

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although the prevalence of hip pain is different according to various definitions and tends to be lower than that of knee pain,12 hip pain is a common musculoskeletal complaint in general practice. An accurate diagnosis of hip pain is mandatory for providing adequate treatment and to retard the disease progression to end-stage degenerative stage of the hip. The etiology or diagnostic approach for hip pain have been extensively reviewed by many experts.345
Because the hip joint is structurally complex and too deeply buried to access in physical examination, hip pain remains still a difficult issue to evaluate for most primary care clinicians.6 Additionally, the recent development of the concept of femoroacetabular impingement (FAI) syndrome as well as a long list of the causes of hip pain could pose a diagnostic challenge in daily clinical care.35 To date, diagnostic algorithm for hip pathologies has been focused mainly in the pediatric or elderly population.6 However, diagnostic approach has received less attention and has not been established yet in young and middle-aged adults without childhood-specific hip disorders or prevalent osteoarthritis (OA). Based on such background, primary physicians could not be familiar with the diagnosis of hip pain in young and middle-aged adults.
An analysis of cases with un- or mis-diagnosed hip pain would give a chance to feedback information to the referred physicians and could improve their ability to diagnose and manage hip pain. Therefore, the purpose of this study was to analyze descriptively un- or mis-diagnosed hip pain cases referred from primary care to a tertiary hospital, especially in young adults ≤ 50 years old.
METHODS
From January 2013 to August 2016, a total of 2,680 patients were referred to our hip clinic by primary physicians. Among the referred patients with hip pain, we retrospectively enrolled adult patients (≥ 16-year-old) who were not diagnosed or misdiagnosed based on the information submitted on the referral form (n = 1,398; average 32 case/month). The exclusion criteria were as follows: 1) a history of hip surgery, 2) age > 50 years at the time of referral, and 3) pain duration < 6 weeks (Fig. 1). Finally, we identified 150 patients who met the inclusion and exclusion criteria. They included 66 (44.0%) men and 84 (56.0%) women. Clinical characteristics of study subjects are summarized in Table 1. Based on the referral form, a specific diagnosis was not made at the referral in 118 (78.7%) patients.
Table 1
Clinical characteristics of study subjects (n = 150)

Data are presented as mean (ranges) or number (%).
aIncluded bursitis, strain or sprain, and tendinitis; bMeralgia paresthetica.
![]()
In our hip clinic, referred patients are seen by two hip surgeons who have provided specialized orthopedic care for hip conditions for 26 and 10 years, respectively. At the first seeing of patient, we ask patients to locate the site of their pain by their index finger. After a through history and focused physical examination of hip joint and/or lumbar spine, we routinely check baseline hip (standing anterior-posterior [AP], Dunn, and translateral views) and lumbosacral radiographs (standing AP, lateral, and flexion/extension views) in all patients. We also check additional radiographs, acute phase reactants including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), human leukocyte antigen (HLA)-B27, computed tomography (CT) or magnetic resonance imaging (MRI), if further investigations are necessary according to initial impressions. In case suspicious of an underlying rheumatic disorder, who has inflammatory peripheral arthralgia, inflammatory back pain, or extra-articular manifestations,7 the patient is consulted to rheumatology department and finally diagnosed in cooperation with rheumatologists.
In February and March 2018, the medical records and images were thoroughly reviewed by the 2 hip surgeons and 1 rheumatologist who has practiced for 18 years. We collected demographic and clinical data including symptom duration, pain location, and diagnosis of hip pain. Hip pains were classified into three locations; 1) anterior (inguinal or groin region) pain, 2) lateral (trochanteric region) pain, and 3) posterior (buttock, sacroiliac [SI] joint or ischial tuberosity region) pain. Reviewed images included hip and lumbosacral spine radiographs, CT, or MRI. The diagnosis of enrolled patients was made on the basis of clinical features, radiographs and/or laboratory tests by consensus. We tried to select the most explainable cause of their symptom as the final diagnosis, but seven patients had two diagnoses (Table 2).
Table 2
Final diagnosis of un- or mis-diagnosed cases with hip pain

FAI = femoroacetabular impingement, HD = hip dysplasia, SpA = spondyloarthritis, OA = osteoarthritis, ONFH = osteonecrosis of the femoral head.
aIncluded patients with one or more diagnosis (2 patients with FAI and HD, 2 with FAI and spine problems, 1 with FAI with OA, 1 with FAI with calcifying tendinitis, and 1 with snapping hip syndrome with trochanteric bursitis).
![]()
A diagnosis of FAI syndrome was made by motion- or position-related pain in the hip or groin, positive provocative impingement test, and characteristic radiographic findings.8 The characteristic radiographic findings for FAI syndrome included an alpha angle > 55°, acetabular over-coverage (center edge [CE] angle > 39°), herniation pit, or retroverted acetabulum signs (cross over sign, ischial spine sign, or posterior wall sign).89 Additionally, an anterior pincer-type lesion was defined by the presence of retroverted acetabulum and a lateral pincer-type lesion was identified by measuring the lateral CE angle (> 39°).10 An anterior cam-type lesion was defined by alpha angle measurement (> 55°) and a lateral cam-type lesion was by a pistol grip deformity. Moreover, FAI syndrome was classified into pincer, cam, or combined-types according.
Hip dysplasia (HD) was defined as Wiberg's CE angle < 20°.11 The diagnosis of osteonecrosis of the femoral head (ONFH) was made according to Association Research Circulation Osseous (ARCO) classification system.12 Also, the diagnosis of spondyloarthritis (SpA) was made based on the Assessment of SpondyloArthritis international Society (ASAS) criteria.13
Statistical analysis
All continuous variables were described as means with ranges (minimum–maximum). For comparisons of the distribution of categorical variables the Pearson's χ2 or Fisher's exact test was employed. Independent t-test or one-way analysis of variance was used to analyze difference in the difference of continuous variables. Statistical analyses were performed using SPSS for Windows version 20 (IBM Corp., New York, NY, USA) and P < 0.05 was considered statistically significant.
RESULTS
Anterior hip was the most common location of the hip pain (43.3%); and posterior hip was the second most common site (29.3%) (Table 1). The distribution of pain in the right and left hips was comparable (38.0% vs. 33.3%) and approximately a third of patients had bilateral hip pain (28.7%). The mean symptom duration was 13.8 (range, 2–96) months for FAI syndrome, 25.8 (2–120) months for HD, 24.3 (5–60) months for SpA, and 16.6 (2–48) months for ischiogluteal bursitis. Thirty-seven (25.7%) of the total patients reported a symptom duration of 24 months or more.
In this study, the most common final diagnosis was FAI syndrome (55.3%), which was followed by HD (13.3%), referred pain from the lumbar spine (9.3%), SpA (7.3%), and ischiogluteal bursitis (3.3%) (Table 2). Among 83 patients with FAI syndrome, HD (n = 2), lumbar spine problems (n = 2), OA (n = 1), and calcifying tendinitis (n = 1) were concurrently diagnosed in 6 patients.
The relationship between the hip pain location and major final diagnoses was shown in Fig. 2 using a heat map: the diagnosis was significantly related with the pain location (P < 0.001). Most patients with FAI syndrome or HD complained of anterior hip pain but those with spine problems, SpA, or ischiogluteal bursitis had posterior hip pain. But the pain sites were not tightly clustered and were variable in each disease, except for ischiogluteal bursitis.
 | Fig. 2Heat map representing the frequency of hip pain location according to the final diagnosis.FAI = femoroacetabular impingement, HD = hip dysplasia, SpA = spondyloarthritis.
aSpine problems included referred pain from spinal stenosis and herniated intervertebral disc in the lumbar spine.
|
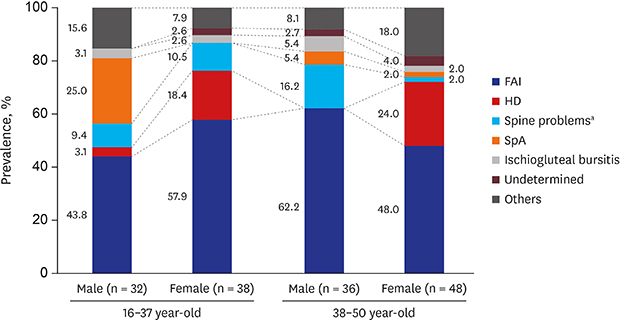
Even when stratified into two age subgroups (16–37 and 38–50 years) according to the mean age of the study subjects, the frequency of FAI syndrome was the highest among the final diagnoses in both subgroups (52.9% in younger and 57.3% in elder subgroups). Younger subgroup tended to have higher prevalence of SpA (72.7% vs. 27.3%). When subgrouped by gender, the distribution of the diagnosis was significantly different (P < 0.001). Men patients were more likely to have SpA (90.9% vs. 9.1%) than women. However, HD (94.4% vs. 5.6%) was more prevalent in women. As a result, the women to men ratio was 17:1 for HD and 1:10 for SpA. The frequency of final diagnoses based on gender and age subgroups was summarized in Fig. 3. When study subjects were categorized into younger women or men and elder women or men subgroups, the prevalence of each final diagnosis was significantly different (P < 0.001). Interestingly, SpA or HD was not observed in younger women subgroup or elder men subgroup, respectively.
 | Fig. 3The distribution of final diagnosis according to gender and age groups.FAI = femoroacetabular impingement, HD = hip dysplasia, SpA = spondyloarthritis.
aSpine problems included referred pain from spinal stenosis and herniated intervertebral disc in the lumbar spine.
|
Of 83 patients with FAI syndrome, 37 (44.0%) had pincer-type and 33 (39.8%) had combined-type FAI (Table 3). Most patients with pincer FAI (27/37, 73.0%) showed anterior pincer-type lesions and 8 (61.5%) of 13 cam FAI had both anterior and lateral cam-type lesions. Moreover, the combination of anterior pincer-type and both anterior and lateral cam-type lesions was mainly observed in combined-type FAI. Pincer FAI was more frequently found in women (30/37, 65.2%) and combined-type FAI was more prevalent in men (23/33, 69.7%; P < 0.001).
Table 3
Distribution of FAI lesions (n = 83)
FAI = femoroacetabular impingement.
aThe numbers on gray background correspond to those of subjects with combined type FAI.
![]()
SpA was found in 11 patients in this study: 10 (90.9%) patients were HLA-B27 positive and 4 (36.4%) had elevated CRP levels (> 0.05 mg/dL). Non-inflammatory spine problems included lumbar intervertebral disc herniation (n = 8) and spinal stenosis (n = 6). Primary hip OA was observed in only 3 (2.0%) patients. Two patients did not have any history of congenital hip disease, trauma or inflammatory arthropathy but one patient had underlying combined-type FAI syndrome. They all showed hip OA with Tonnis grade ≥ 2.14
DISCUSSION
The diagnostic accuracy and treatment modality of arthritic or non-arthritic hip disease in young patients have been rapidly evolving. This shift has been facilitated by the improvement of our understanding about the functional anatomy of the hip, and the advancement in MRI technology has broadened the differential diagnosis of hip pain. However, many of young adult patients with hip pain have nonspecific symptoms, vague findings in the physical examination, and normal imaging studies.15 Therefore, identifying the source and mechanism of the pain can be difficult.
The current study analyzed the causes of hip pain un- or mis-diagnosed by primary physicians. Various final diagnoses were established in 146 (97.3%) subjects by using data from routine clinical practice at a tertiary hospital. The most common diagnosis was FAI syndrome (55.3%), followed by HD (13.3%), spine problems (9.3%), SpA (7.3%), and ischiogluteal bursitis (3.3%). Ultimately, un- or misdiagnosed hip pain resulted from 4 diseases of FAI syndrome, HD, spine problem, and SpA in 80% of our cases.
Although the concept of FAI was introduced in the 1930s, increasing attention has been paid over ten years in accordance with the popularization of arthroscopic treatment.8 The FAI syndrome is characterized by decreased clearance and abnormal contact between the femoral head-neck junction and the acetabular rim.1617 As the hip flexes and rotates, the front of the ball hits the front of the socket causing a collision known as an “impingement.” Over time, repeated collisions of the ball with the front of the socket can tear the labrum and damage the adjacent cartilage, leading to prearthritic hip pain and secondary OA.1617 The reported prevalence of FAI syndrome is highly variable (1% to 75%) according to the different diagnostic criteria, study populations, and morphologic features of interest.181920 Even FAI-related morphologies can be commonly found in asymptomatic subjects.21 Despite of these findings, FAI-related morphologies significantly increases risk to develop hip OA and are related with hip pain associated with activity.212223 Our study showed that a majority of cases where primary clinicians missed a diagnosis had FAI syndrome. It suggests that more effort has to be made to impart the concept of FAI syndrome to primary physicians.
Among 3 types of FAI-related morphologies, cam or combined-type has been considered more clinically significant lesions in view of symptom or cartilage damage.2425 However, in our study, about 40% of patients with FAI syndrome showed radiographic findings of pincer morphology. Our patients were highly selected because they were composed of cases referred without a specific diagnosis, and the prevalence of 3 types of FAI syndrome might not be comparable to that previously reported. Additionally, all our patients with pincer lesion had symptom and physical examination findings compatible with FAI syndrome and also had no otherwise explainable cause for their symptom. Because the diagnosis of FAI syndrome should be made clinically, but not radiographically,826 primary physicians should be familiar with its clinical features to avoid a delayed diagnosis.
Hip pain in FAI syndrome is commonly located in the inguinal or groin area (anterior hip region) but can be described as pain in the posterior and/or lateral hip regions,1527 as shown in the current study. On physical examination, an important maneuver is the impingement test that is a sensitive screening test for patients with acetabular labral disease and impingement.815 If a patient reports groin pain when passively placing the hip in flexion, adduction, and internal rotation, the patient has a positive impingement test. A recent study suggested that either groin pain with a positive Flexion-Abduction-External Rotation (FABER) test or the combination of a positive impingement and a positive FABER test could serve as a sensitive test for FAI syndrome.28
In this study, the second most common diagnosis was HD, that is involved in 20% to 40% of patients with hip OA.293031 Generally, most HD cases are diagnosed through a screening at birth and during infancy. But some of patients could be diagnosed with HD in adolescence or early adulthood. Several population-based studies reported the prevalence of HD was 3.3% to 7.3% in adult population.323334 Even though adolescent or adult-diagnosed dysplasia and infantile-diagnosed dysplasia may be separate identities, both subsets are women-predominant diseases; 7:1 in adolescent or adult-diagnosed dysplasia and 49:1 in infantile-diagnosed dysplasia.35 In the present study, the women to men ratio was also as high as 17:1. Therefore, primary physicians always consider HD as a cause of hip pain even in women adults. In case of borderline dysplasia (20° ≤ CE angle < 25°), depth history taking, physical examination and thorough radiographic evaluation are essential to properly diagnosis.
It is well known that hip pain can be referred from the lumbar spine and spine problems were the third most common condition in our subjects. The subgroup complained of posterior hip pain alone (57.1%) or both anterior and posterior hip pain (21.4%). Birnbaum et al.36 showed the sensory innervation of the hip joint; the anterior, anteromedial, posteromedial, and posterolateral area of the joint capsule are innervated by the branches of obturator, femoral, sciatic, and superior gluteal nerves (i.e., sensory nerves from L2 to S1), respectively. Additionally, in the Rotterdam Study, de Schepper et al.37 found that the disk space narrowing at the L1/L2 or L2/L3 spine level was significantly associated with hip pain. On the contrary, Nakamura et al.3839 reported that some patients with OA secondary to HD (17%) or ONFH (8%) had referred pain to the low back. These findings suggest that primary physicians do not forget spine or hip lesions as a cause of patient's hip or lumbar pain, respectively.
SpA is a group of chronic inflammatory disease primarily affecting the axial skeleton and enthesis and its prevalence has been reported to be 0.4% to 1.3%.40 SpA has been traditionally considered a men-dominant disease, although the gender difference is much reduced in SpA defined by the ASAS criteria.40 In ankylosing spondylitis, the reported prevalence of hip disease ranges from 19% to 36% and is much higher in patients with a younger disease onset.41 The current study also showed that SpA patients were almost men patients (90.9%), especially younger subgroup (80.0%). A Korean multicenter study also showed that the men to women ratio was 6.1:1 and hip involvement is more prevalent in men patients with ankylosing spondylitis.42 Therefore, in men young patients with hip pain, SpA-focused laboratory evaluation including HLA-B27 or a SI joint radiograph could successfully lead to its diagnosis.
There are several limitations to address in this study. First, because our study was retrospective, important diagnostic clues for other uncommon causes could be lost. For example, abductor sprain or tendinopathy, piriformis syndrome, and adhesive capsulitis of hip were not encountered in our study. Differential diagnosis should also consider other hip pathologies in a real-world clinical setting. Nevertheless, it could not affect the overall context of our study since common diseases are more likely to be more often diagnosed than uncommon ones. Second, this study was performed at a single tertiary referral hospital and the prevalence of hip pathologies is different among nations or races.4344 Also, the limitations include the small sample size and the lack of independent data to replicate our results. Therefore, our results could not be generalized to all populations and more studies are warranted in other populations.
Conclusively, our study showed that top 4 diseases causing hip pain included FAI syndrome, HD, spine problems, and SpA in cases un- or mis-diagnosed by primary physicians. Additionally, meticulous history taking, and physical examinations were useful to determine the cause of hip pain in most cases. Primary care giver should add the diseases into the list of differential diagnosis when assessing patients with chronic hip pain.
 XML Download
XML Download