

 PDF
PDF Citation
Citation Print
Print



The occurrence of a variety of traumatic events, such as the Sewol ferry disaster, child abuse, and building collapses, has increased awareness of posttraumatic stress disorder (PTSD) among the Korean general public.1 PTSD is a highly prevalent and costly condition associated with high rates of comorbid mental disorders, including anxiety, depression, and substance use.2 As early detection and treatment of PTSD symptoms is essential, there has been growing interest in developing effective instruments for screening PTSD symptoms.
The Primary Care Posttraumatic Stress Disorder Screen (PC-PTSD) is a four-item measure that is short and easy to administer.3 It reflects the Diagnostic and Statistical Manual of Mental Disorders-fourth edition (DSM-IV) diagnostic criteria for PTSD.4 Because of its excellent diagnostic accuracy and clinical utility, the PC-PTSD has been widely used to screen for PTSD.3,5 Recently, the PC-PTSD was revised to reflect the new DSM-fifth edition (DSM-5) criteria6 for PTSD (PC-PTSD-5), which reflect the most up-to-date knowledge of the PTSD construct. The PC-PTSD-5 includes five items requiring “yes” or “no” responses; it is identical to the PC-PTSD, with exception of the revised trauma exposure stem and the addition of a fifth item. The trauma exposure stem was designed such that individuals who do not report trauma exposure do not answer subsequent questions about PTSD symptoms. The fifth item was added to assess the new symptom cluster of negative alterations in mood and cognitions, particularly guilt and blame. The previous study with the PC-PTSD-5 has shown good diagnostic accuracy and clinical utility with primary care patients.7 It is essential that we have a screening tool that can identify Korean patients who probably meet the DSM-5 criteria for PTSD. The aims of this study were to develop and elucidate the psychometric properties of the Korean version of the PC-PTSD-5 (K-PC-PTSD-5) by assessing its reliability and validity, and to determine its usefulness for evaluating patients with PTSD.
The subjects consisted of 87 PTSD patients, 73 non-psychotic psychiatric patients with other diagnoses (non-PTSD patients), and 92 healthy controls aged between 18 and 70 years. The patients and controls were recruited from eight medical institutions in all provinces and territories of Korea between September 2016 and March 2017. PTSD and other psychiatric disorders were diagnosed with the Structured Clinical Interview for DSM-5-research version (SCID-5-RV).8 The SCID-5-RV is a semi-structured interview guide for making DSM-5 diagnoses, including depression, anxiety, and PTSD. The eight interviewers in this study were all skilled board-certificated psychiatrists with at least 5 years of experience with PTSD. Interviewer training consisted of lectures on the SCID-5-RV and related questionnaires, observation of an evaluation performed by an experienced psychiatrist, and group evaluation of videos of PTSD patients. The inter-rater reliability of the PTSD module of the SCID-5-RV was high (intra-class correlation coefficient = 0.74). The diagnoses of non-PTSD patients included major depressive disorder (n = 43), panic disorder (n = 6), and general anxiety disorder (n = 24). The healthy control group included 88 randomly selected individuals visiting the institutions for regular health screening. All control subjects were also interviewed with the SCID-5-RV and were determined to be free of past and current psychiatric conditions. This study was approved by the public Institutional Review Board of the Ministry of Health and Welfare of Korea (P01-201508-21-002). All subjects provided informed consent after the study procedure had been fully explained to them.
The English version of the PC-PTSD-5 was initially translated into Korean by three psychiatrists and one psychologist; two other bilingual psychiatrists and one psychologist then blindly performed the back-translation. The preliminary translation was modified until the back-translated version was comparable to the English version. A translation committee, consisting of five psychiatrists, one Korean language and literature professor, and one psychologist produced the final K-PC-PTSD-5.
To elucidate the psychometric properties of the K-PC-PTSD-5, we used the Impact of Event Scale-Revised (IES-R),9 the Beck Depression Inventory (BDI),10 and the Beck Anxiety Inventory (BAI).11 The IES-R is the most widely used instrument for screening and assessing the severity of PTSD symptoms. The BDI and BAI were also selected to determine the concurrent validity of the K-PC-PTSD-5, and the results were not too strongly correlated with measurements of similar but distinct traits. Internal consistency was measured using Cronbach's coefficient. Test-retest reliability and concurrent validity were determined using Pearson's correlation. The K-PC-PTSD-5 cutoff score was obtained using receiver operating characteristic (ROC) analysis, and the optimal cutoff score with the maximum Youden Index (sensitivity + specificity − 1) was used. The area under the curve (AUC), positive predictive value (PPV), negative predictive value (NPV), and kappa values were calculated to derive the suggested optimal cutoff points for the K-PC-PTSD-5. Statistical analyses were performed using the SPSS (ver. 24.0; IBM Corp., Armonk, NY, USA) and MedCalc (ver. 16.8; MedCalc Software, Ostend, Belgium) statistical packages. For all analyses, a two-tailed P value < 0.05 was considered significant.
The mean ages of the PTSD (n = 87), psychiatric control (n = 73), and healthy control (n = 92) groups were 45.6 (standard deviation [SD], 14.3), 44.1 (SD, 12.1), and 44.2 (SD, 9.0) years, respectively. The numbers of men in the three groups were 51 (58.6%), 34 (50.7%), and 41 (44.6%), respectively. No significant differences among groups were found with respect to age (F = 0.455; P = 0.635) and gender (χ2 = 3.546; P = 0.170). The mean duration of symptoms in the PTSD group was 4.2 (SD, 8.8) years. The worst traumas experienced in the PTSD group were serious accidents, such as motor vehicle accidents or man-made disasters (n = 64; 73.6%); physical or sexual assault (n = 17; 19.5%); the sudden or accidental death of a loved one (n = 4; 4.6%); and life-threatening illness or injury (n = 2; 2.3%).
The K-PC-PTSD-5 showed good internal consistency (Cronbach's α = 0.872; P < 0.001). Based on the criterion of 0.30 as an acceptable corrected item-total correlation,12 all five items performed adequately (range, 0.63–0.78). The test-retest reliability was examined by comparing baseline K-PC-PTSD-5 scores with the scores of assessments performed 2 weeks later. The PTSD group included only those who reported no change in their PTSD symptoms and agreed to a second assessment. Among the 87 PTSD patients, 34 were recruited for the evaluation of the test-retest reliability, which was determined to be 0.89 (P < 0.001).
There was a relatively strong correlation between the K-PC-PTSD-5 and IES-R (r = 0.81; P < 0.001). However, the BDI and BAI were more weakly correlated with the K-PC-PTSD-5 than with the IES-R, reflecting good discriminant validity (r = 0.61, P < 0.001; r = 0.69, P < 0.001). The mean total K-PC-PTSD-5 scores were 4.1 (SD, 1.2) in the PTSD group, 2.1 (SD, 1.8) in the psychiatric control group, and 0.5 (SD, 0.9) in the normal control group. These values differed significantly, according to our analysis of variance (F = 165.25; P < 0.001), and the Tukey's post hoc test showed significant differences among the three groups. These results reflected the validity of the K-PC-PTSD-5.
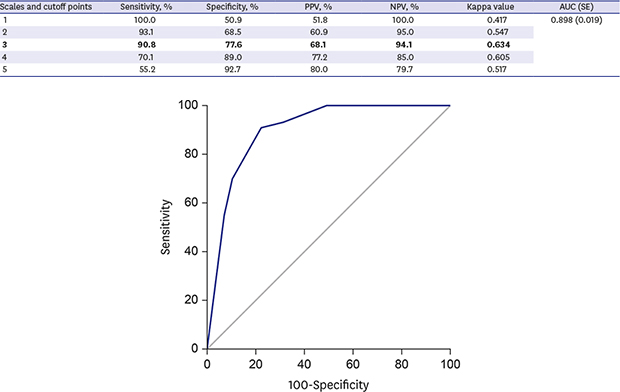
ROC analysis was conducted to determine the cutoff point that provided the highest degree of sensitivity and specificity for the diagnosis of PTSD. The AUC of the K-PC-PTSD-5 was 0.898, and the standard error (SE) was 0.019 (P < 0.001) (Fig. 1); this indicates that the K-PC-PTSD-5 has a high degree of discriminatory power (95% confidence interval, 0.85–0.93). The ROCs indicated that the optimal cutoff point of the K-PC-PTSD-5 for detecting PTSD was 3 (sensitivity, 90.8%; specificity, 77.6%; PPV, 68.1%; NPV, 94.1%; κ = 0.634) (Table 1).
These findings indicate that the K-PC-PTSD-5, which is a Korean version of the useful and novel scale designed to reflect the new DSM-5 PTSD definition, appears to be a valid and reliable screening tool for PTSD. Our analysis of the K-PC-PTSD-5 identified a recommended cutoff point of 3. Despite the difference in the sample (the original PC-PTSD-5 validation study included Veterans drawn from a primary care setting), our results are consistent with the results for the original PC-PTSD-5, including its recommended cutoff score of 3.7 The K-PC-PTSD-5 may be applied to a wide range of populations that have been exposed to various types of trauma. Indeed, the subjects in the current study were recruited from as many as eight institutions, and had experienced a variety of traumas, such as accidents, abuse, rape, and medical problems. However, the present findings must be interpreted with caution considering the relatively small subsample sizes for the individual traumatic events, which renders it difficult to draw any definitive conclusions about issues such as the optimal cutoff point.
In conclusion, the present findings demonstrate that the K-PC-PTSD-5 has good psychometric properties and can be used as a reliable, valid, and timesaving tool to diagnose and assess PTSD. We expect that the Korean adaptation of the PC-PTSD-5 will identify those with PTSD who may benefit from early intervention and thereby facilitate the delivery of mental health care.

 XML Download
XML Download