

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Odontomas, which are formed from an overgrowth of epithelial and mesenchymal cells,1 are classified as benign, and are one of the most commonly occurring types of odontogenic tumors.2 Due to their limited and slow-growing characteristics, they are considered to be odontogenic hamartomas. Odontomas are subdivided into compound and complex odontomas depending on the degree of differentiation of the tooth material and their gross similarities to normal teeth in terms of whether they have crowns and roots.3 Generally, odontomas do not exceed 3 cm in diameter.4 However, in some rare cases, large odontomas1, also known as giant odontomas,5 which have a diameter exceeding 3 cm, may be observed on panoramic radiographs. Only 11 cases of “giant” or “large” odontomas have been reported since 2010, and no report has presented unified criteria suitable for assessing their size.
This study presents the case of a radiopaque mass measuring 3 cm in diameter that was diagnosed as a complex odontoma with an impacted third molar in the right mandible. Additionally, a review of the published cases was conducted to identify the most common type and site of giant odontomas.
Case Report
A 28-year-old female patient with schizophrenia presented with pain of a month's duration in the right mandible. A lesion located in the right aspect of the mandible was observed on a panoramic radiograph taken at a local dental clinic. Following this discovery, the case was referred to Wonkwang University Daejeon Dental Hospital for further management.
In the panoramic view, a calcified mass with a radiolucent rim and heterogenous radiopacity, together with an impacted third molar, was seen (Fig. 1). On a cone-beam computed tomography (CBCT) scan (Alphard-3030, Asahi Roentgen IND. Co. LTD., Tokyo, Japan; field of view, 10.24 cm; 102 mAs; 80 kV; exposure time, 17 s; and 1 mm thickness), a radiopaque mass measuring approximately 30×25×20 mm was found in the right posterior mandibular area with buccal cortical bone expansion and thinning. Additionally, the follicular space of the crown of the impacted third molar was found to be continuous with the radiolucent rim of the radiopaque mass (Fig. 2).
Complex odontoma was diagnosed based on the radiographic findings, because the follicular space of the impacted third molar extended to the boundary of the radiopaque mass. Additionally, it was suspected that the heterogenous radiopacity of the mass was the result of a combination of enamel, dentin, and cementum. Additionally, since the diameter was 3 cm, it was diagnosed as a giant odontoma according to the published literature.
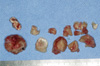
Removal of the giant odontoma and extraction of the left maxillary and left and right mandibular third molars with left iliac bone grafts were done under general anesthesia. During the surgery, the odontoma and impacted right third molar were well separated (Fig. 3). An iliac block bone was fixed in position with 2 mini-plates, and maxillomandibular fixation (MMF) was performed using a skeletal anchorage system screw and rubber (Fig. 4). The MMF was kept in place for 1 week. After its removal, the specimen was subjected to a histopathological examination, which revealed a mixed pattern of enamel and dentin arranged randomly. This discovery confirmed the diagnosis of complex odontoma (Fig. 5). Removal of the plates was done under general anesthesia 6 months after surgery. The patient was followed up and no major postoperative complications were observed.
Discussion
Odontomas are composed mainly of enamel, dentin, and cementum, and are the most commonly occurring benign odontogenic tumor, accounting for 22% of all such lesions.67 They develop and mature when the permanent teeth are formed, and their development ceases when the permanent teeth are fully matured.3 The etiology of odontomas is still unclear, but they are presumed to be caused by trauma and infection, genetic factors, or a family history of conditions such as Gardner syndrome and Hermann syndrome.89 Clinically, odontomas are asymptomatic, and are often found incidentally among teenagers. It has been reported that 75.3% of odontomas are detected at routine dental checkups.3 They occasionally disturb the eruption of deciduous teeth, and roughly 70% of them are associated with impaction, malpositioning, aplasia, malformation, and devitalization of adjacent teeth.10 Pain and inflammation associated with odontomas have been reported in only 4% of cases.1
Odontomas are categorized as compound or complex. Previous studies have shown that compound odontomas are mainly found in the anterior maxillary area, while complex odontomas are found in the posterior mandibular area.1112 The sex predilection of this condition is controversial; however, some authors reported that compound odontomas were commoner in males, while complex odontomas were slightly commoner in females.2 Furthermore, both types of odontomas tend to occur on the right side of both jaws.13
Radiographically, complex odontomas are calcified, irregularly-shaped radiopaque masses with narrow radiolucent rims around them and no similarities to the tooth structure. The radiopacity of an odontoma depends on its developmental stage and degree of mineralization. In the first stage, the odontoma is radiolucent due to lack of calcification. In the intermediate stage, slight radiopacity is seen as a result of partial calcification, while in the third stage, radiopacity is increased, with the mass surrounded by a radiolucent rim determined histologically to be connective tissue.3
Generally, due to their limited growth, it is rare that the diameter of complex odontomas exceeds 3 cm.4 In a study by Miki et al., only 4.3% of odontomas were found to be larger than 3 cm.14 The terms “giant odontoma” and “large odontoma” were used to search Google Scholar and PubMed for reports published since 2010. This search retrieved 11 cases that provided data on the sizes of the odontomas (Table 1). A further review showed that only 8 of the cases of reported giant odontomas with diameters exceeding 3 cm. In these studies, giant odontomas tended to be located on the right (9 of 11), and in the mandibular (9 of 11), and posterior (8 of 11) areas. Furthermore, most giant odontomas were classified as complex odontomas (7 of 11), and they occurred mainly in patients under 30 years of age (9 of 11).
In our case, the complex odontoma measured 3×2.5×2 cm, which is similar to the size of the odontoma described by Vengal et al.15 A giant odontoma measuring up to 6 cm has been reported, with the largest odontoma weighing 0.3 kg.5 The abnormal size of the lesion resulted in expansion of the jaws and facial asymmetry. Giant odontomas rarely perforate the oral mucosa, and when they do, they are referred to as sequestrating or erupting odontomas.16 When this happens, pain, inflammation, and infection of the adjacent oral structures, such as bone, adjacent teeth, and gingiva occur. Furthermore, in our case, the radiolucent area surrounding the crown of the impacted third molar, which was suspected to be the dental follicle, was continuous with the radiolucent rim of the giant odontoma. Through this radiographic evaluation, it was determined that the giant odontoma developed from the malformed dental epithelium of the impacted third molar. Additionally, the third molar was severely impacted, judging from the malpositioning of the adjacent tooth, and this impaction resulted from the presence of the giant odontoma.
Based on the radiolucent rim around the radiopaque mass on the radiograph, the differential diagnoses considered included osteoma and cemento-osseous dysplasia (COD). Other mixed odontogenic tumors such as ameloblastic fibro-odontoma or odontoameloblastoma, which grow aggressively, were also considered.17
Radiographically, osteomas are well-demarcated, ovoid, radiopaque lesions18 that can be distinguished from complex odontomas by the lack of a radiolucent rim around the lesion. It is easy for CODs in the end stage to be confused with complex odontomas because they appear as dense radiopaque masses with radiolucent rims on radiographs.19 However, CODs occur in persons over 30 years of age and are related to the root, whereas complex odontomas occur mainly in adolescents and are located in the alveolar bone of the jaw.1 Ameloblastic fibro-odontomas present as well-demarcated radiolucencies containing radiopaque material and usually occur in patients younger than 20 years of age.20 Odontoameloblastomas, in contrast, are characterized by multilocular radiolucent lesions with radiopaque areas resembling dental tissue, and also predominantly affect patients younger than 20 years of age.21 The main difference between complex odontomas and mixed odontogenic tumors is their growth potential, as exemplified by the fact that even an odontoameloblastoma can cause root resorption of the adjacent teeth.
Although an odontoma is a hamartoma, its recommended treatment involves conservative surgical removal and histopathological examination of the mass to differentiate it from other lesions.22 Very few cases of recurrence after removal have been recorded, and the prognosis is excellent.23
This report has provided a better understanding of the clinical and radiological features of complex odontomas. Additionally, cases of giant odontomas can be distinguished from other conditions mostly by the age of the affected patient, the position of the lesion, its sex predilection, and radiological features including differences in the opacity of the radiopaque mass and features of the well-defined radiolucent rim. Its accurate diagnosis is important, and conservative surgery is the most appropriate treatment.





 XML Download
XML Download