

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cytoreductive surgery combined with platinum-based combination chemotherapy is the standard treatment for advanced-stage ovarian cancer [1]. However, approximately 80% of patients with advanced-stage disease experience recurrence and most die of the disease within 5 years of diagnosis [2]. To improve survival outcomes, the method of chemotherapy administration has been investigated.
Hyperthermic intraperitoneal chemotherapy (HIPEC) is a multi-modal approach that combines intraperitoneal chemotherapy and hyperthermia. It maintains the theoretical benefit of intraperitoneal chemotherapy and reduces most adverse events from catheter-related problems with delivery of the chemotherapeutic agent at the end of surgery. In addition, hyperthermia is directly cytotoxic, increases the penetration of chemotherapy at the peritoneal surface, and increases the chemosensitivity of cancer cells [3].
In advanced-stage ovarian cancer, primary debulking surgery (PDS) often requires a long duration, massive transfusion (because of bleeding), and multiple bowel resections to achieve optimal cytoreduction. For such cases, the incorporation of HIPEC during surgery might contribute to a higher morbidity. Neoadjuvant chemotherapy (NAC) followed by interval debulking surgery (IDS) could be an alternative to reduce perioperative morbidity [45]. HIPEC after NAC is a feasible and relatively safe option, decreasing the tumor burden and the number of IDS procedures. Recently, a randomized, phase 3 trial showed that the addition of HIPEC to IDS improved progression-free survival (PFS) and overall survival (OS) compared to surgery alone [6].
However, there are some limitations regarding the addition of HIPEC to IDS, as follows: there is no consensus regarding the application of HIPEC to all patients, and there is an unresolved concern about whether the efficacy of HIPEC differs according to the response after NAC and the residual disease at IDS. Therefore, we designed a protocol for advanced-stage ovarian cancer and treated patients based on the response after NAC and the residual disease at IDS. This study aimed to evaluate the feasibility and safety of IDS followed by HIPEC as part of the first-line treatment in patients with stage III/IV ovarian cancer.
MATERIALS AND METHODS
We developed a protocol for the current study, and one gynecologic oncologist performed all procedures according to the study protocol. We recruited patients with advanced-stage ovarian cancer, consecutively, between October 2015 and May 2018. The incorporation of HIPEC after IDS was first introduced at Yonsei Cancer Hospital in October 2015. The eligibility criteria were as follows: 1) patients with histopathologically confirmed International Federation of Gynecology and Obstetrics stage III or IV ovarian, fallopian tube, and primary peritoneal carcinoma. In the cases of stage IV, distant metastases were supradiaphragmatic lymph node metastasis and/or parenchymal liver metastasis. Most patients achieved near-complete remission (no uptake on positron emission tomography-computed tomography [CT], no gross lesions on chest CT) at the supradiaphragmatic lymph node after NAC. When the distant metastatic lesion remained, it was removed from the IDS; 2) patients who underwent IDS following NAC; and 3) patients who received more than 1 cycle of NAC before IDS.
This study was reviewed and approved by the institutional review board (IRB) at Severance Hospital, Yonsei University Health System, Seoul, Korea (IRB number 4-2018-0518).
1. Advanced-stage ovarian cancer management protocol
The advanced-stage ovarian cancer management protocol used in our study is described in Fig. 1. All the patients, who were referred to one gynecologic oncologist for HIPEC, were thoroughly evaluated in order to determine the tumor burden of ovarian cancer. The diagnostic workup included esophagogastroduodenoscopy, colonoscopy, and CT of the chest, abdomen, and pelvis, with intravenous contrast agents. Positron-emission tomography CT was considered if extra-abdominal metastasis was suspected or difficult to detect by CT.
 | Fig. 1Flow diagram of the study population.
ASA, American Society of Anesthesiologists; ECOG, Eastern Cooperative Oncology Group; HIPEC, hyperthermic intraperitoneal chemotherapy; HTD, high tumor dissemination; IDS, interval debulking surgery; NAC, neoadjuvant chemotherapy; PDS, primary debulking surgery.
|
Our institution applied the following selection criteria for the use of NAC as the primary treatment strategy. NAC was performed when one of the following three criteria was met: 1) high tumor dissemination was observed on initial imaging studies and was assumed to occur under the following conditions: a) multiple and unresectable extra-abdominal metastases; b) multiple liver parenchymal metastases or pulmonary metastases; and c) extensive small bowel/mesenteric root involvement, 2) patients had a poor performance status and high operative risk because of medical comorbidities, or 3) optimal debulking surgery (residual disease measuring 1 cm or less) was unsuitable because of a high tumor burden (Fagotti score ≥8). For diagnostic laparoscopy, the degree of tumor burden was determined with the peritoneal carcinomatosis index (PCI) described by Harmon and Sugarbaker [7] and the Fagotti score [8].
All patients, preferably, were recommended to receive 3 cycles of NAC, IDS followed by HIPEC, and 3 cycles of postoperative adjuvant chemotherapy (POAC). HIPEC was not incorporated in patients in whom complete remission was achieved after 3 cycles of NAC. After NAC, complete remission was determined by a combination of the response to chemotherapy and radiologic findings and by the absence of operative findings of gross visible tumors. Additionally, HIPEC was not performed in patients with excessive bleeding (estimated blood loss ≥4,000 mL) during surgery and in cases of patient refusal. For NAC and POAC, all patients received carboplatin (area under the curve of 5 to 6) and paclitaxel (175 mg/m2).
At the time of IDS, the degree of tumor burden was also determined with Harmon and Sugarbaker's PCI and the Fagotti score. All patients underwent surgery with the intent to achieve complete cytoreduction (no gross residual disease). Every patient underwent the same routine of procedures, beginning with complete omentectomy, hysterectomy, bilateral salpingo-oophorectomy, and the removal of all macroscopically detectable lesions using surgical resection combined with electrofulguration, after peritonectomy techniques. If the rectosigmoid region was affected, it was resected ‘en bloc’ with digestive reconstruction by mechanical colorectal anastomosis. If the diaphragmatic region was affected, liver mobilization and diaphragmatic peritonectomy were performed. Pelvic and para-aortic lymphadenectomy was performed only for patients with gross nodal disease detected by preoperative imaging studies or operative findings.
HIPEC was performed immediately postoperatively. Of 27 HIPEC cases, 22 were performed using closed methods and 5 were performed using the open method. Paclitaxel was used at a dose of 175 mg/m2, and chemotherapeutic agents were diluted in 3 L of 1.5% dextrose solution for peritoneal dialysis. Initially, 3 L of a heated perfusion solution was infused into the abdominal cavity at a rate of 800–1,000 mL/min through the inflow tube using the Belmont Hyperthermic Pump (Belmont Instrument Corporation, Billerica, MA, USA). Three intra-abdominal thermometers (1 positioned in the pelvis and 2 in the diaphragm area) were used to monitor the temperature inside the peritoneal cavity during the infusion, which remained constant between 42°C. The duration of the HIPEC procedure was 90 minutes, after which the perfusion solution was completely drained and bowel anastomosis was performed by the colorectal surgeon (MS Cho) if needed.
2. Endpoints and statistical analysis
The primary endpoint was PFS. The secondary endpoints included treatment morbidity and OS. The analysis was performed on an intention-to-treat basis. All patients who started the treatment were included in the analysis.
Data of patient demographic and clinical characteristics are summarized using standard descriptive statistics. Disease progression was defined according to the response evaluation criteria in solid tumors, version 1.1 or based on an increase from baseline in the cancer antigen (CA)-125 level, whichever one of those criteria was met first, as recommended by the Gynecologic Cancer Intergroup. OS was defined as the time from diagnosis until death due to any cause. PFS and OS curves were estimated using the Kaplan-Meier method. Perioperative complications were graded according to the Memorial Sloan-Kettering Cancer Center surgical secondary events grading system [9]. Major complications were defined as Memorial Sloan-Kettering Cancer Center (MSKCC) grade ≥III. Operative mortality was defined as death occurring within 30 days postoperatively (grade V). Other adverse events were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events Version 3.0. The analyses were performed using SPSS (version 21.0; IBM Corp., Armonk, NY, USA). Statistical significance was assumed at p<0.05.
RESULTS
1. Patients' characteristics
During the study period, 65 women were treated by one gynecologic oncologist using the advanced-stage ovarian cancer management protocol. After excluding 25 patients treated with PDS, 40 patients were enrolled in the study. HIPEC was not performed in 13 of the 40 patients for the following reasons: complete remission after NAC in 4 patients, excessive bleeding during the procedure in 3 patients (hepatic segmentectomy, iliac vein rupture, severe adhesions in pelvic cavity), suboptimal cytoreduction in 1 patient, poor performance status in 4 patients, and patient refusal in 1 patient. Twenty-seven patients underwent HIPEC, with a 175 mg/m2 paclitaxel infusion administered into the peritoneal cavity over 90 minutes at an inflow temperature of 42°C (Fig. 1). The demographic and baseline disease characteristics and surgical and treatment information are shown in Table 1. At baseline, the median patient age was 63 (range, 43–77) years, 62.5% of the patients presented with comorbidities (hypertension, diabetes, hypothyroidism, etc.), and 57.5% of the patients had stage IV metastasis. Sixteen stage IV patients underwent IDS with HIPEC. Twelve patients had supradiaphragmatic lymph node metastasis, and 4 patients had parenchymal liver metastases. Eleven patients achieved near-complete remission after NAC. The metastatic lesions remained in 5 patients after NAC and was removed from the IDS. The median CA-125 level was 1691.7 (range, 75.2–17,303.1) U/mL. Thirty-seven (92.5%) patients had serous histology. The median number of NAC cycles was 3 (range, 1–4). The median number of PCIs at diagnostic laparoscopy was 10 (range, 8–14). Twenty-four (60.0%) patients underwent diaphragmatic peritonectomy, 11 (27.5%) patients underwent bowel resection at IDS, and 28 (70%) patients underwent pelvic or paraaortic lymph-node dissection. In 14 patients (46.7%), no gross residual tumor was observed after IDS. The mean operative time was 509.0 (range, 129–915) minutes. Twenty-nine (72.5%) patients received blood transfusion during surgery. The median time interval between IDS and POAC initiation was 21 (range, 8–50) days. The surgical findings and postoperative outcomes of patients treated with HIPEC are shown in Table 2. The median value of PCI at IDS was 8 (range, 1–16), and 6 (22.2%) patients showed high tumor burden (Fagotti score ≥8). Two patients showed an estimated blood loss of 2–4 L and 4 patients received more than 5 units of blood transfusion. The mean operative time was 543.8 (range, 277–915) minutes. Five (18.5%) patients had major postoperative morbidity (restricted to grades III–V).
Table 1
Patients' characteristics and surgical information (n=40)

Values are presented as median (range) or number of patients (%).
ASA, American Society of Anesthesiologists; CA, cancer antigen; FIGO, International Federation of Gynecology and Obstetrics; NAC, neoadjuvant chemotherapy.
![]()
Table 2
Surgical findings and postoperative outcomes of HIPEC (n=27)

Values are presented as median (range) or number of patients (%).
HIPEC, hyperthermic intraperitoneal chemotherapy; PCI, peritoneal cancer index; PIV, predictive index value
![]()
2. Safety and treatment administration
The median hospital stay was 12 (range, 3–131) days. No patients died within 30 days postoperatively (grade V events). Major postoperative morbidity (restricted to grades III–V) was encountered in 5 patients and resolved completely in 4 (Table 3). Among these, 2 patients needed secondary surgical revision. One patient underwent total mastectomy with axillary lymph node dissection because of breast cancer at the time of IDS with HIPEC and underwent emergency surgery for postoperative breast hematoma. The other patient underwent prompt surgical intervention 2 weeks postoperatively because of sudden bleeding in the mesenteric vessel. This patient had deep venous thrombosis in the right infra-popliteal vein due to carcinomatosis at the time of diagnosis, and anticoagulation therapy was continued before and after IDS. The sequela of hypoxic brain damage prevented the administration of POAC.
Table 3
Postoperative grade III/IV complications according to the Memorial Sloan-Kettering Cancer Center surgical secondary events grading system from days 0 to 30

HIPEC, hyperthermic intraperitoneal chemotherapy; ICU, intensive care unit; VATS, video-assisted thoracoscopic surgery.
*Conventional surgery included hysterectomy, bilateral oophorectomy and omentectomy, pelvic/para-aortic lymph node dissection, and appendectomy.
![]()
The median time interval to POAC after IDS was 20 (range, 8–50) days; POAC was initiated for 14 (46.7%) patients after 20 days. This delay was mostly due to postoperative complications of radical surgery. The patient with the greatest delay was reintubated because of severe pulmonary edema and was then readmitted to the intensive care unit.
3. Survival
After a median follow-up of 14.5 months, 42 (64.6%) patients were alive and disease-free, 21 (32.3%) patients were alive but had a relapse, and 2 (3.1%) patient died of disease-related causes.
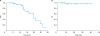
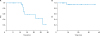
The median PFS was 19.7 months and the median OS was not reached for those who received NAC (Fig. 2). The median PFS was 21.3 months, and the median OS was not reached for those who received HIPEC (Fig. 3). Considering all 65 patients with advanced-stage disease, including those who underwent PDS, the median PFS was 21.3 months, and the median OS was not reached (Supplementary Fig. 1).
DISCUSSION
Our study showed the feasibility and acceptable toxicity of adding HIPEC to the standard first-line treatment for patients with advanced-stage ovarian cancer. Paclitaxel-based HIPEC resulted in major postoperative complications (MSKCC grade ≥III) in 5/18 (27.8%) patients, and 2 (11.1%) of them required prompt repeat surgery. In 2 cases, reoperation was performed after IDS, but this was considered to not be directly related to HIPEC.
As a triage strategy for the response after NAC and residual disease on IDS in patients with advanced-stage ovarian cancer, IDS followed by HIPEC as a first-line treatment according to our institution's management protocol seems to have had little effect on the safety and postoperative complications. In patients with a good response after NAC, tumor burden and extensive IDS procedures are reduced. Therefore, NAC can reduce the adverse effects and postoperative complications of IDS followed by HIPEC. In patients with poor response to NAC, the effect of HIPEC can alter responsiveness to platinum-based chemotherapy. Hettinga et al. [10] investigated the mechanism underlying the interaction between the effects of hyperthermia and chemotherapy cytotoxicity in cisplatin-sensitive and cisplatin-resistant cell lines. At a temperature of 43°C, the intracellular accumulation of cisplatin was shown to be higher in resistant lines than in sensitive lines [10]. Another possible explanation is that hyperthermia leads to the activation of heat-shock proteins, which, in turn, modify multiple cellular functions through their interference with protein folding. It is known that neoplastic cells express higher amounts of heat-shock proteins, therefore, becoming more susceptible to the effect of increased temperature [11].
Several studies have shown that the combination of IDS with HIPEC for the treatment of ovarian cancer is feasible and reasonably well-tolerated [121314]. Recently, a phase 3 clinical trial demonstrated that performing IDS followed by HIPEC improved survival outcomes among patients who had received NAC for stage III epithelial ovarian cancer. The patients who had, at least, stable disease after 3 cycles of NAC were randomly assigned to undergo IDS with or without the incorporation of HIPEC with cisplatin. The incorporation of HIPEC resulted in a longer recurrence-free survival and OS compared to IDS alone and did not result in higher rates of postoperative complications.
Specific drug toxicity is frequently associated with surgical toxicity in HIPEC; however, paclitaxel did not appear to cause any major toxicity compared to other drugs used in HIPEC. Paclitaxel has a high molecular weight and is highly metabolized by the liver; thus, it is associated with very low rates of systemic toxicity and is less likely to penetrate the peritoneum. Cascales-Campos et al. [15] reported that patients with stage III/IV ovarian cancer treated with IDS and HIPEC after NAC using paclitaxel had better survival outcomes than those treated with IDS without HIPEC; the results of disease-free survival (DFS) were significantly better in the group of patients treated with HIPEC. Bae et al. [16] demonstrated, in patients with advanced-stage ovarian cancer, a significant improvement in survival for the group treated with HIPEC using paclitaxel or carboplatin; in this study, DFS rates at 3 years were 56.3% in the HIPEC group and 16.7% in the control group (without HIPEC). Furthermore, the 5-year survival rates were 84.6% in the paclitaxel group, 63% in the carboplatin group, and 32.8% in the control group. HIPEC using paclitaxel, which was employed in this study, has been approved in South Korea as a new medical technology, and the Health Insurance Review & Assessment Service has approved paclitaxel-based HIPEC therapy since 2015 in Yonsei Cancer Hospital. Compared to paclitaxel, carboplatin in HIPEC has demonstrated no synergism with heat [17], and docetaxel in HIPEC occasionally exhibits greater activity and enhanced toxicity [18]. Cisplatin is commonly used in many HIPEC protocols at variable doses for the treatment of advanced-stage ovarian cancer [192021]. Nephrotoxicity and permanent renal dysfunction rarely occur in HIPEC with cisplatin [22]. In addition, Zanon et al. [23] reported a 6% incidence of nephrotoxicity in 30 patients with ovarian cancer using cisplatin with HIPEC.
Our study had some limitations. First, as a protocol-based pilot study, the number of patients analyzed was limited. In addition, the median survival was not reached, making the short follow-up period another limitation of the study.
We believe that incorporation of HIPEC in IDS will be not beneficial for all ovarian cancer patients. In this study, we applied HIPEC on the basis of the study protocol. Patients with complete remission after NAC were considered good responders, and some patients had no gross residual tumor without surgery. We performed laparoscopy without HIPEC for those group and initiated adjuvant chemotherapy immediately postoperatively. It might be preferable to administer chemotherapy without interruption from debulking surgery. However, some patients who were considered poor responders showed stable disease or progression of disease even after NAC. Second-line chemotherapy without IDS is recommended for poor responder. When applying IDS in poor responders, very aggressive surgery is required and optimal cytoreduction is difficult to achieve because of the tumor burden. We did not administer HIPEC to patients with unsuitable operative findings (suboptimal cytoreduction, excessive bleeding) and a poor performance status. Therefore, we applied IDS followed by HIPEC in a small population in which partial remission occurs after NAC and optimal debulking through IDS is achieved. These subgroups should be considered as the inclusion criteria for future clinical trials to determine the true benefit of IDS with HIPEC for ovarian cancer.
In conclusion, our results show that the incorporation of IDS followed by HIPEC according to our institution's management protocol seems to be feasible and safe for the treatment of ovarian cancer patients. Further evaluations of this protocol are required to assess its survival benefits. Additional larger trials are needed to determine if IDS with HIPEC has survival benefits as first-line treatment. A multicenter prospective study on the addition of HIPEC to IDS (KGOG 3042) is underway and its results could clarify the role of HIPEC in first-line treatment.
 XML Download
XML Download