

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Prosthodontic restoration plans to guide the locations of dental implants are utterly important.1 Inadequate implant placement makes the restorative procedure difficult. Fabricating prosthesis is sometimes impossible for a misplaced implant, and removing the implant is considered.2 The prosthodontic procedures without the removal of implant lead to undesired outcomes biomechanically and aesthetically.
There are many possible reasons for implant misplacement, one of which appears to be that the precise implant placement directly depends on the amount of bone at the planned site.3 There are several studies trying to find some factors affecting implant prognosis and survival.4,5,6 Such studies generally used the logistic regression methods or other traditional tools to infer the factors statistically.7 Regression models evaluate the influences of the factors on the implant survival, including the age, installed site, and bone quality, which are the variables already planned to be investigated. However, modern data mining tools including machine learning methods are considered necessary in analyzing the effects of the various variables associated with the implant surgery, which include mesio-distal position, bucco-lingual angulation, and the depth of an implant. Two advantages of these machine learning methods are to precisely analyze the data of a small sample size and to detect a new factor affecting the results.8 Those two features are the requirements that many clinical studies need in the field of dentistry, the sample size of which is usually small.
The decision tree, one of the machine learning methods, is often used for classification and prediction and consists of a root node on the top, internal nodes for grouping criteria, links for nodes, and leaves as the final classification using a recursive partitioning method. A decision tree is appropriate for discovering patterns from binomial data with a learning binomial function.9 Many researchers in medical science are currently applying the decision tree model in diverse fields.10,11
The support vector machine is a supervised learning method used to determine the decision surface with the best classification of data.12 This method showed at least equal or better performance to that of other classification methods such as Bayesian classifier or artificial neural network.13 Medical researchers use support vector machines in various research areas, such as diagnosing Alzheimer's disease through single-photon emission computed tomography image classification, discriminating breast cancer patients from a control group based on nucleosides in urine samples, and prognosis of drugs for heart failure patients.14,15,16 However, support vector machines have not been used in the field of prosthodontics.
This study tried to find the determinant location factors of an inserted implant, which influences implant survival or complication. Additionally, both the decision tree and the support vector machine investigated whether there was a new factor affecting the implant prognosis.
Go to : 
MATERIALS AND METHODS
The data were collected from the retrospective chart review and filtered very carefully at at Seoul National University Bundang Hospital for one year (IRB No. B-0602-030-016). Subjects included in the analysis were partially edentulous patients who wanted their consecutively missing teeth to be restored by implants, having the implants placed without surgical stents. The patients having well-controlled hypertension or diabetes were included. However, smokers and patients with any other systemic disease that was likely to compromise implant survival were excluded.17,18
After consulting with a prosthodontist about implant location, all operations included in this study were performed by a maxillofacial surgeon with the same surgical protocol. The surgeon placed 667 implants in the mouths of 198 patients according to the anatomic guide structures. Two dental implant systems (Osstem, Osstem Co., Busan, Korea, and Implantium, Dentium Co., Yongin, Korea) were used. All subsequent prosthodontic procedures were similarly performed by a prosthodontist. The problems that were confronted during the prosthodontic procedure were assessed and the final prostheses were evaluated by the prosthodontist. A year after prosthodontic restoration, the prosthodontist evaluated the implant's location, features, and biomechanical aspects with relation to the outcome.
The prosthodontic evaluations were categorized into cases according to the chart records. If a patient had several implants, more than one case could exist. The authors processed the descriptive evaluations into several features designated in nominal form for the analysis. During this process, some cases that lacked sufficient information for evaluation were excluded. Therefore, a total of 53 patients and 59 cases were analyzed, and the machine learning method was applied because of the small sample size.
The features consisted of explanatory variables and output variables. The explanatory variables were divided into controllable variables, which could be managed by dentists, and host variables (Table 1 and Table 2). As explained above, these variables had nominal values. In Table 1, for example, the ‘immediate implantation’ variable has ‘Yes’ or ‘No’, and the other variables have ‘Adequate’ or ‘Inadequate’. In Table 2, the ‘site of placement’ variable has ‘Maxilla’, ‘Mandible’, or ‘Both’, and the ‘posterior site of placement’ variable has ‘premolar’, ‘molar’, or ‘both’.
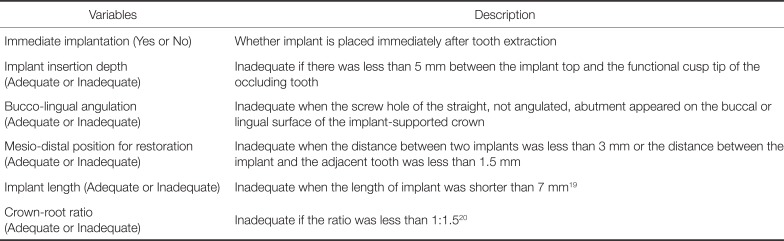
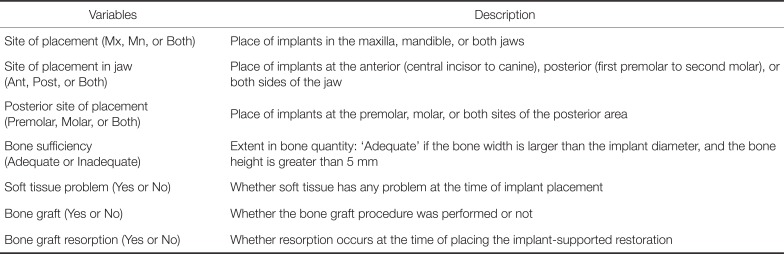
Table 1
Controllable variables
| Variables | Description |
|---|---|
| Immediate implantation (Yes or No) | Whether implant is placed immediately after tooth extraction |
| Implant insertion depth (Adequate or Inadequate) | Inadequate if there was less than 5 mm between the implant top and the functional cusp tip of the occluding tooth |
| Bucco-lingual angulation (Adequate or Inadequate) | Inadequate when the screw hole of the straight, not angulated, abutment appeared on the buccal or lingual surface of the implant-supported crown |
| Mesio-distal position for restoration (Adequate or Inadequate) | Inadequate when the distance between two implants was less than 3 mm or the distance between the implant and the adjacent tooth was less than 1.5 mm |
| Implant length (Adequate or Inadequate) | Inadequate when the length of implant was shorter than 7 mm19 |
| Crown-root ratio (Adequate or Inadequate) | Inadequate if the ratio was less than 1:1.520 |
![]()
Table 2
Host variables
![]()
There were two kinds of output variables: the first was the survival of the implant, evaluated as whether the implant was osseointegrated or not; and the second was complications of the implant, evaluated as any discomfort or defect despite of adequate function with osseointegration (Table 3). The result variable has one of ‘Survival’ and ‘Osseo-disintegration’. The complication variable has one of ‘None’, ‘Thread/Implant exposure’, ‘Screw loosening’, ‘Loading problem’, and ‘Others’.
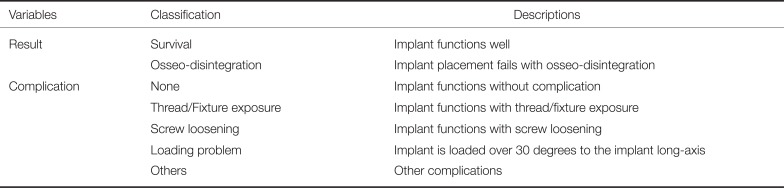
Table 3
Output variables
![]()
All the features had nominal values in this study. Therefore, we selected a decision tree model among many available machine learning methods. Also, we used the support vector machine since this method is widely utilized in various fields including medical science. The authors trained and tested the decision tree using the collected data. Learning and classification of the factors affecting survival and complication were accomplished for the decision tree model analysis, using WEKA (Waikato Environment for Knowledge Analysis, University of Waikato, Hamilton, New Zealand) - Java based machine learning software. All possible combinations of features were made for the support vector machine. For each combination of features, cross validation was performed on the support vector machine. Linear function was used for classification by the support vector machine. The evaluation of support vector machine classification by machine learning was carried out by leave-on-out-cross-validation (LOOCV), which classified one sample with machine learning that was trained using the other 58 samples. The accuracy, defined as true positive and negative over the whole sample, was calculated with the confusion matrix.
Go to :
RESULTS
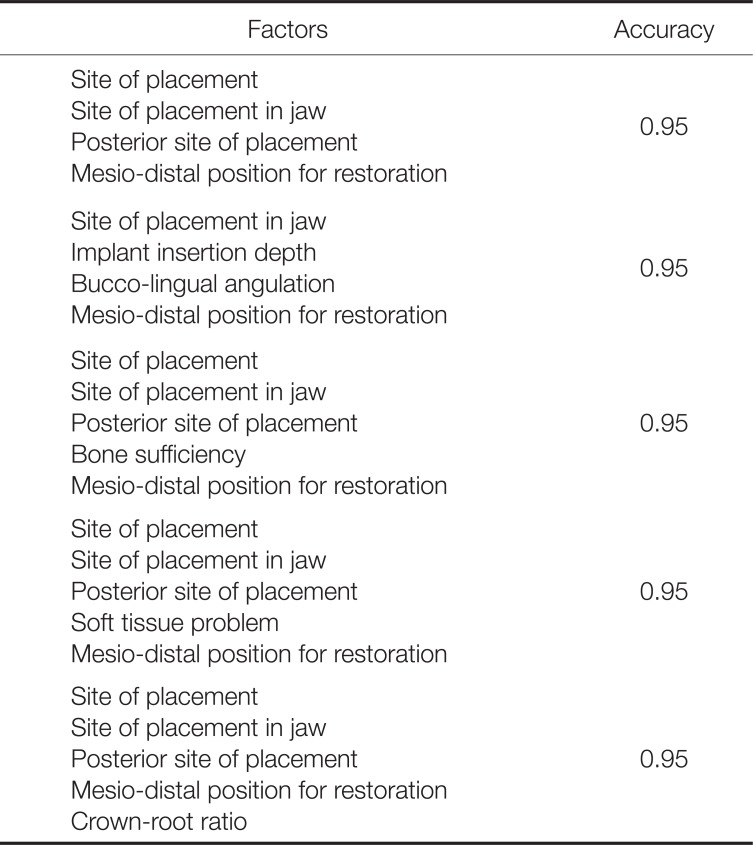
The decision tree model for implant survival is presented in Fig. 1. The mesio-distal position was the most significant factor determining implant prognosis (accuracy = 0.93). The decision tree model for complications of implant is shown in Fig. 2. Thread/fixture exposure appeared when the implant was placed with bone graft even when the implants were placed adequately (accuracy = 0.64). Support vector machine with LOOCV - survival measure of implant is presented in Table 4. Support vector machine with LOOCV - complication measure of implant is shown in Table 5.
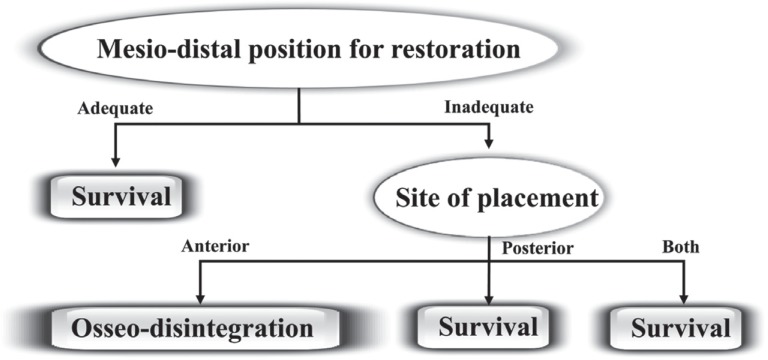 | Fig. 1The decision tree model for implant survival. The mesio-distal position is the most significant factor determining implant prognosis (accuracy = 0.93).
|
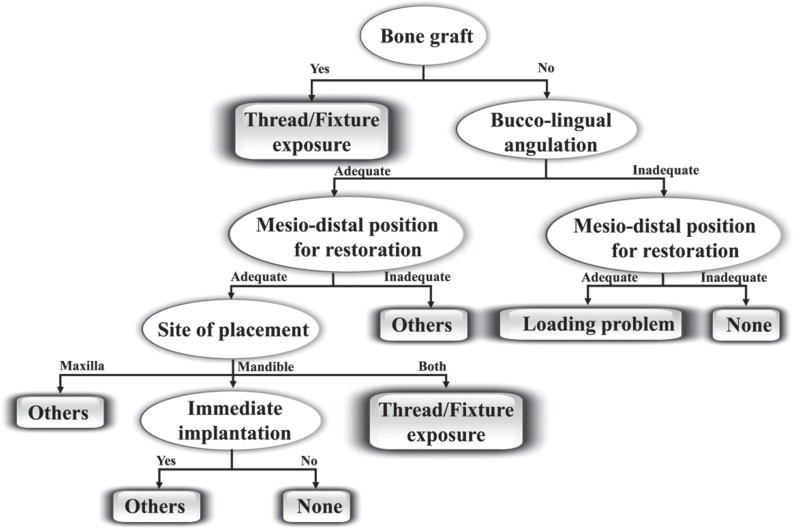 | Fig. 2The decision tree model for complications of implant. Thread/fixture exposure appeared when the implant was placed with the bone graft even when the implants were placed adequately (accuracy = 0.64).
|
Table 4
Support vector machine with LOOCV - survival measure of implant (top 5 results)
![]()
Table 5
Support vector machine with LOOCV - complication measure of implant (top 5 results)
![]()
Go to :
DISCUSSION
First, both the decision tree model and support vector machine clearly identified ‘mesio-distal position’ as the most important factor during implant treatment. Both complication and survival of implant were associated with this factor in the decision tree model and most sets of the support vector machine also included this factor.
The decision tree model showed that the implant functions successfully without osseo-disintegration when placed appropriately in the mesio-distal position. Even when this condition was inappropriate, there was no problem unless the placement was in the anterior part of jaw. According to features of the decision tree model, the mesio-distal position variables potentially affected the survival of the implant to a greater extent because they were located in the root of the tree (Fig. 1, accuracy = 0.93).
Regarding complications, noticeable thread exposure appeared when the implant was placed with bone graft. Thread/fixture exposure occurred even when the implants were placed with the appropriate bucco-lingual angulation and mesio-distal position in the maxilla and mandible. This result indicated that there was thread exposure even with adequate bucco-lingual angulation of the implant axis. In addition, loading problems occurred if the implant was placed without bone graft, inappropriate bucco-lingual angulation, and appropriate mesio-distal position. This loading problem led to non-axial loading on the implant (Fig. 2, accuracy = 0.64).
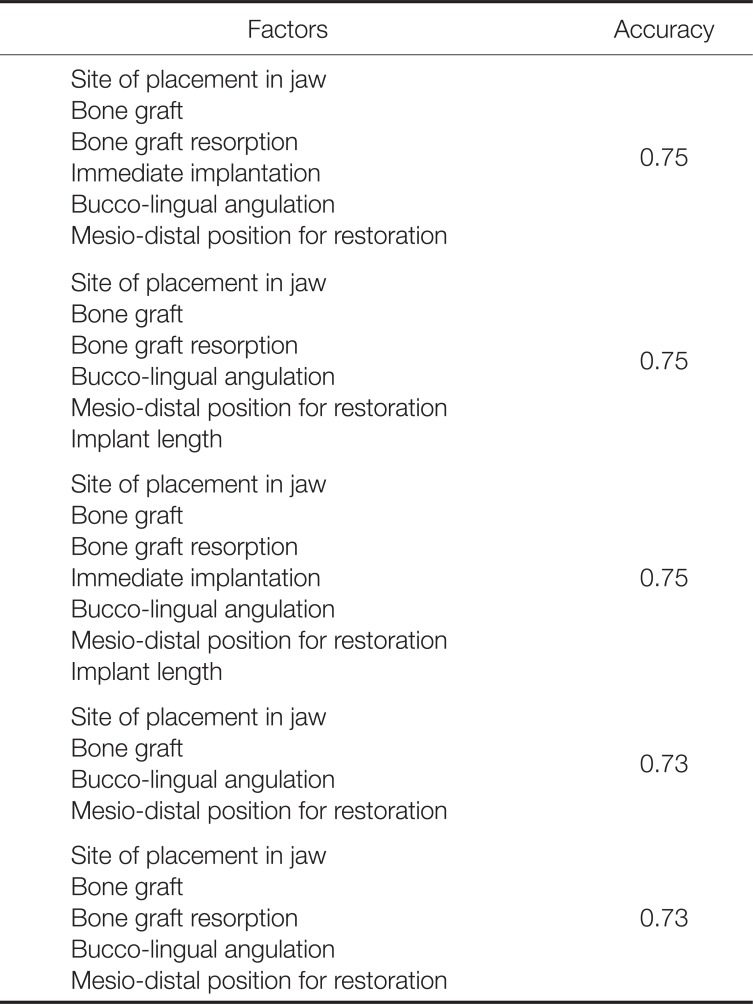
Support vector machine with LOOCV showed outstanding performance in linear kernel function (Table 4, Table 5). In the survival measure, two sets with only four features were sufficient to classify the result of the implant with high accuracy (0.95). One of the sets consisted of the following features: site of placement-maxilla or mandible; site of placement in jaw-anterior, posterior, or both; posterior site of placement; and mesio-distal position for restoration. The other set included the following: site of placement in jaw-anterior, posterior, or both; implant insertion depth; bucco-lingual angulation; and mesio-distal position for restoration. Interestingly, all of the sets had one common feature, mesio-distal position for restoration (Table 4). As Bryant (1998) found, most sets showed that the site of placement, whether it is on the maxilla or mandible, was important.4
Regarding complication of implants, the support vector machine indicated that six factors were important in order to predict the prognosis with the best accuracy (0.746). All sets commonly included the following four factors: site of placement in jaw-anterior, posterior, or both; bone graft; bucco-lingual angulation; and mesio-distal position for restoration. The other factors in these sets were bone graft resorption, immediate implantation, and implant length.
In the present study, the machine learning method was selected for analysis.9,19 This term was first used in the literature by Samuel, who proposed a learning game through alternating features and weighted values.20 Thereafter, the machine learning method integrated with computation theory was studied as a new research area in the 1980s. Document classification, information searching, and various other areas utilize machine learning methods.21,22
Many practitioners have realized how agonizing it is to encounter unexpected situations during implant placement. We also know how important it is to reach consensus between surgical operation and biomechanical prosthetic rehabilitation. Knowledge of the factors primarily considered during the operation would be very valuable for functional rehabilitation. Several factors have been proposed by other researchers, including quality and quantity of bone, history of trauma to the region, proximity of important structures (sinus, inferior alveolar nerve), need for bone grafting, degree of arterial blood supply, and rate of tissue healing.6 For implant fixture, a wider diameter and long length are known to be important factors for the survival of the implant.23,24 The shape of dental implants has been one of the most contested aspects and may have an effect on implant biomechanics.25
It has been demonstrated that bone loss of 1.5 to 2 mm apical to the implant-abutment junction would occur after uncovering surgery.26 Moreover, it has been documented that this bone loss could result in less inter-implant crestal bone loss if inter-implant distance is greater than 3 mm.27 Therefore, it has been suggested that two implants must be spaced more than 3 mm apart.27 It is commonly observed that it is more difficult to increase inter-implant distance at the anterior than posterior. This results from differences in mesio-distal width of the crowns at the anterior and posterior. Therefore, the residual bone must be carefully studied to place implant fixtures in mesio-distally correct positions for anterior implants. It will ensure at least 3 mm of the inter-implant distance. Moreover, it may indicate that wider diameter implants may be of limited use in the anterior.
Go to :
CONCLUSION
Adequate mesio-distal positioning of the implant significantly affected the implant prognosis. Thus, site of placement was the most critical feature in this pilot study, as also indicated in other research. The small sample size demonstrated the strength of the machine learning method. However, traditional statistical tools should be applied with large samples to verify our conclusion.
Go to :
 XML Download
XML Download