

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With an estimated 570,000 cases and 311,000 deaths in 2018 worldwide, cervical cancer ranks as the fourth most frequently diagnosed cancer and the fourth leading cause of cancer death in women. Cervical cancer is the most commonly diagnosed cancer in 28 countries with a low human development index and the leading cause of cancer death in 42 countries, the vast majority of which are in Sub-Saharan Africa and Southeastern Asia and presenting at a late stage [12]. In other parts of the world cervical cancer is gradually becoming an orphan disease because of the introduction of human papilloma virus (HPV) vaccination and early detection of pre-invasive disease by screening. As a consequence, many patients present at an early stage (International Federation of Gynecology and Obstetrics [FIGO] stage I/IIA) [3].
This early stage is mainly treated by surgery and less frequent by radiotherapy, depending on the diameter of the tumor and sometimes depending on the preference of the treating physician and/or patient. While 2 decades ago surgical treatment for the majority of patients entailed a radical hysterectomy (RH) with a complete pelvic node dissection (one fits all), currently many patients get individualized treatment. The type of individualized treatment depends on the wish to retain fertility (trachelectomy), the wish to lower morbidity (less radical parametrectomy, sentinel node procedure and nerve sparing surgery) and the wish to get a quicker recovery resulting in a shorter hospital stay and a less extensive abdominal scar (minimally invasive surgery). These modifications were gradually introduced over the last 2 decades [456]. The safety of these modifications was and is mostly analyzed by retrospective case series or case-control series, using frequency of recurrences and survival as endpoints and only rarely by randomized controlled trials (RCTs). The problem with this way of analyzing “oncological safety” in case series is that we do not always know what to consider as standard baseline recurrence frequency and/or survival. This also depends on the clinical and pathological characteristics of the patients. In the absence of a RCT a case-control study is considered second best. However, in case-control series the controls (treated by RH) are frequently historical controls. These patients tend to have a much longer follow-up with a resultant higher recurrence rate. When matching is not properly performed and the historical controls have more poor prognostic variables, this may result in comparing “apples with oranges.”
In this review we have critically analyzed the available evidence for the safety of the major modifications in surgical treatment for early cervical cancer (stages IA, IB1, IB2, and IIA1) introduced over the last two decades such as various types of radicality regarding parametrectomy, trachelectomy, and minimally invasive surgery.
SAFETY OF A LESS RH
Over the years surgeons have tried to standardize the extend of radicality of the RH in order to “speak the same language.” From 1974 till 2017 various proposals for standardization of radicality were published (Table 1) [789101112]. These different types of radicality concerned the radicality of the parametrium, the pararectal and paracolpal tissues, with or without classifying nerve sparing surgery as a separate entity. Others also tried to standardize the extend of lymphadenectomy in either 3 classifications [13] or 4 classifications [12] on the basis of the anatomic regions of the pelvic and para aortic lymphatic basin. Because of the direct relationship between extend of RH and morbidity, especially bladder morbidity, many gynecologic oncologists want to diminish the extend of the parametrectomy and paracolpectomy in order to save the autonomic nerve plexus from dissection to avoid this type of bladder morbidity [1415]. The question now arises in which subgroups can we safely perform less radical surgery and what is the evidence for the oncological safety. The first study, hypothesizing that the extend of the radicality/parametrectomy may be less important in a favorable subgroup, used RH specimen with a tumor size of 2 cm or less and absent vascular space invasion (VSI), to show that parametrial involvement in this subgroup was not present [16]. Later, other authors, came to the conclusion that not only tumor diameter, but also the presence of nodal metastases and depth of infiltration were important risk factors for the presence of parametrial involvement (Table 2) [17181920212223]. During the same time period three prospective controlled trials showed that less radical parametrectomy was safe in early cervix cancer, where “early” was defined in some studies as “stage IB”, in another study as stage IB1 and in yet another study as IB1 and IB2 (less than 6 cm) [142425]. In the first prospective controlled study (not randomized but “alternating” treatment) patients either underwent a Wertheim-Meigs procedure (n=108) or a less radical Galvin-TeLinde procedure (n=102) [24]. Recurrences occurred in 20% and 22% of cases and overall survival (OS) was reported to be 72% and 78% respectively. This study is subject to serious criticism. Firstly, no randomization took place, resulting in an imbalance in prognostic variables in favor of the less radical group such as the presence of positive nodes (11% in less radical vs. 17% in more radical group) or parametrial involvement (5% vs. 12%). Secondly, the high frequency of adjuvant radiotherapy (50%) could potentially compensate for less radical surgery, precluding firm conclusions on the effect of radicality.
Table 1
Various classifications of the extent of radicality of the hysterectomy

| Piver et al., 1974 [7] | Trimbos, 2009 [9] | Cibula et al., 2011 [10] | KSOG, 2017 | Querleu, 2017 [11] | |||||
|---|---|---|---|---|---|---|---|---|---|
| Class I | Ventral extension | Type A | Type A | Type A | |||||
| • Identification ureter | • V1-medial to ureter | • No ureteral dissection | Minimum resection of paracervix | • Identification ureter | |||||
| • Hysterectomy (total removal cervix) | • V2-including medial part of posterior leaf of VUL | • No parametrial resection | • Identification ureter | • Hysterectomy lateral of para cervix medial of ureter | |||||
| • No vaginal cuff | • V3-including lateral part of posterior leaf of VUL | • Full removal paracervical tissues up to attachment vaginal fornices | • Hysterectomy (total removal cervix) | • 5 mm resection VUL and RVL | |||||
| • No vaginal cuff | • Vaginal cuff <10 mm | ||||||||
| Class II | Lateral extension | Type B | Type B | Type B | |||||
| Modified RH | • L1-medial to ureter | Modified RH | Transection of paracervix at ureter | B1 | |||||
| • Ureters dissected but not from pubovesical ligament | • L2 between ureter and pelvic side wall | • Ureter unroofed and dissected from cervix | • Ureter unroofed and rolled laterally | • Ureter deperitonized and rolled to lateral side | |||||
| • Uterine arteries dissected medial form ureter | • L3 at pelvic side wall | • Resection of small part of medial leaf VP | • Paracervix transected at level of ureteric tunnel | • Partial resection of uterosacral and VUL | |||||
| • Uterosacral ligaments dissected midway sacral insertion | • Horizontal resection of about 1–1.5 cm of LP | • Uterosacral and VUL: partial resection | • Section of paracervical tissue at level of ureteral tunnel | ||||||
| • Cardinal ligaments dissected op to medial half | • Horizontal resection of 1–2 cm of DP dorsal from cervix | • Neural component of paracervix: no resection | • Vaginal cuff 10 mm and no resection of paravaginal tissue | ||||||
| • Removal upper ⅓ vagina | • Vaginal cuff >10 mm | • No removal of lateral paracervical nodes | |||||||
| • Pelvic lymphadenectomy | B2 | ||||||||
| • As B1 but removal of lateral paracervical nodes | |||||||||
| Class III | Caudal extension | Type C | Type C | Type C | |||||
| Classical RH | • C1-above ureter | C1 | Transection of the paracervix at its junction with internal iliac vascular system | C1 | |||||
| • Complete dissection of ureters except for a small part where the umbilical bladder artery is penetrated the bladder | • C2-above deep uterine vein | • Ureter complete dissected from cervix and LP, partially from VP (1–2 cm) | • Transection of uterosacral ligament at rectum | • Ureters fully mobilized | |||||
| • Uterine artery at the origin of hypogastric | • C3-under deep uterine vein | • LP (transverse): up to medial aspect of internal iliac vessels | • Transection of VUL at bladder | • Paracervix resection at internal iliac artery | |||||
| • Uterosacral ligaments excised at sacral origin | • LP (longitudinal): up to deep uterine vein (caudal part containing splanchnic nerve preserved) | • Resection 15–20 mm vaginal cuff with paracervix | • Uterosacral ligaments resection at level of rectum | ||||||
| • Cardinal ligaments excised as close to pelvic wall | • VP (transverse): resection of 1–2 cm | C1 | • Sectioning VUL at level of bladder | ||||||
| • Removal of upper ½ of vagina | • VP (longitudinal): up to bladder branch hypogastric plexus below ureter | • With preservation autonomic nerves | • Vaginal cuff at least 15–20 mm with paracolpal tissue | ||||||
| • Pelvic lymphadenectomy | • DP (transverse): up to recto-uterine ligament at origin of rectum | C2 | • Preservation of autonomic nerves | ||||||
| • DP (longitudinal): sagittal dissection of recto-uterine and recto-vaginal ligaments | • Without preservation autonomic nerves | C2 | |||||||
| C2 | • As C1 without preservation of autonomic nerves | ||||||||
| • Dissection ureter from ventral parametrial up to bladder wall | |||||||||
| • LP (transvers): as C1 | |||||||||
| • LP (longitudinal): to pelvic floor (splanchnic nerves are sacrificed) | |||||||||
| • VP (transverse): complete removal up to bladder | |||||||||
| • VP (longitudinal): up to level of paracolpium vaginal resection (hypogastric plexus sacrificed) | |||||||||
| • DP (transverse): as C1 | |||||||||
| • DP (longitudinal): complete resection (hypogastric plexus sacrificed) | |||||||||
| Class IV | Dorsal extension | Type D | Type D | Type D | |||||
| As previous with addition of: | • D1-between uterus and rectum | Differs from C2 only in lateral extent | Entire dissection of paracervix with vessels | D1 | |||||
| • Complete dissection of ureter from pubovesical ligament | • D2-anterior of rectal border | • LP (tranverse): sacrificing internal iliac vessels | D1 | • Resection of paracervix to pelvic bony wall sacrificing iliac vessels | |||||
| • Umbilical vesical artery is sacrificed | • D3-halfway rectal circumference | • Lateral border is lumbosacral nerve plexus and piriform and internal obturator muscle | • Resection with iliac vessels, exposing sciatic nerve | • Ureter fully ambulant | |||||
| • Vaginal cuff ¾ of vagina | D2 | D2 | |||||||
| • As D1 with resection of adjacent muscle and fascial structures | • As D1 with resection of adjacent muscles and fascia | ||||||||
| Class V | |||||||||
| As previous with addition of: | |||||||||
| • Excision of portion of ureter/bladder | |||||||||
DP, dorsal parametrium; LP, lateral parametrium; RH, radical hysterectomy; VP, ventral parametria; VUL, vesico-uterine ligament.
![]()
Table 2
Collated literature data on low-risk variables in early cervical cancer predicting absence of PM involvement

| Author | Low risk variables | No. | PM involvement |
|---|---|---|---|
| Kinney et al. [16] | ≤2 cm, VSI negative | 83 | 0% |
| Covens et al. [17] | ≤ 2 cm, DOI <10 mm, negative nodes | 536 | 0.6% |
| Stegeman et al. [18] | ≤2 cm, DOI <10 mm, VSI negative, negative nodes | 103 | 0% |
| Wright et al. [19] | <2 cm, VSI negative, negative nodes | 270 | 0.4% |
| Frumovitz et al. [20] | ≤2 cm, VSI negative | 125 | 0% |
| Kim et al. [21] | DOI ≤5 mm, (3.6% positive nodes, median diameter 16.6 mm) | 140 | 0% |
| Kodama et al. [22] | ≤2 cm, VSI negative, age ≤50 years (1.6% positive nodes) or | 64 | 0% |
| DOI ≤10 mm, VSI negative, age ≤50 years (2.9% positive nodes) | 68 | 0% | |
| Lee et al. [23] | ≤2 cm (2.5% positive nodes) | 40 | 0% |
![]()
In a second prospective randomized study a Piver class II RH was compared with a Piver class III in patients with stage IB1 and stage IB2 (<6 cm) [14]. This study was well balanced regarding prognostic factors and showed no difference in recurrence rate (24% vs. 26%, respectively) and OS (81% vs. 77%). This study, again, showed a high frequency (55% in both arms) of adjuvant radiotherapy. In patients with a tumor diameter >4 cm this frequency was even 80%.
A third, very daring, RCT compared a Piver class I (n=62) with a Piver class III (n=63) hysterectomy in stage IB1 cervix cancer [25]. Recurrence rates (24% and 13%, respectively) and OS (85% and 95%, respectively), although differing quite substantially in absolute terms, did not show significant differences. However, in the small subgroup of patients with a tumor diameter >3 cm there was a significant difference in OS in favor of more radical surgery (74% vs. 97%). This study was clearly underpowered and also showed a very high frequency of adjuvant radiotherapy (69% vs. 55%, respectively).
When these three studies are critically analyzed, we must focus on the high frequency of adjuvant radiotherapy in more than 50% of the patients in all 3 studies. The larger the tumor diameter, the more adjuvant radiotherapy was given (in the poor prognostic group with a tumor diameter of >4 cm this frequency increased to >80% of the patients). Because adjuvant radiotherapy will most likely compensate less radical surgery, the interpretation of the studies discussed here can only be that the real impact of radicality cannot be assessed. There is an indication that the impact of adjuvant radiotherapy in a group of patients with intermediate risk factors (Sedlis criteria) is less important when more radical surgery is used [26]. In the latter study a more radical Okabayashi variant of the Wertheim RH was used in 57 patients with intermediate risk factors. None of the patients had adjuvant radiotherapy and a 6% pelvic recurrence rate was found. This compared favorably with the results of a randomized Gynecologic Oncology Group study where the isolated pelvic recurrence rate was 13% and 19% for patients in intermediate risk groups who did and who did not receive adjuvant radiotherapy after a standard RH [27]. Although non-randomized studies have a lower level of evidence, they become important when the studies showing level 1 evidence are subject to substantial criticism. A recently published retrospective study on 2124 patients with early cervical cancer showed that, other than the conventional prognostic variables such as tumor diameter, vascular space invasion, depth of invasion, lymph node and parametrial involvement, also the radicality of the surgery (using the Leiden TNM classification [9]) had an independent prognostic impact on recurrence rate and survival [28]. The impact of radicality was greatest in tumor diameter >4 cm, while in the subgroup of patients with a tumor diameter <2 cm no difference in disease-free survival (DFS) was seen (Fig. 1). The frequency of 34% adjuvant radiotherapy was much lower than previously discussed in the prospective studies. Another recently published population-based study in stage IB1 cervix cancer also showed no impact on survival of more radical surgery in tumors <2 cm [29]. However, in contrast to the previous study, more radical surgery in tumors >2 cm did not have an impact on survival either. Because of missing information on the frequency of adjuvant radiotherapy for the subgroup of patients with a tumor diameter more than 2 cm who had less radical surgery it is impossible to assess the true impact of more or less radicality in that particular subgroup. An ongoing RCT (SHAPE study) where patients with negative pelvic lymph nodes and a tumor diameter 2 cm or less are randomized to either get a type II RH or a simple hysterectomy and an ongoing observational study in a similar group of patients (ConCerv study) will hopefully confirm the oncological safety of less radical surgery for small tumors [3031].
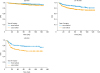 | Fig. 1Kaplan-Meier curves for DFS in tumor diameter subgroups. Five-year DFS for more radical surgery vs. less radical surgery: ≤20 mm, 97% vs. 95% (p=0.348); 21–40 mm, 89% vs. 79% (p<0.001); and >40 mm, 79% vs. 64% (p=0.004). Figure reprinted from PhD thesis with author's permission “Derks, M. (2017). Radical surgery for early stage cervical cancer.”DFS, disease-free survival.
|
RADICAL TRACHELECTOMY (RT)
Since the first publication on RT by Dargent in 1994 numerous retrospective case series and case-control studies have been published over the last 25 years [32]. Originally a vaginal radical trachelectomy (VRT) was recommended for tumors with a diameter less than 2 cm, after the confirmation of tumor negative pelvic nodes, obtained by a laparoscopic approach. Over time several modifications have been introduced, both less radical such as a simple trachelectomy or conization or more radical such as the abdominal radical trachelectomy (ART). With the use of the abdominal and more radical approach also the indications for fertility sparing surgery widened. Also, tumors with a diameter >2 cm were treated by fertility sparing surgery. Unfortunately, pregnancy rates after more radical procedures decreased. To enhance pregnancy rates the use of neo-adjuvant chemotherapy (NACT) was proposed, resulting in down staging of the tumor in order to perform a less radical surgical procedure [33]. Assessing oncological safety in this context is extremely difficult because randomized trials will never be performed. We must therefore deal with the results of retrospective case series or case-control studies. Where some recent case series show recurrence in 1/151 patients (0.7%) [34], others show recurrences in 8/43 (18.5%) patients [35]. This represents the different frequencies of prognostic variables in these patient populations under study. Therefore case-control series are a better way to assess the oncological safety. Here we would like to critically review the available case-control series with a focus on how well controls were matched regarding prognostic factors and duration of follow-up. Marchiole and co-workers [36] were the first to compare VRT with a laparoscopic assisted radical vaginal hysterectomy. The study was not well balanced because tumor diameter ≥2 cm was significantly more frequent in the RH group (40% vs. 18%). Recurrence frequencies did not differ for the small tumors (<2 cm) but more recurrences were observed in patients who had a trachelectomy with a larger tumor (29% vs. 16%). Furthermore, the trachelectomy group represented a very favorable group of patients of which 46% had no residual tumor in the trachelectomy specimen and only 4.2% positive nodes. The authors concluded that a VRT is only safe in tumors less than 2 cm in diameter. The problem of comparing groups with different tumor diameters was also seen in the study of Diaz et al. [37] where size ≥2 cm was significantly more frequent in the RH group (8% vs. 39%). In addition, the distribution of the variable “absence of residual disease in the operative specimen” was not well balanced (53% vs. 22%). Despite the presence of significant more favorable prognostic variables in the trachelectomy group (both VRT and ART), disease-specific survival (DSS) was similar for both the trachelectomy and RH groups, where you would expect a much better survival for the trachelectomy group. A well-balanced case-control study by Beiner et al. [38] of a very favorable subgroup (negative nodes, <2 cm diameter, and 70% no residual), compared VRT with RH. However, even with these very favorable parameters they found 5.6% recurrences in the VRT group and only 1.1% in the RH group. Because this difference was not statistically significant, the authors concluded that a VRT in tumors <2 cm is a safe procedure. It must be kept in mind that the total numbers in this study were small (only 90 patients in each arm) resulting in an underpowered study.
The case-control studies discussed so far showed no significant difference in recurrence rate or survival between VRT and RH (Table 3). In most studies the majority of patients had a tumor less than 2 cm, therefore the conclusion must be that in tumors less than 2 cm a radical vaginal trachelectomy seems to be a safe procedure. Hopefully, we will get a confirmation of this statement from the results of an ongoing prospective observational study where patients with pelvic lymph nodes and a tumor diameter of 2 cm or less are treated by a conization only (Concerv study) [31]. A recent population-based case-control study in the United States compared trachelectomy (n=29), unfortunately not specified if this was a VRT or ART, with RH (n=1,428) and showed a 5-year cancer specific mortality rate of 14.4% vs. 8.4% (p=0.41), respectively [39]. On the basis of these results, the authors advised careful counseling because they felt that the shown trend, although not significantly different, was not in favor of trachelectomy. Also in a series comparing a VRT with a more radical ART in patients with a tumor more than 2 cm, a high recurrence rate of 22% (5/23) was found for the VRT group while no recurrences were found in the ART group (0/19) [40]. This led to the hypothesis that an ART should be used for the larger tumors. As yet 3 case-control studies have been published on the safety of ART [414243]. The first study by van Gent and co-workers [41] showed no difference in recurrence rate and survival for nerve sparing ART vs. nerve sparing RH in a well-balanced but small study. However, with median tumor diameters of 14 and 18 mm for the ART and RH groups, respectively, this study was not very valid in assessing safety of ART for larger tumors. Two recent case-control studies comparing ART with RH included relatively large numbers of tumors >2 cm. The first study by Li et al. [42] was well-balanced regarding prognostic variables. No difference in recurrence rate was found for ART vs. RH in tumors with a tumor diameter more than 2 cm (2/61 [3.3%] vs. 3/82 [3.7%], respectively). The median follow-up for the ART group, however, was significantly shorter (30 vs. 49 months) resulting in a potential lower risk on recurrence for the ART group. The second study by Guo et al. [43] was also well balanced and showed no significant difference in recurrence rate for the ART group vs. the RH group in total. Unfortunately, it was not possible to compare recurrence rates for the subgroup of patients with tumors more than 2 cm because no data were available for the RH group. Median follow-up did not differ between groups (76 vs. 83 months). A remarkable fact was that there were no differences in recurrence rates between patients with tumors more or less than 2 cm in the ART group (2.7% vs. 2.9%, respectively). This is definitely in contrast to literature data in large patient sets where 3.5 times more recurrences are found in patients with tumors between 2–4 cm compared with tumors less than 2 cm [28]. Also, the fact that no recurrences were reported after 30 months is in contrast with literature data showing that 50% of the recurrences occur after 27 months [44]. This same problem was seen in the study of Li et al. [42] where no recurrences were reported after 20 months. Both the fact that there was no difference in recurrence rate between less and more than 2 cm in the Guo et al.'s study [43] and the fact that after 20 and 30 months no further recurrences were reported in the Li and Guo studies, respectively, raises the question if the follow-up was complete. The sparse evidence for the safety of an ART in patients with tumors more than 2 cm, combined with the decrease in pregnancy rates for ART compared with VRT resulted in initiatives such as NACT followed by less radical surgery [33]. At this point in time the few retrospective data preclude a safe evidence-based recommendation. Therefore, we must await initiatives for prospective studies using NACT in this setting.
Table 3
Case-control studies comparing oncological outcomes of RT vs. RH

| Study | Numbers | Follow-up (mon) | Diameter <2 cm | Recurrence | Type of RT | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| RT | RH | RT | RH | RT | RH | RT | RH | |||
| Marchiole et al. [36] | Diameter <2 cm | 118 | 139 | 95 | 113 | 40% | 18% | 7/118 (5.9%) | 9/139 (6.5%) | 118 VRT |
| Diameter ≥2 cm | 6/21 (28.6%) | 9/56 (16.1%) | ||||||||
| Diaz et al. [37] | RFS | 40 | 110 | 15 (total: 44) | 39% | 8% | 1/40 (2.5%) | ? | 28 VRT/12 ART | |
| DSS | 92% | 91% | ||||||||
| Beiner et al. [38] | 90 | 90 | 51 | 58 | 0% | 0% | 5/90 (5.6%) | 1/90 (1.1%) | 90 VRT | |
| Matsuo et al. [39] | 29 | 1,428 | Total: 76 | 100% | 100% | 14.4% | 8.4%* | Unknown | ||
| van Gent et al. [41] | 28 | 77 | 47 | 52 | 14 mm | 18 mm | 2/28 (7.1%) | 11/77 (14%) | 28 ART | |
| Li et al. [42] | 107 | 141 | 30 | 49 | 57% | 58% | 2/107 (1.9%) | 3/141 (2.1%) | 107 ART | |
| Guo et al. [43] | 143 | 186 | 75 | 83 | 52% | 53% | 4/143 (2.8%) | 8/186 (4.3%) | 143 ART | |
DSS, disease specific survival; RFS, recurrence-free survival; RH, radical hysterectomy; RT, radical trachelectomy.
*Five-years cervical cancer specific mortality rate.
![]()
MINIMALLY INVASIVE RH
In the last decades, one of the surgical developments directed at reducing morbidity without compromising survival is the use of minimally invasive techniques, such as laparoscopy and robotic surgery. The advantage of these techniques compared to open procedures is a shorter hospital stay and possibly less complications. Working with a surgical robot has the benefit of improved visibility, highly accurate instrument control and better ergonomics for the surgeon, but it lacks tactile feedback. Several retrospective studies and meta-analyses have been published comparing minimally invasive RH with laparotomy, and recently data of a large randomized trial have been presented. Surprisingly, these studies show conflicting results. A systematic review and meta-analysis of 26 retrospective cohort studies investigated abdominal, laparoscopic and robotic RH in 4,013 patients with early stage cervical cancer in terms of intra- and postoperative outcomes [45]. In this study, the robotic procedure took more time, but was associated with less blood loss, less wound related complications, less febrile morbidity and shorter hospital stay than the open RH. The laparoscopic approach was equivalent to the robot-assisted RH. These results were also seen in a meta-analysis by Wang et al. [46]. They included 12 cohort studies with a total of 1,539 patients comparing laparoscopic (n=754) with open RH (n=785) in early stage cervical cancer. Laparoscopy was associated with less blood loss, less postoperative complications and a shorter hospital stay. Five-year OS and 5-year DFS were similar in both groups. However, only 4 studies in this meta-analysis provided data on DFS and 2 on OS. Park et al. [47] recently published a systematic review and meta-analysis evaluating the safety and effectiveness of robot-assisted RH compared to laparoscopy and laparotomy. They included 22 studies with a total of 1,062 patients. Most of these studies were single-center cohort studies. In robot-assisted surgery less wound infections, fever and urinary tract infections were seen, but more vaginal cuff complications compared to the open group. Complication rates were similar in the robot-assisted and laparoscopy groups. Only four studies in this systematic review reported survival outcomes and no differences were seen between the groups. However, the follow up periods for the various surgical approaches varied and therefore no firm conclusions could be made with regard to survival.
After these reviews four other retrospective studies have been published (Table 4). One study was a multicenter study comparing robot-assisted RH with laparotomy [48]. A total of 259 cervical cancer patients received a robot-assisted RH and 232 patients underwent an open procedure. Mean estimated blood loss, transfusion rates and intra-operative complications were lower with robotic surgery. The length of stay at the hospital was also shorter, while the operation time was longer. Recurrence rate and survival were comparable, however, the patients that were treated by robot-assisted surgery had a shorter follow up time (a mean of 34.6 months vs. 45.2 months for the laparotomy group). A retrospective cohort study in the United States evaluated surgical and clinical outcomes in minimally invasive surgery compared to laparotomy [49]. Of 382 patients with early cervical cancer, 101 underwent a minimally invasive RH and 282 a laparotomy. Patients in the minimally invasive group had less estimated blood loss during surgery, less blood transfusions and a shorter hospital stay. After a mean follow up of 5.1 years (±4.2 years) no differences were seen with regard to OS and rate of recurrence. However, of the patients included in the study, 31.7% had stage IA disease and therefore a very good prognosis to start with, perhaps even regardless of the type of surgery. Another retrospective study investigated the surgical and oncological outcomes in 155 patients that were treated by robot-assisted RH and 149 patients that underwent an open RH [50]. Intra-operative complications, blood loss and length of hospital stay were also lower in the robot group, but recurrence rates were significantly higher. Recurrence was detected in 13.4% of the patients after robotic surgery and in 10.3% after an open procedure. According to the authors, the higher recurrence rate with robot-assisted RH may have been due to the learning curve. A recently published large retrospective study showed similar results [51]. In this study, the National Cancer Database in the United States was used to compare minimally invasive surgery with laparotomy in patients with early stage cervical cancer diagnosed between 2010 and 2013. Of the 2,461 patients included in the study, 49.8% underwent a minimally invasive procedure, and in this group 79.8% had a robot-assisted laparoscopy. In the minimally invasive group the 4-year mortality was 9.1% and in the laparotomy group is was 5.3%. Patients treated by minimally invasive surgery had a 65% higher risk of death from any cause compared to laparotomy (hazard ratio [HR]=1.65; 95% confidence interval [CI]=1.22–2.22). The authors also performed an interrupted time-series analysis using data from the Surveillance, Epidemiology and End Results (SEER) database from 2000–2010. Before the introduction of the minimally invasive RH the 4-year relative survival rate was stable. The introduction of minimally invasive surgery form early cervical cancer in 2006 coincided with the beginning of a decline in the 4-year relative survival rate. Retrospective studies are at risk for bias. RCTs provide a higher level of evidence and therefore the outcomes of the first RCT, the Laparoscopic Approach to Cervical Cancer (LACC) trial, were eagerly awaited. Results from this study were recently published in the New England Journal of Medicine [52]. The LACC study is the first randomized, phase 3 trial comparing minimal invasive RH with the abdominal approach. In this study, 631 patients with early stage cervical cancer (stage IA1 with LVSI, IA2, and IB) were randomized to a total abdominal RH or a minimally invasive RH, either by laparoscopy (84.4% of the minimally invasive group) or robot-assisted (15.6%). Primary objective of the study was DFS at 4.5 years. Secondary objectives included OS, recurrence, and morbidity. Contrary to what was expected, the DFS was worse in the minimally invasive group (86% vs. 96.5% for the abdominal approach group; HR=3.74; 95% CI=1.63–8.58). OS after 3 years was also inferior in the patients treated with a minimally invasive procedure: 93.8% vs. 99% in the laparotomy group (HR=6.00; 95% CI=1.77–20.3). The recurrence rate was 27/319 in the minimally invasive arm compared to 7/312, while there was no difference in short- or long-term morbidities.
Table 4
Summary of characteristics of most recent case-control studies comparing minimally invasive surgery (MI) with open surgery (O) in early cervical cancer. ( 1not specified < or = 2 cm; NR=not reached; 2median survival in months estimated from survival figure; 35 years overall survival; 45 years progression free survival; 5after inverse probability of treatment weighting; 6Statistically significantly different)

| Characteristics | Sert et al. [48] | Diver et al. [49] | Wallin et al. [50] | Melamed et al. [51] | |||||
|---|---|---|---|---|---|---|---|---|---|
| O (232) | MI (259) | O (282) | MI (101) | O (155) | MI (149) | O (1,340)∥ | MI (1,334) | ||
| Stage | |||||||||
| IA | 10% | 14% | 32% | 33% | 8% | 12% | 12% | 12% | |
| IB1 | 80% | 80% | 63% | 66% | 82% | 84% | 88% | 88% | |
| IB2/IIA | 10% | 6% | (IB1+IB2) | 4% | 1% | ||||
| Positive nodes | 12% | 10% | 11% | 9% | 14% | 8% | 11% | 9% | |
| Median diameter | |||||||||
| <12 mm | 43% | 50% | |||||||
| <2 cm | 50%* | 61% | 40% | 40% | |||||
| ≥2 cm | 50% | 39% | 47% | 47% | |||||
| Unknown | 100% | 100% | 13% | 13% | |||||
| Adjuvant RT | 33% | 27% | 20% | 24% | 49% | 22% | 22% | 21% | |
| Recurrence (%) | 9% | 9% | 5% | 6% | 10.3% | 13.4% | ? | ? | |
| Survival | NR | 87%† | 95%‡ | 95% | 90.7%§ | 82.5%¶ | 94.7% | 90.9%¶ | |
| Follow-up | 39 | 34 | 5.1±4.2 years | 45 months | |||||
| Median months | Mean total group | Study ended 2015, published 2016 | Median total group | ||||||
*Not specified ≤2 cm; †Median survival in months estimated from survival figure; ‡5-years overall survival; §5-years progression free survival; ∥After inverse probability of treatment weighting; ¶Statistically significantly different.
![]()
There is no clear answer to the question why a higher recurrence rate and worse survival are seen in (robot-assisted) laparoscopically treated patients in these recent studies. The results are in contrast to many earlier retrospective studies showing a similar survival and less perioperative morbidity with laparoscopy compared to laparotomy. However, retrospective data should always be cautiously interpreted. In retrospective series, the groups may not be well balanced, and furthermore, imaging and radiotherapy techniques were less sophisticated in older cohorts, resulting in relatively worse outcomes in the historical group, in this case the patients treated by laparotomy. Another factor of importance may be tumor size. As mentioned before, tumors larger than 2 cm may require a more radical approach than smaller tumors. In the LACC trial no difference was made between tumors larger than 2 cm and those smaller than 2 cm. At the annual American Society of Clinical Oncology (ASCO) meeting in 2018 an abstract was presented in which tumor size was taken into account in a retrospective comparison between open RH to minimally invasive RH (robotic and laparoscopy) in patients with early stage cervical cancer [53]. Data from the American National Cancer Database were used to evaluate the 5-year survival in patients treated between 2010–2013. A total of 982 patients was treated with open surgery and 910 patients underwent a minimally invasive procedure. A decreased survival was observed in patients with a tumor ≥2 cm that had laparoscopic or robotic surgery (81.3% 5-year survival compared to 90.8% in the open group; p<0.001). Less surgical complications and lower costs were seen with minimally invasive RH.
CONCLUSIONS
Deviation from standard treatment for tumors less than 2 cm seems safe. However, there is no reliable level 1 evidence for this statement. This means that we have to await currently ongoing prospective RCTs (SHAPE and ConCerv studies) to find out if we can really tailor the radicality in patients with tumors less than 2 cm. For tumors more than 2 cm in diameter, it seems that we have to make a choice: either more radical surgery with restricted indications for adjuvant radiotherapy or less radical surgery but with a higher frequency of adjuvant radiotherapy. In the end, the discussion will then focus on the comparison of the morbidity of both treatment modalities. Likewise, fertility sparing surgery in patients with tumors less than 2 cm in diameter seems safe. However, no prospective studies have been published so far to show the oncological safety. Therefore, we are awaiting the results of the ConCerv study, hopefully confirming the reassuring results of the retrospective studies. For tumors with a diameter more than 2 cm retrospective data show conflicting results regarding oncological safety when fertility sparing surgery is used. It is recommended to support initiatives for prospective studies using NACT in these patients in order to be able to perform less radical surgery without compromising oncological safety. The safety of minimally invasive surgery for early stage cervical cancer is a matter of ongoing debate, since a recent RCT showed an increase in recurrence rate and impaired survival for patients treated by minimally invasive techniques. Although a retrospective study showed that tumor size played a role (impaired survival in minimally invasive group only for patients with tumor diameter >2 cm), the RCT was not powered to give a definite answer to this question. Finally, it is our personal opinion, that deviating from the standard open RH in patients with a tumor diameter >2 cm is only recommended in observational studies where patients are counseled about the possible increased risk of recurrence.
 XML Download
XML Download