

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Adult patients with cleft lip and palate (CLP) often present with maxillary hypoplasia,12 severe maxillary arch constriction,23 missing teeth,4 and periodontal disease.5 Selection of the optimal treatment method for such patients is a complicated process because palatal scar contractures and upper lip tension reduce postoperative stability in the case of large anteroposterior skeletal discrepancies.6 Maxillary expansion is a common treatment option for severe maxillary arch constriction7; however, sufficient maxillary arch expansion is difficult to achieve if the scar contracture is tough. In addition, this method can exacerbate gingival recession depending on the alveolar basal width and status of the periodontium.78 Maxillary arch expansion and prosthodontic treatment for missing teeth can be avoided in such cases by planning treatment in combination with orthognathic surgery.
Conventional Le Fort I osteotomy is a conventional and standard surgical procedure for the correction of maxillary hypoplasia in patients with CLP.9 However, the risk of relapse is high in patients with tough scar contractures,10 and maxillary advancement by distraction osteogenesis (DO) is now frequently indicated for the correction of maxillary hypoplasia in patients with CLP.111213 DO allows for progressive bone regeneration accompanied by more gradual soft tissue adaptation, which may lower the risk of relapse.14 This is crucial, particularly in the management of patients with CLP requiring excessive maxillary advancement, because of the increased soft tissue tension caused by scar contractures.15
Here we describe a case involving an adult patient with unilateral CLP (UCLP), severe occlusal collapse, and gingival recession who exhibited good treatment outcomes with long-term stability after multidisciplinary treatment involving maxillary DO and mandibular sagittal split ramus osteotomy (SSRO) following minimal maxillary arch expansion and leveling.
DIAGNOSIS AND ETIOLOGY
A 34-year-old woman with CLP on the left side was referred to our department with a chief complaint of dissatisfaction with the appearance of her face and teeth (Figure 1). The patient had congenital UCLP and had previously undergone surgeries at other institutions, including cheiloplasty at 6 and 8 months of age and palatoplasty at 1.2 years of age. Bone grafting had not been performed.
Extraoral examination revealed a concave facial profile with maxillary retrusion and mandibular protrusion. There was evident facial asymmetry with mandibular deviation to the right.
Intraoral examination showed a Class III molar relationship on both sides (Figure 1). The maxillary arch was remarkably constricted, with severe crowding and anterior and posterior crossbites. There was mild crowding in the mandibular arch with an accentuated curve of Spee. Alveolar defects with oronasal fistulae were present on the left side.
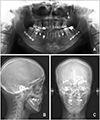
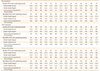
Clinical and panoramic radiographs demonstrated congenital absence of the maxillary left lateral incisor, maxillary left second molar, and mandibular right and left second premolars (Figures 1 and 2A). In addition, the maxillary left central incisor, maxillary right lateral incisor, and maxillary left and right second premolars showed extensive crown structure loss due to severe caries, and only root stumps were remaining. The maxillary right central incisor, left canine, and both first premolars also showed caries. The majority of teeth showed significant gingival recession (Table 1).
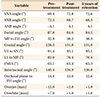
Lateral cephalometric analysis revealed an A point-nasion-B point (ANB) angle of −4.1°, sella-nasion-A point (SNA) angle of 68.4°, and sella-nasion-B point (SNB) angle of 72.5°. The maxillary and mandibular central incisors were retroclined (Figure 2B; Table 2). Posteroanterior cephalometric analysis showed right-sided mandibular deviation by approximately 4.0 mm at the mental spine (Figure 2C). The maxillary occlusal plane inclination was not observed.
TREATMENT OBJECTIVES
The patient was diagnosed with Angle Class III malocclusion with skeletal Class III facial asymmetry and left-sided CLP. The following treatment objectives were developed on the basis of the diagnostic records and patient consultation: reconstruction of the left-sided alveolar defects by bone grafting; extraction of the maxillary right lateral incisor and both maxillary second premolars; alignment using light continuous force for minimum expansion, with full consideration of the gingival recession; correction of the maxillary retrusion using maxillary DO; correction of the mandibular protrusion and deviation using SSRO; establishment of stable, functional occlusion; and periodontal reconstructive surgery for the exposed roots.
TREATMENT ALTERNATIVES
We considered three strategies for orthodontic alignment of the maxillary arch and orthognathic surgery. The first one involved extraction of the maxillary right lateral incisor and both second premolars, alignment by minimum expansion of the maxillary arch, maxillary advancement by DO for correction of the maxillary retrusion, and mandibular setback by SSRO for correction of the mandibular protrusion and deviation. The second one involved extraction of both maxillary second premolars, slow maxillary expansion with space regaining and prosthetic treatment for the maxillary right lateral incisor, and two-jaw surgery (Le Fort I + SSRO) for correction of the maxillary retrusion, mandibular protrusion, and mandibular deviation. The last strategy involved the extraction of both maxillary second premolars, maxillary expansion by surgically-assisted rapid palatal expansion (SARPE), correction of the maxillary retrusion and overjet by DO, space regaining and prosthetic treatment for the maxillary right lateral incisor, and correction of the mandibular retrusion and deviation by SSRO.
Adequate maxillary arch expansion was considered difficult because of severe scar contraction. Moreover, almost all teeth showed significant gingival recession, which could be exacerbated by lateral maxillary arch expansion. In addition, maxillary advancement by Le Fort I surgery or a combination of maxillary DO and SARPE was likely to worsen her speech function by reducing the area of the palate. After considering these factors, we finalized on the first strategy and accordingly initiated the treatment.
TREATMENT PROGRESS AND DISTRACTION PROCEDURE
We first extracted both maxillary second premolars and treated the caries in the maxillary right central incisor and first premolar; maxillary left central incisor, canine, first premolar, and first molar; mandibular left canine, first premolar, first molar, and second molar; and mandibular right canine, first premolar, and first molar. Then, we performed bone grafting in the left cleft region using cancellous bone harvested from the patient's left iliac crest. Orthodontic treatment was initiated 1 year after the bone grafting procedure (i.e., treatment time [TT]: 0 years, 0 months). A 0.018 × 0.025-inch pre-adjusted edgewise appliance (Dentsply-Sankin, Tokyo, Japan) was placed on the entire mandibular arch, and 0.014-inch nickel–titanium (Ni-Ti) (Sentalloy™, Tomy, Tokyo, Japan) and 0.016 × 0.022-inch improved superelastic Ni-Ti (L&H; Tomy) wires were used for initial leveling. After alignment of the mandibular teeth for 8 months (TT: 0 years, 8 months), a transpalatal arch was placed for 6 months (TT: 1 year, 2 months) in order to expand the molar region; however, no effective expansion was detected. We therefore changed the treatment plan to include SARPE. At that time, the treatment was discontinued for 1 year so that the patient could make a decision regarding further treatment. Meanwhile, the patient's speech function was evaluated by an ear–nose–throat (ENT) specialist, who suggested that SARPE could result in deterioration of her speech function. We therefore decided to continue her treatment without SARPE. After extraction of the maxillary right lateral incisor (TT: 2 years, 6 months), the maxillary teeth were aligned using a 0.018 × 0.025-inch pre-adjusted edgewise appliance placed on the entire maxillary arch (TT: 2 years, 7 months); 0.014-inch and 0.016-inch Ni-Ti wires and a 0.016 × 0.022-inch improved superelastic Ni-Ti wire were used for leveling, which took 15 months (TT: 3 years, 11 months). Subsequently, maxillary DO was performed for correction of the maxillary retrusion (Figures 3 and 4). Le Fort I osteotomy, including separation of the pterygomaxillary junction, was performed. Internal distractors (Zurich Paediatric Distractor®, 15-mm model; KLS Martin, Tuttlingen, Germany) were bilaterally fixed to the zygomatic buttress according to a surgical acrylic guide for distractor positioning. The distraction vector was set at 25.0° to the Frankfurt horizontal (FH) plane on the basis of a previous study at our facility16; this would ensure correction of the anteroposterior and vertical maxillary deficiencies. The distractors were intraoperatively activated for confirmation of their function and mobility of the maxilla. After a latency period of 6 days, distraction was initiated at the rate of 1.0 mm once a day, with an initial advancement amount of 10.3 mm over 12 days. With regard to the amount of maxillary advancement, we planned to extend as much as possible under close monitoring of her speech function. However, her speech function deteriorated with an extension of 10 mm, so the procedure was terminated. The actual amount of advancement at the anterior nasal spine was 6.5 mm. We built up the occlusal surface of the mandibular left first molar with resin in order to prevent left and right maxillary occlusal plane inclination after DO (Figures 3B and 4B). The distracters were surgically removed and SSRO was performed 5 months after DO (TT: 4 years, 5 months). We planned 5.0 mm of mandibular advancement on the right side and 7.0 mm of setback on the left side. A 15.0-mm bone defect was observed in the maxillary left molar extension bone after distractor removal; therefore, we fixed a mini-plate on the left side only. The preadjusted edgewise appliances were removed 13 months after SSRO. Arch co-ordination and interdigitation were also completed at that time. After removal of the edgewise appliances, a Hawley retainer and canine-to-canine fixed retainer were delivered for the maxillary and mandibular arches, respectively. The total treatment duration was 5 years and 6 months. The maxillary left central incisor, maxillary right canine and first molar, and mandibular left first premolar and first and second molars were restored at the start of the retention phase.
RESULTS
The patient's post-treatment records demonstrated a balanced facial profile and occlusion with improved facial symmetry (Figures 5, 6, 7). Her profile was dramatically improved, with reduced upper lip retrusion and lower lip protrusion as a result of the maxillary advancement and mandibular setback, respectively. Intraoral photographs showed satisfactory occlusion with adequate overjet and overbite and coincident midlines (Figure 5). The patient's speech function was re-evaluated by ENT specialists, who found no major changes. Gingival recession was slightly increased, but tooth mobility was within the normal physiological range (Table 1). No tooth hyperesthesia was observed after treatment. The patient was not willing to undergo any periodontal reconstructive surgery, so we referred her for follow-up to a periodontist. Post-treatment cephalometric analysis and computed tomography images showed an increased SNA angle (72.8°), a decreased SNB angle (68.7°), and an increased ANB angle (4.1°; Figures 6, 7, 8; Table 2). The amount of advancement at the anterior nasal spine was 6.0 mm. With regard to the maxillary anterior tooth axis, the upper incisor to sella-nasion axis changed from 91.4° to 95.1°. Posteroanterior cephalometric analysis revealed a decrease in the amount of mandibular deviation at the mental spine from 4.0 mm to 2.0 mm. The post-treatment panoramic radiograph showed good root alignment. There was no discernible bone loss or root resorption, with no apparent post-treatment changes in either occlusion or the alveolar bone height in the grafted areas.
DISCUSSION
In the present case, we successfully achieved long-term stability after multidisciplinary treatment involving maxillary DO and SSRO for UCLP with severe occlusal collapse and gingival recession.
Patients with CLP often have a narrow maxillary arch as a result of the scar3; this is generally treated by rapid palatal expansion or slow expansion.7 We initially attempted slow expansion for our patient, although this was ineffective because of the tough scar contracture. In addition, the patient had significant gingival recession, numerous root stumps as a consequence of extensive caries, and missing teeth. Therefore, we decided to minimize the expansion and perform orthognathic surgery. The disadvantage of treatment without sufficient maxillary expansion is the need for increased forward movement of the maxilla or backward movement of the mandible during orthognathic surgery in order to adjust the widths of the maxillary and mandibular arches. Considering the need for increased forward movement of the maxilla, we opted for DO.
Our strategy of minimal maxillary arch expansion resulted in expansion of 0.2 mm in the canine region and 0.8 mm in the first molar region. This was lesser than the amount of expansion required for patients with UCLP (maxillary premolar: 5.3 ± 4.0 mm, maxillary molars: 1.6 ± 3.8 mm) in a previous study.17 However, the relationship between lateral expansion in orthodontic treatment and gingival recession remains controversial,781819 although minimizing the amount of expansion is thought to inhibit treatment-related progression of gingival recession.
Maxillary advancement is the most common surgical technique for the correction of maxillary hypoplasia in patients with CLP. Maxillary DO is a frequently used technique that may lower the risk of relapse,14 allow expansion of the associated soft tissues, and minimize the resistance from muscles, ligaments, and the skin, which may be responsible for relapse.614 Long-term skeletal stability after maxillary advancement by DO was crucial for our patient. A previous study found that the relapse rate after a 5-year follow-up period was lower for patients treated with DO than for those treated with conventional orthognathic surgery (8.2% vs. 37%).20 Moreover, the use of an intraoral distractor (such as the Zurich maxillary distractor used in the present case) instead of an extraoral distractor provides long-term skeletal stability despite the small amount of extension.21 The rate of relapse when intraoral distractors were used has been reported to be < 10%.62022 The relapse rate for our patient was 7.7% (0.5 mm/6.5 mm) at 5 years after DO; this was less than previously reported rates.
Placement of an external distractor such as the RED system is easy and allows adaptation of the distraction vector throughout the distraction period. However, despite the advantages and success of external distraction devices, the use of an internal distractor for DO reduces the physical and psychological stresses on the patient and shortens the length of hospitalization.15232425 All maxillary DO procedures are therefore performed using internal distractors at our facility. Using the Zurich maxillary distractor, we achieved 10.3 mm of extension on both sides in the present case. The actual amount of advancement at the anterior nasal spine was 6.5 mm, which accounted for approximately 63.1% of the activation distance. The reported distraction ratio achieved with the use of Zurich maxillary distractors at our facility ranged from 51.1% to 95.9% (mean, 69.5%).16 During our patient's first visit, severe scar contraction with significant maxillary arch constriction and severe crowding of the maxillary teeth were observed. Thus, the extension efficiency was considered to be lower because of the strong soft tissue tension caused by the scar contracture, and the distraction ratio was slightly lower than the average value for our facility.
The disadvantages of an internal distractor include difficulty in positioning, less flexibility of the vector control, and reduced advancement.262728 Furthermore, it has been reported that internal distractors may rotate in a clockwise direction during the distraction period.22 A previous study at our facility noted that the change in the placement angle of the distractors relative to the FH plane was 7.7°, while the angle of the actual advanced vector at the anterior nasal spine relative to the FH plane was 9.7° less than the planned vector. Furthermore, the mandible showed clockwise rotation by 3.5°.16 Similar observations were made in the current case; the angular change of the distractors was 6.0°, the actual advanced vector at the anterior nasal spine was 4.0° less than the planned vector, and the mandible showed clockwise rotation of 0.5°. These results indicate that the maxilla was advanced inferior to the planned vector, with slight clockwise rotation, during the distraction period. Clinicians should consider this aspect at the time of preparing a surgical plan involving the use of internal distractors.
In summary, we believe that long-term stability after maxillary DO in the present case was achieved with the use of SSRO without excessive forward movement of the maxilla and by consideration of the limitations of internal devices at the time of planning the treatment strategy for maxillary advancement.
CONCLUSION
In conclusion, the findings from the present case suggest that a multidisciplinary treatment approach involving a combination of minimum maxillary arch expansion, maxillary advancement by DO, and mandibular setback by SSRO, with consideration of strong scar contraction and gingival recession, is an effective strategy for the treatment of patients with UCLP with maxillary hypoplasia, severe maxillary arch constriction, severe occlusal collapse, and gingival recession. Such approaches can improve occlusion and facial esthetics without the need for prostheses such as dental implants or bridges, and the outcomes tend to remain stable in the long term after treatment.










 XML Download
XML Download