeveloped antegonial notches could be helpful in diagnosing CMD. Serial panoramic radiographs showed that sclerosis of alveolar bone decreased significantly after the eruption of the permanent teeth. This characteristic phenomenon could be caused by the abnormal function of bony remodeling.8 Since bony remodeling plays an important role in the eruption of teeth, relatively abnormal sclerosis could be commonly observed. Sclerosis was thought to have decreased after eruption because of the diminished importance of bony remodeling. There was no detectable change in the shape of the condyle or antegonial notch after the eruption of the teeth.
Sclerotic changes of the cranial bone can suggest osteopetrosis, frontometaphyseal dysplasia, or Paget disease,15 but the imaging features of panoramic radiographs described in this report could contain possible pathognomonic features of CMD.
Patients with CMD usually show otorhinolaryngological symptoms at first and seek treatment for dental abnormalities after being diagnosed with CMD. For patients without clear symptoms, common radiologic features of CMD could be discovered by routine panoramic radiographs. If it is possible to detect suspected CMD patients through panoramic radiographs, further medical examinations for a proper diagnosis and further treatment can be recommended. Since CMD is not well treated and can only be controlled, it is essential to properly diagnose CMD patients as soon as possible.
 XML Download
XML Download