

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Primary liver cancer is the sixth most common type of cancer and is the second largest cause of cancer mortality worldwide.1 Hepatocellular carcinoma (HCC) is the most frequent primary liver cancer.2 Patients with HCC die due to not only disease progression but also combined complications. Causes of death in patients with HCC in Korea, irrespective of treatment modality and in order of decreasing incidence, are liver failure, gastrointestinal bleeding, and infection.3
Spontaneous bacterial peritonitis (SBP) is a serious complication of cirrhosis and is associated with significant morbidity and mortality.4 SBP is defined as an ascitic fluid infection without an evident intra-abdominal surgically treatable source. Patients with SBP present with signs and symptoms of infection, including fever, abdominal pain, and altered mental status, in addition to an ascitic fluid absolute polymorphonuclear (PMN) leukocyte count 250 cells/mm3; cultures of ascitic fluid are positive for bacteria in about half of patients when cultures are obtained.56 Although mortality related to SBP has markedly decreased, due to earlier recognition of the infection followed by administration of effective antibiotics, it continues to be high, ranging from 20% to 40%.578910 In addition, the 1-year survival rate after recovery from the first episode of SBP is only 30%–40%.11 SBP also occurs frequently in patients with HCC.
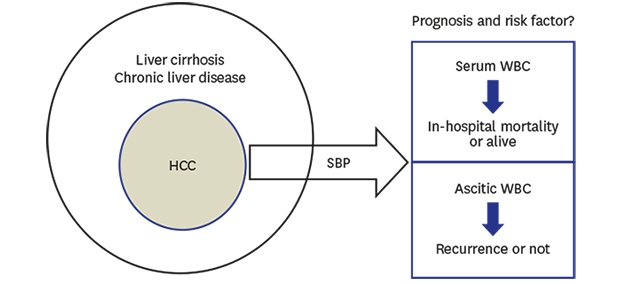
However, information about prognosis of SBP in patients with HCC is limited. We aimed to investigate the clinical course of SBP in patients with HCC over 12 years (2005–2017) in a single center.
METHODS
Patients
We conducted a retrospective single-center study. Between August 1, 2005 and December 31, 2017, we enrolled patients with SBP, including those with HCC, at Konkuk University Hospital. Total and differential cell counts were performed with an optical microscope. In patients with a red blood cell count of > 10,000 cells/mm3 in ascitic fluid, one PMN was subtracted per 250 red blood cells. SBP was diagnosed based on a PMN count of ≥ 250 cells/mm3 in ascitic fluid in the absence of any clinical and radiological findings suggestive of secondary peritonitis.6 We excluded patients whose cell counts were suggestive of secondary peritonitis rather than SBP. Patients without a neutrophil response (PMN count < 250/mm3) in ascitic fluid and a positive ascitic fluid culture–bacterascites were also excluded. All patient data were collected retrospectively from their electronic medical records.
Laboratory findings in serum and ascitic fluid
Serum and ascitic fluid were sampled whilst diagnosing SBP, before antibiotics were administered. The levels of white blood cells (WBCs, × 103 cells/mm3), platelets (× 103 cells/mm3), albumin (g/dL), aspartate aminotransferase (AST, IU/L), alanine aminotransferase (ALT, IU/L), total bilirubin (mg/dL), blood urea nitrogen (BUN, mg/dL), creatinine (mg/dL), sodium (Na, mmol/L), and prothrombin time (international normalized ratio [INR]) in serum, and the WBC (cells/mm3) and PMN (cells/mm3) counts in ascitic fluid were obtained. Liver function was evaluated according to the Child-Pugh (CTP) score, the model for end-stage liver disease (MELD) score and model for end-stage liver disease-sodium (MELD-Na) as previously described.12
Bacterial culture
Diagnostic paracentesis for ascitic fluid culture was performed in all patients who showed symptoms or signs of peritoneal infection, such as fever, leukocytosis, and abdominal pain. Ascitic fluid was placed in blood culture bottles and incubated at 37°C for 7 days. At least 10 mL of ascitic fluid was inoculated into two bottles for aerobic and anaerobic cultures. All isolated organisms in the culture were tested for antimicrobial susceptibility according to the diffusion methods.
Analysis of clinical outcomes
We investigated the antibiotics administered to patients with SBP, bacterial cultured from ascites, the use of prophylactic antibiotics and the incidence of hepatorenal syndrome. Tumor stage information was collected according to Barcelona Clinic Liver Cancer (BCLC) and American Joint Committee on Cancer (AJCC) 8th edition.
We analyzed the difference between the HCC and non-HCC groups. We compared in-hospital mortality group with the alive group of patients with HCC, and also compared SBP recurrence group with the non-recurrence group in patients with HCC.
Statistical analysis
Categorical data are reported as number with percentages. Continuous data are reported as the median with range. Continuous variables were compared via the Mann-Whitney's U test and categorical variables via the χ2 or Fisher's exact test as appropriate.
The area under the receiver operating characteristic (AUROC) curve of variables was calculated to predict in-hospital mortality and SBP recurrence. The Youden index was calculated to select the optimal cut-off value for stratifying patients with a high risk of in-hospital mortality and recurrence.
Variables found to have P < 0.1 in the univariable analysis were included in a multivariable step-wise logistic regression analysis, with backward elimination, to identify independent predictors of the in-hospital mortality and recurrence. Odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated.
A value of P < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 17.0 (IBM Corp., Chicago, IL, USA).
RESULTS
Comparison of non-HCC vs. HCC group
In total, 123 SBP cases, including 49 HCC cases, were enrolled. Men were predominant (48/74, 64.9% vs. 34/49, 69.4%; P = 0.697) and the median age was 58 years in both groups (P = 0.887). Treatment durations were 9 days and 10 days in the non-HCC and HCC groups, respectively (P = 0.719).
The most common etiology was alcohol (32/74, 43.2%) in the non-HCC group and hepatitis B (30/49, 61.2%) in the HCC group (P = 0.009). Portal vein thrombosis was more common in HCC group (18/74, 24.3% vs. 21/49, 42.9%; P = 0.047) and previous SBP history was not different between groups (19/74, 25.7% vs. 6/49. 12.2%; P = 0.108). Serum and ascitic laboratory findings were similar in both groups although thrombocytopenia (P = 0.084) and prothrombin time prolongation (P = 0.064) were severe in the non-HCC group. Median CTP scores were 12 and 11 in the non-HCC and HCC groups, respectively (P = 0.218), and CTP class C was 63 of 74 (85.1%) in the non-HCC group and 38 of 49 (77.6%) in the HCC group (P = 0.339). Median MELD scores were 22.7 and 21.1 (P = 0.122) and MELD-Na scores were 27.1 and 27.2 (P = 0.371) in the non-HCC and HCC groups, respectively.
Cultured bacteria profile was similar in both groups (P = 0.682). In the non-HCC and HCC groups, respectively, microorganisms were isolated from the ascitic fluid in 35 patients (47.3%) and 17 patients (34.7%); 39 patients (52.7%) and 32 patients (65.3%) were culture negative neutrocytic ascites. Among the isolated microorganisms, Escherichia coli (27.0% vs. 22.5%) was the most frequently isolated organism and among these, extended spectrum beta-lactamases (ESBL) positive E. coli were found in 8.1% and 4.1% of non-HCC and HCC cases, respectively. Antibiotics resistance rate was higher in the non-HCC group than in the HCC group (29.7% vs. 12.2%, respectively; P = 0.028).
Empirical antibiotics were administered immediately after SBP was diagnosed. When the signs and symptoms of SBP were persistent or worsening, secondary antibiotics were administered based on the susceptibility of the cultured organisms to the antibiotics. Use of first-line antibiotics were similar between the groups (P = 0.913). The most commonly used first-line antibiotic was cefotaxime (non-HCC: 62/74, 83.8% vs. HCC: 40/49, 81.6%) followed by ceftriaxone (non-HCC: 4/74, 5.4% vs. HCC: 5/49, 10.2%). A total of 15 patients (20.3%) in the non-HCC group and 10 patients (20.4%) in the HCC group were treated with secondary antibiotics due to initial treatment failure (P = 1.000). Prophylactic antibiotic treatment was administered only in 11 (14.9%) patients in the non-HCC group and four (8.2%) patients in the HCC group with low total protein content in ascitic fluid (P = 0.400).
In-hospital mortality was not different between the groups (non-HCC: 25/74, 33.8% vs. HCC: 13/49, 26.5%; P = 0.431). Although cause of death also did not differ between groups (P = 0.214), the most common cause was septic shock in the non-HCC group (12/25, 52.0%) and hepatic failure in the HCC group (5/13, 38.5%).
Recurrence was lower in the HCC group (29/74, 39.2% vs. 10/49, 20.4%; P = 0.031). Development of hepatorenal syndrome did not differ between groups (non-HCC: 14/74, 18.9% vs. HCC: 10/49, 20.4%; P = 1.000), and hepatic encephalopathy was less common in the HCC group (26/74, 35.2% vs. 9/49, 18.3%; P = 0.008). Recurrence free survival was not different between groups (non-HCC: median 49 days vs. HCC: median 41 days; P = 0.759) and overall survival was not different also (non-HCC: median 62 days vs. HCC: median 44 days; P = 0.530).
There was no evidence that HCC itself had an influence on SBP prognosis (Table 1).
Table 1
Baseline characteristics of the enrolled patients

Data are presented as median (range) or number (%).
HCC = hepatocellular carcinoma, HBV = hepatitis B virus, HCV = hepatitis C virus, SBP = spontaneous bacterial peritonitis, WBC = white blood cell, PMN = polymorphonuclear leukocyte, AST = aspartate aminotransferase, ALT = alanine aminotransferase, BUN = blood urea nitrogen, Na = sodium, INR = international normalized ratio, CTP = Child-Pugh, MELD = model for end-stage liver disease, MELD-Na = model for end-stage liver disease-sodium, ESBL = extended spectrum beta-lactamases, BCLC = Barcelona Clinic Liver Cancer, AJCC = American Joint Committee on Cancer.
Comparison of non-HCC vs. HCC group in alcohol related and hepatitis B virus (HBV) related SBP patients
In alcohol related SBP patients, previous SBP history was relatively common in non-HCC group (10/32, 31.3% vs. 0/10, 0%; P = 0.084) and recurrence was more frequent in non-HCC group (15/32, 46.9% vs. 0/10, 0%; P = 0.007). In-hospital mortality, recurrence free survival and overall survival did not differ between groups. In HBV related SBP patients, in-hospital mortality, recurrence rate, recurrence free survival and overall survival were not different between groups (Table 2).
Table 2
Comparison according to HCC or not in alcohol related and HBV related SBP patients

Comparison of in-hospital mortality vs. alive group in HCC patients
Gender, age, treatment duration, etiology, presence of portal vein thrombosis and previous SBP history did not differ between groups. Serum WBC (11.7 × 103/mm3 vs. 8.2 × 103/mm3; P = 0.028) and AST level (120.0 IU/L vs. 65.5 IU/L; P = 0.013) were higher in the in-hospital mortality group. Hyponatremia was severe in the in-hospital mortality group (124.0 mmol/L vs. 128.5 mmol/L; P = 0.025). Other laboratory findings were similar between groups. CTP score (12 vs. 11; P = 0.027) and MELD-Na (30.4 vs. 25.0; P = 0.024) score were higher in the in-hospital mortality group. MELD score was relatively higher in the in-hospital mortality group (24.6 vs. 20.3; P = 0.085). CTP class C was the most common in both groups (in-hospital mortality: 12/13, 92.3% vs. alive: 26/36, 72.2%; P = 0.246). Cultured bacteria, presence of resistance, and antibiotic use were similar between groups.
Although recurrence rate did not differ between groups (in-hospital mortality: 1/13, 7.7% vs. alive: 9/36, 25.0%; P = 0.253), recurrence free survival (median 15 days vs. 50.5 days; P < 0.001) and overall survival (median 15 days vs. 69.5 days; P < 0.001) were longer in alive group. Hepatorenal syndrome was more common in the in-hospital mortality group (in-hospital mortality: 6/13, 46.2% vs. alive: 4/36, 11.1%; P = 0.014) and hepatic encephalopathy was relatively common in the in-hospital mortality group (in-hospital mortality: 5/13, 38.5% vs. alive: 4/36, 11.1%; P = 0.052). BCLC stage was not different between groups and stage D was most common in both groups (in-hospital mortality: 12/13, 92.3% vs. alive: 26/36, 72.2%; P = 0.509). AJCC 8th stage was not different between groups (Table 3).
Table 3
Comparison of in-hospital mortality group vs. alive group in HCC

Data are presented as median (range) or number (%).
HCC = hepatocellular carcinoma, HBV = hepatitis B virus, HCV = hepatitis C virus, SBP = spontaneous bacterial peritonitis, WBC = white blood cell, PMN = polymorphonuclear leukocyte, AST = aspartate aminotransferase, ALT = alanine aminotransferase, BUN = blood urea nitrogen, Na = sodium, INR = international normalized ratio, CTP = Child-Pugh, MELD = model for end-stage liver disease, MELD-Na = model for end-stage liver disease-sodium, ESBL = extended spectrum beta-lactamases, BCLC = Barcelona Clinic Liver Cancer, AJCC = American Joint Committee on Cancer.
Predictor of in-hospital mortality
According to direct comparison, we used serum WBC, AST, Na, CTP score, MELD-Na, hepatorenal syndrome, and hepatic encephalopathy as variables. AUROC analysis was performed for continuous variables and we set cut-off values as: WBC > 11,570 /mm3, AST > 79 IU/L, Na ≤ 124 mmol/L, CTP score > 12, and MELD-Na > 28.9. All were P < 0.05 (Fig. 1). Univariable logistic regression analysis showed all variables were significant, but multivariable analysis showed only WBC > 11,570 /mm3 was significant variable (Table 4).
Fig. 1
ROC curve analysis and AUROC for the prediction of in-hospital mortality. (A) WBC, (B) AST, (C) Na, (D) CTP score, and (E) MELD-Na.
ROC = receiver operating characteristic, AUROC = area under the receiver operating characteristic, WBC = white blood cell, AST = aspartate aminotransferase, Na = sodium, CTP = Child-Pugh, MELD-Na = model for end-stage liver disease-sodium.

Table 4
Predictors of In-hospital mortality in patients with HCC and SBP

Comparison of recurrence vs. non-recurrence group in HCC patients
Gender, age, treatment duration, etiology and presence of portal vein thrombosis were not different between groups (Table 5). Previous SBP history was more common in recurrence group (6/10, 60.0% vs. 0/39, 0%; P < 0.001). Ascitic WBC (5,885 vs. 1,750 cells/mm3; P = 0.039) and serum creatinine (1.6 mg/dL vs. 1.2 mg/dL; P = 0.085) were higher in the recurrence group. Other laboratory findings were similar between groups.
Table 5
Comparison of recurrence group vs. non-recurrence group in HCC patients

Data are presented as median (range) or number (%).
HCC = hepatocellular carcinoma, HBV = hepatitis B virus, HCV = hepatitis C virus, SBP = spontaneous bacterial peritonitis, WBC = white blood cell, PMN = polymorphonuclear leukocyte, AST = aspartate aminotransferase, ALT = alanine aminotransferase, BUN = blood urea nitrogen, Na = sodium, INR = international normalized ratio, MELD = model for end-stage liver disease, MELD-Na = model for end-stage liver disease-sodium, ESBL = extended spectrum beta-lactamases, BCLC = Barcelona Clinic Liver Cancer, AJCC = American Joint Committee on Cancer.
CTP score and MELD score were similar in both groups. The MELD-Na (recurrence: 30.3 vs. non-recurrence: 25.2; P = 0.074) score was relatively higher in the recurrence group. CTP class C was the most common in both groups (recurrence: 8/10, 80.0% vs. non-recurrence: 30/39, 76.9%; P = 1.000).
Culture positive rate (6/10, 60.0% vs. 11/39, 28.2%; P = 0.075) and antibiotics resistance rate (3/10, 30.0% vs. 3/39, 7.7%; P = 0.090) were higher in the recurrence group. Cultured bacteria and antibiotics use were similar between groups.
In-hospital mortality, recurrence free survival and overall survival did not differ between groups. Hepatorenal syndrome and hepatic encephalopathy incidence were similar in both groups. BCLC stage did not differ between groups and stage D was most common in both groups (8/10, 80.0% vs. 30/39, 76.9%; P = 0.910). AJCC 8th stage did not differ between groups (P = 0.225).
Predictor of recurrence
According to direct comparison, we used ascitic WBC, serum creatinine, MELD-Na, culture positive, antibiotic resistance and previous SBP history as variables. AUROC analysis was performed for continuous variables and we set cut-off values as: ascitic WBC > 3,000 cells/mm3, creatinine > 1.2 mg/dL, and MELD-Na > 25.2. Only ascitic WBC was significant (P = 0.003) (Fig. 2).
Fig. 2
ROC curve analysis and AUROC for the prediction of SBP recurrence. (A) Ascitic WBC, (B) Creatinine, and (C) MELD-Na.
ROC = receiver operating characteristic, AUROC = area under the receiver operating characteristic, SBP = spontaneous bacterial peritonitis, WBC = white blood cell, MELD-Na = model for end-stage liver disease-sodium.

Univariable logistic regression analysis showed ascitic WBC, creatinine and previous SBP history were significant variables, and multivariable analysis showed only ascitic WBC > 3,000 cells/mm3 was significant (Table 6).
Table 6
Predictors of recurrence in patients with HCC and SBP

DISCUSSION
Liver cancer is the sixth most common cancer (fourth in men and sixth in women) and the second largest cause of cancer mortality in Korea.13 On the other hand, SBP is one of the most serious complications of cirrhosis. Various cohort studies have examined in-hospital mortality associated with SBP over the last few decades and the mortality of SBP has decreased. Between 1984 and 1989, the Liver Unit at the University of Barcelona Hospital Clinic reported 38% in-hospital mortality in 185 consecutive cirrhotic patients with SBP.14 In a study using the Maryland Health Services Cost Review database of all patients admitted to Maryland hospitals with SBP as a diagnosis from 1988 to 1998, the rate of in-hospital mortality was 32.6%.15 However, between 1998 and 2007, in-hospital mortality associated with SBP using the National Inpatient Sample lowered to 20.2%.16 In a most recent study, overall in-hospital mortality was 17.6% for patients with SBP in the USA from 2006 to 2014.4 However, the prognosis of SBP in patients with HCC is not well known.
In the current study, the HCC group had relatively better prognosis than the non-HCC group. Antibiotic resistance, SBP recurrence, and hepatic encephalopathy were less common in the HCC group. This may be related to some differences in baseline characteristics, such as the etiology of liver disease. HBV is the predominant cause of HCC in Korea, China, and Taiwan.17 According to several retrospective studies, HBV accounted for 62%–75% of HCC cases.1819202122 Heavy alcohol consumption contributes to the development of HCC and increases the risk of developing HCC in patients with HBV or hepatitis C virus (HCV) infection.2324 In Korea, 2.4%–10.9% of HCC has been attributed to alcohol use.13 A prospective observational study reported that 67% of Korean patients newly diagnosed with HCC had a past or current history of alcohol abuse.17 In Korea, the most common cause of liver cirrhosis is HBV, affecting around 57%–73% of the cases. The prevalence of alcoholic cirrhosis has continued to increase up to 31%, compared with the reported rate of 7% in the 1980s.25 Hepatitis virus-related cirrhosis was more frequently associated with HCC than with cirrhosis of other causes.25 In the current study, the most common etiology was HBV in the HCC group, and alcohol in the non-HCC group. In the antiviral treatment era, viral hepatitis is a controllable disease. However, alcohol drinking is still hard to control and there is a problem of compliance. That can lead to repeated development of complication. When comparison between non-HCC group and HCC group was limited to alcohol related SBP patients, non-HCC group had relatively more previous SBP history and higher recurrence rate (Table 2). On the other hand, there was no difference between groups in HBV related SBP patients. Generally, patients with HCC well accept regular follow-up management. Furthermore, although not significant, thrombocytopenia and prothrombin time prolongation were more severe in the non-HCC group. That means underlying liver function was also better in the HCC group, which explains the relatively improved prognosis.
Another difference between the two groups was the presence of antibiotic resistance. SBP caused by resistant bacteria was rare in one recent study from Spain on community-acquired infections (7%), but was far more common in patients with frequent contact with the health care system (22%) and those with nosocomially acquired infection (41%).26 Resistance can result in failure to respond to initial empirical therapy with third-generation cephalosporin in 33%–75% of cases, and such failure to respond is associated with reduced survival.262728 Resistance was lower in the HCC group, and this may be related to lower recurrence in the HCC group.
In the present study, microorganisms were isolated in 52 of 123 patients (42.3%). The results were similar to those of previous studies conducted in Korea (39%–41%), which were lower than those of the Western studies (−60%).2930 The three most common isolates from ascitic fluid cultures in Korea were E. coli, Streptococcus, and Klebsiella.303132333435
We could not conclude that prophylactic antibiotic therapy had a role in prevention of recurrence of SBP since only 15 patients (12.2%) with low total protein content in ascitic fluid were administered with prophylactic antibiotics. Further studies are required on whether prophylactic antibiotics can prevent recurrence of SBP.
The most common cause of death was septic shock, followed by hepatic failure. In the HCC group, hepatic failure was the most common cause of death. A recent study found that septic shock from SBP leads to mortality of > 80%, and each hour of delay in appropriate antimicrobial therapy is associated with a 1.86 times increased hospital mortality.36
Several studies showed HCC is a poor prognostic factor for patients with SBP. Tsung et al.30 showed that HCC, higher serum bilirubin levels, prolonged serum prothrombin time, renal dysfunction, and lower ascitic glucose concentration are associated with higher mortality in cirrhotic patients with SBP. A multicenter retrospective study performed in Korea at a comparatively recent date reported that high mortality rates were seen in patients with a high MELD score. In addition to MELD score, ESBL producing organisms-induced SBP and combined HCC were associated with poor prognosis in patients with SBP.34 However, we could not find any evidence that HCC itself influences prognosis of SBP in patients with HCC.
There have been many studies that investigate risk factors of mortality in SBP. As a serious complication in cirrhosis, SBP can trigger a cascade of events in other organ systems; specifically, renal impairment in cirrhotic patients has been associated with worse prognosis.37 In a landmark study in 1999, Sort et al.38 showed the incidence of renal dysfunction in patients with SBP decreased from 33% to 10% with intravenous albumin infusion given together with antibiotic therapy vs. antibiotic therapy alone, and mortality decreased from 29% to 10%. As SBP mortality rates remain high despite antibiotic and albumin therapy, it is particularly important that clinicians accurately identify high risk patients at the time of presentation. The provision of timely and appropriate antibiotic therapy is likely to reduce sepsis-associated acute on chronic deteriorations in hepatic function and renal function and may affect the overall inflammatory milieu, in part reflected by the peripheral leukocyte count.39 SBP remains the most common trigger of infection-induced acute-on chronic liver failure (ACLF). ACLF whatever its trigger, is characterized by the failure of organs (including kidney, cerebral, liver, coagulation, circulation and lungs) and high risk of death, depending on the number of failing organs.40 Tandon and Garcia-Tsao41 reviewed 18 prognostic studies for in-hospital and 1 month mortalities in adult patients with SBP. In their review, renal dysfunction was the most important independent predictor of mortality in cirrhotic patients with SBP, followed by the MELD score. Another recent study showed that creatinine concentration ≥ 1.5 mg/dL, MELD score ≥ 22, and delayed paracentesis were associated with in-hospital mortality.42 Another study found that mortality of patients with renal failure and SBP was 50% compared with 6% without renal failure.37 Renal injury develops in 30%–40% of patients with SBP and is the best biochemical predictor for mortality.3741 In an attempt to identify independent markers of short-term mortality, a recent systematic review summarized 18 SBP trials that accurately defined SBP and also included a multivariate analysis of prognostic indicators. This review of trials identified renal dysfunction and the MELD score as the top two independent predictors of prognosis.41 Tandon et al.39 showed that in cirrhotic patients with SBP receiving standard therapy, MELD score ≥ 22, and peripheral blood leukocyte count ≥ 11 × 109 cells/L are validated independent predictors of mortality. In summary, renal impairment, peripheral leukocytosis related with systemic inflammation, sepsis, and high MELD score are predictors of mortality. In the current study, high peripheral WBC count, high AST, low Na level, high CTP score, high MELD-Na, hepatorenal syndrome, and hepatic encephalopathy were predictors of in-hospital mortality and the most important factor was high WBC. This result is not different from that of other SBP studies. MELD-Na may be better than MELD because hyponatremia is also an important factor for prognosis. Tumor stage has no effect on mortality and this may be because patients with HCC already have advanced liver disease. We conclude that predictors of mortality are similar between patients with and without HCC.
Recurrence risk factor of current study was different from previous SBP studies. As previously mentioned, prophylactic antibiotic management was not a major factor because only a small portion of patients received such treatment. Patients with prior SBP should receive long-term prophylaxis with antibiotics to prevent recurrence, because the rate of recurrence is 70% in the first year.4344 Tito et al.43 showed risk factors for recurrence, based on univariate analysis, are serum bilirubin (> 4 mg/dL), prothrombin (≤ 45%), and low ascitic fluid protein concentration (< 1 g/dL). Likewise, after evaluating 86 patients who survived their first episode of SBP, a serum albumin concentration of < 2.85 g/dL at hospital discharge was strongly associated with SBP recurrence.45 In the current study, high ascitic WBC, high creatinine, high MELD-Na, culture positive, and antibiotics resistance were possible risk factors and multivariate analysis showed that only ascitic WBC was a predictor of recurrence. Because only 10 patients were recurrence cases, a larger study is warranted.
There were several limitations to this study. First, it was a single center study; therefore, it is unlikely to reflect all of the characteristics of patients with HCC and SBP. Second, because this study was retrospectively designed, the sample size is relatively small and follow-up management was not controlled. Third, the follow-up periods after diagnosis of SBP were short. However, there has been no study focus on clinical outcome of patients with HCC and SBP, and this is a meaningful analysis.
In conclusion, prognosis of SBP in patients with HCC seems relatively less severe than in patients without HCC. This finding may be related to lower antibiotic resistance and better hepatic function with lower development rates of other complications, such as hepatic encephalopathy. This could also be related to presence of strict regular follow-up management in patients with HCC. The most important predictor of in-hospital mortality was serum WBC count, which may be associated with systemic inflammation and risk of sepsis development. HCC itself had little effect on prognosis of SBP. Prospective investigation is required to further investigate this issue.
 XML Download
XML Download