

 PDF
PDF Citation
Citation Print
Print



Introduction
Epithelial ovarian cancer (EOC) is one of the most frequent malignancies in females and is the most fatal disease of gynecologic malignancy. In the United States, EOC accounts for 3% of all cancers in women, but is the cause of 5% of cancer deaths [1]. Worldwide, ovarian cancer was the seventh most common cancer and the eighth leading cause of cancer-related death in 2012, with 238,700 cases and 151,900 deaths occurring, respectively [2].
Currently, over 60% of all cancers in the United States are diagnosed in population older than 65 years, and by 2030, the percentage of all cancers diagnosed in older populations (age ≥65) will increase from 61% to 70% [3]. This tendency is expected to be observed also in the EOC patients as our population ages and life-expectancy improves [45]. As a clinical prognostic factor, age at diagnosis has been investigated in many malignancies including breast cancer [6], gastric cancer [7], and well-differentiated thyroid cancer [8]. The prognostic significance of age at diagnosis also has been investigated in EOC patients [910111213].
EOC is primarily a disease diagnosed in postmenopausal women with a median age at diagnosis of 63 years [14] and, approximately 70% of EOC cases and 85% of cancer-related deaths of EOC patients occur after the age of 55 years [15]. The incidence of EOC increases with advancing age and reaches culmination at 80 to 84 years of age [1]. Along with these demographic characteristics, several studies indicate that old age has an adverse prognostic effect for EOC patients, and the poor prognosis of elderly EOC patients is associated with offensive tumoral biology and less aggressive cytoreductive surgery and adjuvant chemotherapy due to frailty of elderly patients [101213].
Elderly patients are characterized by tremendous heterogeneity in terms of health status including comorbidities, geriatric syndromes, functional status and nutritional status [16]. Therefore, the physiologic age from comprehensive geriatric assessment (CGA) is one of the important indicators that clinicians can provide for tailored cancer treatment [161718]. Recently, more and more treatment options have been available; the tailoring of cancer treatment based on the physiologic age is needed. Even though many studies have selected conventionally the age of 65 to 80 years as a demarcation for elderly patients in EOC, the optimal age cutoff representing a poor prognostic indicator with CGA was not evaluated [1718].
This study was conducted to estimate the optimal cutoff age with CGA that can be used as a prognostic and geriatric assessment indicator in EOC patients using homogeneous populations treated with standardized surgery and chemotherapy in a single institution. Furthermore, we validated the prognostic significance of the chosen cutoff age with propensity score-matching analysis and with a dataset of The Cancer Genome Atlas (TCGA) of serous EOC.
Materials and Methods
1. Patients and data collection
The present study was a retrospective analysis of data from a single institution, including 1,236 EOC patients of Samsung Medical Center in Seoul, Korea, from January 1997 to April 2015. This study included EOC patients who underwent primary surgery at our institution and who were diagnosed with a serous, mucinous, endometrioid, or clear cell histologic subtype. Patients with borderline histology, germ cell tumor, or a rare histology were excluded. All patients were subjected to similar surgical procedures, adjuvant treatment, and follow-up protocols. We collected data on patient demographics including age at diagnosis, cancer characteristics including International Federation of Gynecology and Obstetrics (FIGO) stage, tumor grade and histology, and tumor markers including cancer antigen (CA) 125 and CA 19-9 prior to treatment. Staging was performed according to the 2014 FIGO staging system, and stages were grouped into IIIB or less and IIIC or higher for subgroup analysis. Tumor grade and histology were determined according to the current World Health Organization classification.
Most patients underwent radical debulking surgery, consisting of salpingo-oophorectomy, ascitic fluid, or peritoneal washings for cytological examination, whereas lymph node and peritoneal biopsies were acquired as indicated after the manual exploration or inspection of the retroperitoneum and the abdominal cavity including the subdiaphragmic surfaces of the peritoneum. The amount of residual disease after surgery was recorded according to intraoperative assessment by the surgeons and was supplemented by postoperative computed tomography scans. Optimality was divided into ‘Suboptimal’ when grossly visible tumor was 1 cm or larger at the end of surgery or a ‘Optimal’ if visible tumor was less than 1 cm. Primary treatment modality and discontinuation of adjuvant chemotherapy were also analyzed.
For geriatric assessment; comorbidities, geriatric syndromes, functional status and nutritional status were analyzed on the basis of previous studies [1619]. For this analysis, we collected registered 10th revision of the International Classification of Diseases (ICD-10) codes which associated with comorbidities and geriatric syndromes using hospital disease registry. Comorbidities represented the diseases that the patient is currently receiving treatment for; including hypertension, diabetes mellitus, cardiovascular disease, cerebrovascular disease, liver disease, thyroid disease and other disease that require treatment, and the patients were divided into 2 groups; yes or no. Geriatric syndromes are clinical conditions that are almost exclusively observed in elderly; depression, delirium, dementia, deep vein thrombosis and osteoporosis were included in this study. To evaluate the nutritional status, body mass index (BMI, kg/m2) and albumin (g/dL) level at diagnosis were analyzed. The American Society of Anesthesiologists (ASA) score prior to surgery was used to evaluate functional status.
Overall survival (OS) was measured from the date of surgery to the time of death or, for living patients, to the date of last contact. Data for patients who had not had an event were censored as of the date of the final observation. This study was evaluated by the Institutional Review Board at the Samsung Medical Center, Seoul, Korea (IRB No. 2018-04-124).
2. Finding the age cutoff
Multivariate Cox regression analysis was conducted to identify the age cutoff and estimate its effects on OS adjusted for covariates (histology, grade, stage, optimality, and comorbidities), with age as a dichotomous categorical variable. The hazard ratios (HRs) and negative log p-values using all possible cutoffs of age were plotted. Furthermore, to determine whether the pattern of p-value differed by cell type, we plotted a graph for serous and non-serous patients with multivariate cox regression analysis was conducted using histology, grade, stage, optimality and comorbidities as covariates. We also plotted the p-values and chi square distribution of Pearson's χ2 test analysis using all possible cutoffs of age as a dichotomous variable according to geriatric syndromes.
To validate the optimal age cutoff as a clinical prognostic factor in ovarian cancer, additional cohort data from a TCGA dataset of serous EOC were analyzed. Clinical information from TCGA Data Portal (https://tcga-data.nci.nih.gov/docs/publications/tcga/) was obtained, and survival analysis and multivariate regression analysis were conducted for a total of 548 patients with EOC.
3. Matching analysis
To reduce the effects of selection bias and potential confounding in this retrospective cohort study, survival outcomes were compared between women aged <66 years and ≥66 years after 1:3 propensity score matching Cases were matched with the closest propensity patients aged <66 years according to stage, histology, grade, optimality, and primary treatment (performed with R using the MatchIt package; R Foundation, Vienna, Austria; http://www.R-project.org). The propensity scores were calculated using a multivariable logistic regression model based on factors that demonstrated significant differences between the 2 groups in the total cohort. Based on the propensity score, 160 patients who were aged 66 years or older were matched to 480 patients younger than 66 years.
4. Statistical analysis
Patient characteristics were compared using the χ2 test for categorical variables, whereas Student's t-test was employed for continuous variables. Survival curves were estimated by the Kaplan-Meier method according to age cutoff and compared using the log-rank test. All statistical analyses were two-tailed with a significance level set at 0.05 and were conducted using R 3.1.3 statistical software (R Foundation).
Results
1. Baseline characteristics
A total of 1,236 patients with EOC were included in the present study; their detailed clinical and histological characteristics are depicted in Supplementary Table 1. Mean age was 53.0±11.2 years, 772 patients (62.5%) were stage IIIC or higher, and most patients demonstrated a serous histologic subtype (71.6%) and grade 3 (64.6%). Optimal cytoreductive surgery was performed in 933 patients (75.5%), and 1,178 patients (95.3%) completed the appropriate adjuvant chemotherapy. The 373 patients (30.2%) had comorbidities and ASA score was 3 to 4 points in 49 patients (4%).
The age-specific clinicopathologic characteristics according to a cutoff of 66 years of age are described in Table 1; 1,067 patients (86.3%) were aged <66 years at diagnosis, whereas 169 patients (13.7%) were aged ≥66 years. The mean age of patients aged <66 years was 50.1±9.1 years; whereas the mean age of patients aged ≥66 years was 71.1±4.4 years. Comparisons of the baseline characteristics of the 2 age groups showed significant differences in the distribution of stage (p<0.001), histology (p<0.001), optimality (p<0.001), comorbidities (p<0.001), geriatric syndromes (p<0.001) and ASA score (p<0.001). Seventy-eight percent of the elderly group were stage IIIC or higher versus 60.0% of the younger women. Elderly patients were more often diagnosed with a serous subtype than patients younger than 66 years of age (90.5% vs. 68.6%; p<0.001). Although, there were no statistical difference between the 2 groups in primary treatment modality and chemotherapy discontinuation, elderly patients received less optimal cytoreductive surgery than patients younger than 66 years of age (59.2% vs. 78.1%; p<0.001). More elderly (≥66 years) individuals showed significantly higher ASA score (p<0.001) than younger patients, and there were significantly more patients with comorbidities in elderly than younger patients (47.9% vs. 27.4%; p<0.001). Furthermore, elderly patients (≥66 years) were more often diagnosed with geriatric syndromes than patients younger than 66 years of age (p<0.001). The plot of Pearson's χ2 test analysis with geriatric syndromes also showed significant p-values (above the red line) for age cutoffs 66 years of age (χ2=19.2, p<0.001) (Supplementary Fig. 1). Albumin level and BMI prior to treatment were similar in both groups. There were no statistical differences between the 2 groups with respect to preoperative CA-125 (p=0.608), but CA19-9 (p=0.016) levels were significantly lower in the ≥66 years age group. Clinical and histological features of EOC patients from the TCGA dataset of serous EOC are described in Supplementary Table 2, and there were no significant differences between the age groups.
Table 1
Clinical and histological characteristics of patients with EOC stratified according to age at diagnosis in Samsung Medical Center (Total=1,236)

2. Multivariate regression analysis to identify prognostic age cutoff
Multivariate analysis using stage, histology, grade, optimality and comorbidities as covariates and leaving age at diagnosis as a dichotomous variable was performed to identify the specific prognosticated age. Then, we plotted the p-values and HRs of Cox analysis using all possible cutoffs of age. The plot showed significant p values (above the red line) for age cutoffs between 54 and 67 years of age (Fig. 1A). Age cutoff of 66 years was shown to be the most significant for defining age with poor prognosis (HR=1.45; 95% confidence interval [CI]=1.04–2.03; p=0.027). Notably, this pattern was observed only in the serous histologic subgroup analysis compared with the non-serous subgroup (Fig. 2). Analysis of a TCGA dataset of serous EOC showed similar patterns (cutoff age=70 years; HR=1.60; 95% CI=1.22–2.09; p<0.001) (Supplementary Fig. 2A).
Fig. 1
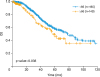
(A) HRs and p-values of Cox regression using age as a dichotomous cutoff of EOC patients in Samsung Medical Center. (B) Age-specific OS analysis with patients aged <66 years or ≥66 years.
EOC, epithelial ovarian cancer; HRs, hazard ratios; OS, overall survival.

Fig. 2
(A) HRs and p values of Cox regression analysis in serous histologic subtype using age as a dichotomous cutoff. (B) HRs and p values of Cox regression analysis in non-serous histologic subtype using age as a dichotomous cutoff.
HRs, hazard ratios.

Using the optimal age at diagnosis cutoff of 66 years, a Kaplan-Meier survival curve was depicted. Patients older than 66 years of age had significantly worse OS compared to younger individuals (56 months vs. 87 months; p=0.006; Fig. 1B), which was also shown in TCGA dataset analysis of the serous histologic cohort (35.8 months vs. 48.3 months; p=0.012; Supplementary Fig. 2B).
With the Cox proportional hazards model; advanced stage, optimal surgery and patients without comorbidities also remained independent prognostic factors for OS (HR=3.67; 95% CI=2.47–5.47; p<0.001, HR=0.67; 95% CI=0.52–0.86; p=0.002, and HR=0.68; 95% CI=0.5–0.91; p=0.01, respectively) in the multivariate analysis (Table 2).
Table 2
Multivariate analyses of survival outcome according to prognostic variables with EOC in Samsung Medical Center (n=1,236)

3. Comparison after propensity score matching
Following propensity score matching, patients were similarly distributed between groups, whereas comorbidities (p<0.001), geriatric syndromes (p=0.002) and ASA score (p<0.001) still showed statistically significant difference between 2 groups (Table 3). The median OS of patients aged older than 66 years was significantly lower than that of the younger group (57 vs. 78 months; p=0.038), showing the clinical significance of the chosen age cutoff (Fig. 3).
Table 3
Clinical and histological characteristics of patients with EOC stratified according to age at diagnosis following propensity scored matching (Total=640)

Discussion
In this study, we analyzed the survival outcomes of EOC patients according to age using pathologic characteristics, optimality and comorbidities as covariates, and identified the optimal age cutoff of 66 years as a prognostic indicator. This result was also observed in the serous histologic subgroup analysis. In addition, the prognostic significance of age cutoff of 66 years persisted in survival analysis following propensity score matching and validated with survival analysis using a TCGA dataset of serous EOC. These results indicate that 66 years of age can be the optimal cutoff for elderly in the prognostication of EOC, especially, serous histologic subtype. Consequently, we dichotomized patients aged <66 years or ≥66 years, and the baseline characteristics and geriatric assessment were compared between 2 groups. Elderly women had a significantly higher incidence of advanced stage and serous histology and were less optimally treated than younger patients; these findings indicated that aged older than 66 years tended to have more biologically aggressive disease. In addition, elderly women showed higher incidence of comorbidities and geriatric syndromes and high ASA scores, and these findings persist after propensity score matching analysis; these results indicated that elderly patients aged 66 years or older were facing a number of health problems which can complicate cancer treatment.
Many patients with EOC have poor prognosis, even though the current standard of care includes radical cytoreductive surgery and platinum-based adjuvant chemotherapy [120]. Notably, 37.6% of patients with EOC die within 2 years of diagnosis, while 31.0% of women diagnosed with EOC survive 10 years or longer [20]. Despite this wide range of survival times, little is known about the clinical characteristics predicting survival. Cress et al. [20] analyzed data from the California Cancer Registry and described clinical characteristics of long-term survival in EOC patients. Patients with low grade and low stage at diagnosis were more likely to be long-term survivors and had favorable prognosis with mucinous, clear, and endometrioid histology compared to serous subtype. These tumor characteristics were constant in subgroup analysis with early-stage EOC and closely correlated with each other [21]. The extents of residual disease after initial cytoreductive surgery and performance status were also important prognostic factors [121622]. In demographic analysis, endometriosis and menopausal hormone therapy may have a positive prognostic effect; meanwhile, older age, lower socioeconomic status, African ethnicity, and current smoking habit were associated with poorer survival outcomes [23].
Older age at diagnosis was reported to have an adverse effect on survival outcome and independent negative prognostic power in EOC patients [10111213]. Unfortunately, elderly patients with EOC will continue increase with the increase in life expectancy [145]. The European cancer survival data showed a steep decrease of survival in ovarian cancer patients with advancing age (70.9%; 95% CI=69.6–72.1 months at 15–44 years and 20.1%, 95% CI=19.2–21.1 months at ≥75 years) [24]. This tendency was also observed in a survival analysis of the California Cancer Registry [20]. These findings might be explained by the greater likelihood of elderly patients to have advanced-stage and higher-grade disease, which points to more aggressive biological behavior [11]. On the contrary, even though survival outcome adjusted for tumor characteristics, and treatment modalities including type of surgery and adjuvant chemotherapy, old age remained an independent negative prognostic factor itself [10]. These findings are consistent with our results and suggest that tumor biology or other unknown factors might be different between age groups.
Another explanation for the difference in survival of EOC patients by age is the use of less aggressive treatment in the face of older age. Aging is associated with a certain physiologic status including reduced stress tolerance, a decline in functional reserves of multiple organ systems, and a higher prevalence of comorbidity [25]. In this regard, the poor prognosis of elderly patients has been associated with lower rates of complete cytoreductive surgery and a high incidence of discontinuation of chemotherapy [101213]. Petignat et al. [10] dichotomized patients aged <70 years or ≥70 years and found that older women received less adequate primary cytoreductive surgery (20% vs. 43%) and less frequent aggressive chemotherapy (52% vs. 73%) compared with younger EOC patients, with a resultant negative impact on the prognosis of elderly patients. This tendency also observed in this study, a large number of elderly patients had significantly higher incidence of comorbidities, geriatric syndromes and high ASA score than younger patients. Although elderly patients showed no differences in primary treatment modality and chemotherapy discontinuation rate compared with the younger patients, they received significantly less adequate primary cytoreductive surgery than younger patients.
Ovarian cancer treatment in elderly women is not well-documented. Despite the increasing number of elderly cancer patients, treatment recommendations for this group are often inconsistent and quite different. Clinicians' barriers to cancer treatment of elderly, specifically clinicians' reasonable apprehension for comorbidities, and geriatric syndromes, have been noted as well. Despite this does not completely explain the tendency for clinicians to treat younger patients more intensively, cancer treatments, especially clinical trials, have been less conducted to this specific frailty population [2627]. Recent studies emphasize the importance of geriatric assessment to ensure the most adapted therapies in elderly patients [2428]. The GINECO and others have suggested that systemic treatments should be based not only on initial clinical evaluation, but also on geriatric assessment to reduce morbidity and toxic mortality and to improve OS [2930]. Furthermore, Girre et al. [31] reported that the conduct of a geriatric assessment led to the alteration of cancer treatment plans for over a third of the study population. However, geriatric assessment can be time consuming and labor intensive; in general, conducting geriatric assessment was not consistently applicate into real world cancer treatment [16]. Therefore, it is important to discover the possible candidate cutoff age to apply a CGA for elderly patients when considering efficiency. The results of our retrospective analysis can provide a potential candidate cutoff age 66 years to initiate geriatric assessment for elderly patients. With these efforts, elderly patients with EOC will be undertake better cancer treatments and these improve treatment outcomes in elderly patients.
There were some limitations in this retrospective study. First, age is considered a continuous variable, not a descriptive variable. Therefore, there will be several limitations in applying the optimal age cutoff to EOC patients in a real world cancer treatment. Second, information about comorbidities and geriatric syndromes was collected as ICD-10 code, which registered only in our hospital registry instead of medical chart review. Therefore, comorbidities and geriatric syndromes were often underreported and underestimation might cause bias of the results. Third, this study did not evaluate comorbidities and geriatric syndromes as each detailed subgroup. At last, we evaluated patients’ functional status with ASA score for anesthesiology, instead of Eastern Cooperative Oncology Group Performance status or Instrumental Activities of Daily Livingwhich generally used in geriatric assessment.
In conclusion, this retrospective analysis is a relatively large study that comprises almost 1,200 EOC patients including 169 elderly patients from a single institutional hospital. According to our results, the age cutoff 66 years may be the prognostic indicator and the optimal starting point for a CGA of EOC patients, especially in serous histologic subtype. Even though, there will be several limitations to employ our age cutoff because age is considered as continuous variable, this study may allow for the design of more weighted and evidence-based form of geriatric assessment for gynecologic oncologist in future research. Through our study, we not only proposed optimal age cutoff, but also highlighted the physiologic age to treat elderly EOC patients optimally. In order to improve the power of geriatric research and facilitate geriatric assessment, we must reduce heterogeneity of diverse geriatric assessment and develop more simple and formalized geriatric assessment tools. For this, multi-center prospective studies will be needed in a near future.
 XML Download
XML Download