

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, progressive autoimmune disease most commonly associated with joint pain, stiffness, and swelling.1 The ideal RA treatment goal is defined as remission, although low disease activity (LDA) is also considered a valuable treatment target.1 Treating patients with RA to a pre-specified target (treat-to-target [T2T]) represents an international initiative to develop recommendations for achieving optimal therapeutic outcomes in patients with RA.23 Initially, an international task force was established, which consisted of 68 rheumatologists from 25 countries. These rheumatologists put forth a series of recommendations based on evidence obtained from a systematic literature review4 and expert opinion.2 Thereafter, the second phase of the T2T initiative was established, with the goal of promoting acceptance and implementation of these recommendations in daily rheumatology practice.
An international survey was conducted among rheumatologists to evaluate the extent to which individual components of the T2T recommendations have been incorporated into clinical practice.5 The Korean College of Rheumatology participated in the global survey and performed a separate survey in Korea alone.6 The Korean survey, administered to rheumatologists by the Korean National T2T Steering Committee, indicated high agreement with and application of the T2T recommendations in daily practice. Despite the positive results regarding the agreement level, the Korean T2T survey concluded that barriers remained for Korean rheumatologists in the application of T2T in practice due to heavy clinical burden and lack of support. In Korea, the 2016 cost of a rheumatology clinic visit in a tertiary medical center as a new patient is USD15 and a follow-up visit is USD12. Because of the low cost of office visits, physicians work hard to see many patients in one session. There is also little staff support from health educators or clinical nurse specialists. Unfortunately, this type of healthcare system may lead rheumatologists to practice suboptimal care, though treatment of patients with RA requires thorough evaluation for multi-organ involvement and disease progression in routine clinic visits. High demands on rheumatologists should be supported by the healthcare system to encourage rheumatologists to take the necessary time to navigate through the complicated decision-making process of treating patients with RA.
The present study aimed to observe treatment results and practice patterns related to the adoption of the T2T principles in the management of Korean patients with early RA. In addition, we investigated whether adopting T2T recommendations is feasible in Korean practice and could benefit Korean patients with RA in terms of clinical and functional outcomes.
METHODS
Patients
This prospective, non-interventional study was performed in 20 institutions across Korea. Participating patients were followed for 12 months. To be eligible for study inclusion, patients had to be ≥ 20 years old; have a diagnosis established according to the American Rheumatism Association 1987 revised classification criteria for RA7; have early RA (2 years or less after diagnosis); and have moderate or high RA disease activity, with a disease activity score of 28 joints (DAS28) > 3.2. The study was conducted from June 2013 to December 2015.
T2T group vs. non-T2T group
Within each of the 20 participating institutions, rheumatologists applied a patient management strategy per their preference (i.e., T2T or non-T2T). Rheumatologists who adopted the T2T strategy in their practice followed the T2T principles and recommendations set forth by the T2T Korean National Steering Committee,6 and their patients were enrolled in the T2T group. Rheumatologists who did not adopt T2T followed their routine clinical practice, and their patients were enrolled in the non-T2T group. The non-T2T group was provided with usual care which includes the following: patients have follow-up appointments in physicians' usual schedule. There is no regular evaluation for disease activity index such as DAS28. The change of disease-modifying antirheumatic drugs (DMARDs) is based on physicians' clinical judgement. This cluster observation study design was chosen because it would have been difficult for the same doctor to treat patients according to different sets of guidelines based on treatment target assignment, and such an approach would likely have influenced their daily practice pattern.8 All rheumatologists participating in the study have been board certified for more than 10 years and are actively involved in patient care in university hospitals. Both T2T and non-T2T adjustments to the prescription of DMARDs were allowed per physician clinical decision, in agreement with the adopted treatment strategy. Although there was no restriction on the choice of medication, following the guidelines of the Korean National Health Insurance System was recommended.
Outcome measures
The following characteristics were evaluated and compared between the T2T and non-T2T groups: the DAS289 and Korean Health Assessment Questionnaire (KHAQ) score10 were determined at baseline and 12 months. DAS28 was calculated based on the erythrocyte sedimentation rate (ESR), with clinical remission defined as DAS28 < 2.6 and LDA defined as 2.6 ≤ DAS28 < 3.2. Based on the extent of change in disease activity level from baseline until the end of the treatment (△DAS28), as well as on the actual disease activity level at the end of the treatment (DAS28), the European League Against Rheumatism (EULAR) response criteria were applied for the classification of patients as good responders (△DAS28 > 1.2; follow-up DAS28 ≤ 3.2), moderate responders (0.6 < △DAS28 ≤ 1.2; follow-up DAS28 > 3.2), or non-responders. Data regarding patient adherence to follow-up visits to their rheumatologist, DAS28 scores, and changes in treatment regimen were also collected. The primary endpoint was the percentage of patients who achieved the predefined treatment target. Secondary endpoints included the percentage of patients who achieved remission and/or LDA, the change in DAS28 at 12 months from baseline (△DAS28), the percentage of patients who achieved good or moderate EULAR response at 12 months, the mean change in KHAQ score at 12 months from baseline, the percentage of patients who achieved a KHAQ score ≤ 0.5 at 12 months, the frequency of follow-up visits, and the changes in DMARD prescription.
Power calculation
In a large cohort study in Korea,11 the incidence of RA was 20/100,000 per year, resulting in 7,354 new cases of RA per year. Another epidemiologic study found that 62.9% of Korean patients with RA have moderate or high disease activity [unpublished data]. The Korean adult population (aged ≥ 20 years) was 36,765,374 in 2010, as reported by the Korea National Statistical Office.12 Considering that 43.1% of Korean patients with RA are treated by rheumatologists in hospitals,13 and estimating a 10% drop-out rate, we calculated a minimum sample size of 334 patients. The present study enrolled a total of 346 patients, which was sufficient to detect the effect of interest.
Statistical analysis
Demographic and disease-related data, as well as the results of all clinical assessments of patients, were summarized using descriptive statistics. For normally distributed data, continuous variables are presented as means with standard deviations, while non-normally distributed data are presented as medians with interquartile ranges (25%–75%). Frequency and percentage are presented for categorical variables. Mean values and frequencies of the parameters were compared by independent t-tests or χ2 tests, as appropriate. For non-normally distributed variables, the Mann-Whitney U test was performed. All statistical evaluations were the results of 2-sided tests, with the statistical significance threshold set at 0.05. The 95% confidence interval was calculated using a normal approximation. All statistical analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA). All missing data points for DAS28 and KHAQ scores were considered “missing.”
RESULTS
Baseline characteristics
Of the 346 patients who participated in this study, 21 were excluded from the analysis because of violation of the inclusion criteria. Among the 325 patients who satisfied the inclusion criteria, 163 and 162 patients were assigned to the T2T and non-T2T groups, respectively. By the end of the study period, 25 and 49 patients were lost to follow-up in the T2T and non-T2T groups, respectively. Patients in the T2T group were younger than patients in the non-T2T group (Table 1). Further, patients in the T2T group had a shorter disease duration than patients in the non-T2T group (Table 1).
Table 1
Baseline characteristics of patients with early RA

Values are expressed as medians (interquartile ranges 25%–75%) or number (%). Patients were stratified into a T2T group and a non-T2T group, according to the treatment strategy applied for 12 months. DAS28 was measured using ESR.
RA = rheumatoid arthritis, T2T = treat-to-target, RF = rheumatoid factor, anti-CCP = anti-cyclic citrullinated peptide antibodies, TJC28 = tender joint count of 28 joints evaluated, SJC28 = swollen joint count of 28 joints evaluated, ESR = erythrocyte sedimentation rate, PGA = patient global assessment, DAS28 = disease activity score of 28 joints, KHAQ = Korean Health Assessment Questionnaire.
![]()
Primary endpoint
In the T2T group, the percentage of patients who achieved the predefined treatment target was evaluated at 12 months. Each investigator chose the predefined treatment target as either remission or LDA for their cluster of patients. In some T2T centers, only remission was predefined as a treatment target, whereas LDA or remission was considered a valid target in most T2T centers. Therefore, 118 patients (72.4%) had LDA or remission as a predefined target, while 45 patients (27.6%) had remission only as a predefined target. In the T2T group, the overall proportion of patients who achieved the predefined treatment target after 12 months of treatment was 55.2% (90/163 patients). Because it is more difficult to achieve remission than LDA, the rate of remission in patient clusters was 35.5%, while the rate of LDA in patient clusters was 62.7% (P < 0.001) (Table 2). However, there was no difference in the rates of remission or LDA whether the target was either remission only or LDA/remission. Because there was no predefined treatment target in non-T2T group, the primary endpoint was not assessed. However, DAS28, KHAQ, and other parameters were assessed as secondary endpoints in the non-T2T group.
Table 2
Proportion of patients achieving the predefined treatment target in the T2T group

Values are expressed as number (%). Patients were stratified into a remission group and LDA group according to the predefined therapeutic target.
T2T = treat-to-target, LDA = low disease activity.
aDifferences were compared between patients with a predefined target of remission versus LDA or remission.
![]()
Change in DAS28-ESR
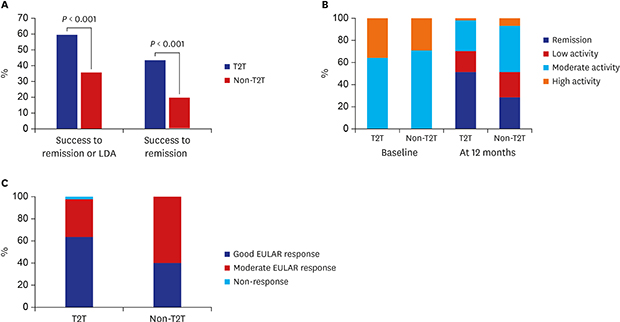
The proportion of patients who achieved clinical remission or LDA at 12 months was 59.5% (97/163 patients) and 35.8% (58/162 patients) in the T2T and non-T2T groups, respectively (P < 0.001) (Fig. 1A). The proportion of patients who achieved clinical remission at 12 months of treatment was 43.5% (71/163 patients) and 19.7% (32/162 patients) in the T2T and non-T2T groups, respectively (P < 0.001). The mean change in DAS28 at 12 months was higher in the T2T group than in the non-T2T group (Table 3). Patients in the T2T and non-T2T groups had significant differences in tender joint count of 28 joints evaluated and ESR among the 4 components of DAS28 (Table 3). Further analysis was performed with data from patients who had DAS28 scores available at both baseline and the end of the study period, namely 138 patients in the T2T group and 113 patients in the non-T2T group (Fig. 1B). At baseline, there was no difference between the groups regarding the proportion of patients with moderate or high disease activity. However, at 12 months, the proportion of patients with moderate or high disease activity was lower in the T2T group than in the non-T2T group (29.7% vs. 48.7%, P = 0.002) (Fig. 1B).
 | Fig. 1Disease activity in patients with early RA with high and moderate activity at baseline. Patients were stratified into a T2T group and a non-T2T group, according to the treatment strategy applied for 12 months. (A) Treatment success defined as remission or LDA, quantified in terms of DAS28. (B) Disease activity (DAS28) at baseline and at the end of the study period (12 months from baseline). (C) EULAR response to treatment.RA = rheumatoid arthritis, T2T = treat-to-target, LDA = low disease activity, DAS28 = disease activity score of 28 joints, EULAR = European League Against Rheumatism.
|
Table 3
Mean change in disease activity and KHAQ scores from baseline in patients with early RA

Values are expressed as medians (interquartile ranges 25%–75%) or number (%). Patients were stratified into a T2T group and a non-T2T group, according to the treatment strategy applied for 12 months. DAS28 was measured using ESR.
KHAQ = Korean Health Assessment Questionnaire, RA = rheumatoid arthritis, T2T = treat-to-target, TJC28 = tender joint count of 28 joints evaluated, SJC28 = swollen joint count of 28 joints evaluated, ESR = erythrocyte sedimentation rate, PGA = patient global assessment, DAS28 = disease activity score of 28 joints.
aValues are expressed as means (standard deviations).
![]()
Clinical efficacy by EULAR response
According to DAS28 values after 12 months of treatment, the proportion of patients that had a good EULAR response was 63.0% (87/138 patients) and 39.8% (45/113 patients) in the T2T and non-T2T groups, respectively (P < 0.001) (Fig. 1C).
Physical function
At 12 months, evaluation of the mean change in KHAQ scores indicated significantly more pronounced improvement in patients in the T2T group than in the non-T2T group (Table 3). Among several KHAQ components, eating and grip activities were improved to a significantly higher extent in patients in the T2T group (Supplementary Table 1).
Frequency of visits and changes in medication
During the 12 months of follow-up visits, patients in the T2T group made more frequent visits for follow-up than the non-T2T group (Table 4). DAS28 was more frequently evaluated in the T2T group than in the non-T2T group (Table 4). DMARD prescriptions were more frequently changed in the T2T group than in the non-T2T group (Table 4).
Table 4
Difference in treatment patterns of patients with early RA in the T2T group and non-T2T group

Values are expressed as medians (interquartile ranges 25%–75%). Patients were stratified into a T2T group and a non-T2T group, according to the treatment strategy applied for 12 months. DAS28 was measured using ESR.
RA = rheumatoid arthritis, T2T = treat-to-target, DAS28 = disease activity score in 28 joints, DMARD = disease-modifying antirheumatic drug, ESR = erythrocyte sedimentation rate.
aThe baseline visit and the 12 months visit were excluded for assessment of changing DMARDs.
![]()
DISCUSSION
The treatment of RA has dramatically evolved over the past several years, with a shift toward more aggressive treatment approaches in the early stages of the disease, combination use of multiple DMARDs, and the emergence of biologic treatment. Although several clinical trials have demonstrated the benefits of the T2T strategy, there are limitations to adopting this approach in daily practice.14 In particular, each health service system is characterized by a certain level of patient awareness, medical costs, accessibility to rheumatology care, and availability of biologics, which can differ from country to country. To our knowledge, this is the first T2T clinical trial in Asia to demonstrate the benefits of the T2T strategy. Specifically, we found that, compared with the non-T2T group, patients in the T2T group achieved higher rates of remission or LDA and better functional outcomes.
The benefits of the T2T strategy include superior disease activity control, better functional outcomes, and long-term economic benefits.1415 However, there have been very few reports in countries outside of Europe and the United States. A small intensive treatment trial was performed in Hong Kong with a historical control group.16 Nevertheless, it is important to evaluate the feasibility of T2T in Korea because of the differences in ethnic background, access to medical care, patient preference toward traditional medicine such as acupuncture, and physician willingness to adopt the T2T strategy. The Korean National Medical Insurance System allows easy referrals to any medical center that a patient prefers.17 As a result, most academic centers run busy rheumatology outpatient clinics to handle a wide range of diseases from osteoarthritis to complicated vasculitis. Reimbursement for expensive medication can be tightly controlled by the national medical insurance system, although most biologics were available during the study period (with the exception of certolizumab and tofacitinib). A brief analysis demonstrated that the T2T trial in Korea is comparable to previous trials conducted in European countries (Table 5). It is interesting to see that the benefits of T2T are reproducible in Korea, which has a different medical system than those in European countries.
Table 5
T2T trials for early RA using DAS28 as a treatment target

| Randomization | Study duration, (mon) | Strategy arm | Study target | Target achievement rate | |
|---|---|---|---|---|---|
| Goekoop-Ruiterman et al.26 | Yes | 18 | Tight control (n = 234) vs. usual care (n = 201) | DAS28 ≤ 2.4 | 31% vs. 18% |
| Soubrier et al.27 (GUEPARD/ESPOIR) | No | 12 | Targeted group (n = 65) vs. routine group (n = 130) | DAS28 ≤ 3.2 | 63.1% vs. 43.8% |
| Schipper et al.28 (DREAM) | No | 12 | Tight control (n = 126) vs. usual care (n = 126) | DAS28 < 2.6 | 55% vs. 30% |
| Korean T2T study (present) | No | 12 | T2T (n = 163) vs. non-T2T (n = 162) | DAS28 < 2.6 | 43.6% vs. 19.7% |
| DAS28 ≤ 3.2 | 59.5% vs. 35.8% |
T2T = treat-to-target, RA = rheumatoid arthritis, DAS28 = disease activity score of 28 joints, GUEPARD = Guérir la Polyarthrite Rhumatoide Débutante, ESPOIR = Etude et Suivi des Polyarthrites Indifférenciées Récentes, DREAM = Dutch Rheumatoid Arthritis Monitoring.
![]()
There are several obstacles to implementing the T2T strategy in Korea. Considering the fact that physician's clinical judgement for remission has low concordant rate with the Boolean criteria in the Korean Observational Study Network for Arthritis (KORONA) cohort,18 it is necessary to set the treatment target. Given the busy daily schedule in Korean clinics, it is difficult to evaluate complex indicators of treatment target, such as DAS28. Without proper incentive to measure DAS28, it will be difficult to establish an appropriate treatment target during a short routine visit to the clinic. Of note, smart phone or computer software applications make it fast and easy to calculate a patient's DAS.19 In addition, frequent visits to the rheumatologist can be difficult for some patients. Furthermore, because the availability of rheumatologists is generally low in some areas, many patients with RA seek medical services from practitioners of primary care, other specialties (orthopedics or pain specialists), or even Korean traditional medicine, with a focus on pain management rather than disease activity management. Medication nonadherence is common in Korean RA patients. According to Korean multicenter clinical data, the medication nonadherence rate was 54.1%.20 However, our study demonstrated that frequent visits to the rheumatologist led to beneficial adjustments to DMARD prescriptions and, ultimately, better disease control. Therefore, the T2T strategy should be considered by Korean rheumatologists and policymakers for future planning to improve patient outcomes.
Compared with the non-T2T group, the T2T group had better functional outcomes, measured in terms of KHAQ scores. This finding is important because, in RA, functional outcomes are strongly associated with economic impact.21 The T2T strategy could be more expensive than current daily practice in Korea, with more frequent visits and greater medication cost. However, better functional outcomes and the prevention of joint damage and disability can reduce long-term medical costs.22 Consistent with our finding, low DAS28-ESR is associated with low KHAQ score in a large Korean RA cohort (KORONA).23
A strength of our study is that patients were recruited from 20 academic medical centers, which cover the majority of rheumatology services across Korea.24 Therefore, our data represent current practice patterns in the management of patients with RA in Korea. There are also limitations to our study. First, there was no randomization within academic centers, which may have influenced the outcome. Second, details of medication and adverse effects were not collected due to budget restrictions. Third, since this was a non-interventional study of daily clinical practice, it was unfeasible to thoroughly control factors that could influence the data regarding clinical effectiveness. In addition, it is possible that the treatment benefits in the T2T group could be partly associated with patient demographics, as the patients in the T2T group were younger with a shorter disease duration than patients in the non-T2T group.
Increasing evidence from randomized controlled trials suggests that in patients with early RA, monitoring disease activity with subsequent adjustment of medication, in the aim of achieving predefined treatment targets, can lead to better outcomes than those achieved via usual care.25 Based on the findings of the present study, the implementation of T2T in Korean clinical practice is feasible and may lead to positive outcomes in patients with RA. To confirm the generalizability of these findings, further studies, including large randomized trials, are necessary.
 XML Download
XML Download