

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Kawasaki disease (KD) is an acute febrile illness of unknown etiology that affects predominantly children aged <5 years of age.1) KD is currently the most common cause of acquired heart disease in children in developed countries.1) Currently, there is no definitive diagnostic test for KD. A KD diagnosis is based on clinical criteria including ≥5 days of fever and the presence of at least four of the five principal clinical features (oropharyngeal changes, bilateral conjunctival injection without exudates; polymorphous rash, changes of the extremities, and cervical lymphadenopathy).1)
Redness or crust formation at the Bacille Calmette-Guérin (BCG) inoculation site is reported in about 30–50% of all KD patients.23) However, it is observed in ≥50% of KD patients at 1 to 12 months after inoculation.24) The BCG site reaction is a useful diagnostic finding especially in children with incomplete presentation of illness.2345) The BCG site reaction has been regarded as one type of skin rash of KD by some authors.6) Comprehensive reports investigating the clinical characteristics of KD patients manifesting the BCG site reaction are rare.78)
The purpose of this study was to investigate the significance of the BCG site reaction as a diagnostic clinical finding and an outcome predictor in young children with KD.
MATERIALS AND METHODS
1. Subjects
Among 1,090 patients who were admitted to the Asan Medical Center for management of acute illness between January 2006 and February 2017, 41 transferred patients without data related to BCG site status or principal clinical features and 1 patient without BCG vaccination were excluded. Age-specific incidence of the BCG site reaction was analyzed in those 1,058 patients. Subsequently, patients aged less than 18 months were enrolled as subjects for the analysis of the association between the BCG site reaction and other laboratory and clinical findings. Subjects were divided into two groups according to the presence of the BCG site reaction in complete and incomplete KD separately.
This study was approved by the Institutional Review Board of Asan Medical Center (2018-0370), and the requirement for informed patient consent was waived.
2. Data acquisition
Demographic, clinical, laboratory, and coronary arterial diameter data were obtained via retrospective review of the medical records of subjects. Diagnosis of KD was made according to the American Heart Association criteria.1) Complete KD was defined as ≥5 days of fever and the presence of ≥4 of the 5 principal clinical features. Incomplete KD was defined by fever ≥5 days, 2 or 3 principal clinical features, and compatible laboratory or echocardiographic findings without other causal explanation for fever. Spontaneous improvement was defined as resolution of fever without intravenous immunoglobulin (IVIG) treatment. Refractory KD was defined as the requirement for 2nd line treatment to control persistent fever at 36 hours after 1st IVIG treatment. The BCG site reaction was defined as any redness or crust formation at BCG inoculation site recorded during admission.7)
Laboratory data included white blood cells, hemoglobin, platelet count, erythrocyte sedimentation rate, C-reactive protein, sodium, potassium, chloride, albumin, alanine aminotransferase, aspartate aminotransferase (AST), bilirubin, brain natriuretic-peptide, urine analysis.
A coronary artery diameter measured at subacute phase was converted to z score using the regression equation of McCrindle et el.9) A coronary artery aneurysm was defined as z score of any coronary arterial branch diameter ≥2.5.1) Pyuria was defined as ≥10 white blood cells per high power field in microscopic exam.
3. Statistical analysis
All the data were presented as mean±standard deviation or frequency (%) as appropriate. Continuous data between two groups was compared by t-test. χe test was used to compare frequencies between two groups and to analyze the altered rate of incidence of the BCG site reaction according to age. The association between the BCG site reaction and other variables was investigated separately in complete and incomplete KD groups via univariate logistic regression analysis. A multivariate analysis was performed with statistically significant variables in univariate analysis. To avoid collinearity between variables, we used body weight as the representative variable of body size in multivariate analysis. SPSS version 21.0 (IBM Co., Armonk, NY, USA) was used for all statistical analysis. Statistical significance was defined as a P-value <0.05.
RESULTS
1. The incidence rate of the BCG site reaction according to age
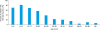
The proportions of patients with BCG site reaction in the respective age ranges were above 70% in age group under 18 months (Fig. 1). The incidence rate of the BCG site reaction was higher in patients in the age group 6–12 months than in the 0–6 months (P=0.017), and significantly decreased with increasing age (P<0.001) after 12 months. The 416 patients in the age range 0–18 months were enrolled in subsequent analyses.
2. Characteristics of subjects
The subjects included 313 patients with BCG site reaction and 103 patients without BCG site reaction (Table 1). Patients with the BCG site reaction had lower body index, fewer cervical lymphadenopathy, fewer changes in extremities and fewer spontaneous improvement. They also had lower hemoglobin level, higher AST, higher potassium level and more pyuria. Incidence of coronary aneurysm and z scores of three major coronary arteries were not different between two groups.
Table 1
Characteristics of subjects

Data are reported as mean±standard deviation or number (%).
Abbreviations: BCG, Bacille Calmette-Guérin; KD, Kawasaki disease; WBC, white blood cell; ESR, erythrocyte sedimentation rate; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LD, lactate dehydrogenase; BNP, brain natriuretic peptide; LMCA, left main coronary artery; LAD, left anterior descending; RCA, right coronary artery.
![]()
3. Correlation between the BCG site reaction and other variables in the complete KD groups
The univariate analysis of 322 subjects with complete KD showed that patients with the BCG site reaction had lower body index, fewer spontaneous improvement, lower hemoglobin level and more pyuria (Table 2). Other variables including age, principal clinical findings and the z scores of three major coronary arteries were not associated with the BCG site reaction. Among the significant variables in the univariate analysis, body weight (odds ratio [OR], 0.799; 95% confidence interval [CI], 0.697–0.916; P=0.001) and pyuria (OR, 2.124; 95% CI, 1.188–3.797; P=0.011) were still significant variables in the multivariate analysis.
Table 2
Logistic regression analysis of the Bacille Calmette-Guérin site reaction in 322 complete Kawasaki disease patients aged less than 18 months

Data are reported as mean±standard deviation or number (%).
Abbreviations: OR, odds ratio; CI, confidence interval.
![]()
4. Correlation between the BCG site reaction and other variables in the incomplete KD groups
In the univariate analysis of 94 subjects with incomplete KD, patients with the BCG site reaction had lower body index, higher serum total bilirubin level. The body weight (OR, 0.638; 95% CI, 0.440–0.926; P=0.018) remained a significant variable in the multivariate analysis (Table 3).
Table 3
Logistic regression analysis of the Bacille Calmette-Guérin site reaction in 94 incomplete Kawasaki disease patients aged less than 18 months

Data are reported as mean±standard deviation.
Abbreviations: OR, odds ratio; CI, confidence interval.
![]()
DISCUSSION
BCG vaccination for prevention of tuberculosis especially severe infection in children,10) is included in the national immunization program of South Korea.11) BCG vaccination has been recommended for newborn infants aged <1 month since 1966,12) and its coverage was nearly 100%.1113) There was only one excluded patient due to lack of vaccination in this study. Therefore, South Korea with the second highest incidence of KD worldwide,14) should be the most appropriate country to conduct any investigation into the BCG site reaction in KD.
It is well known that incidence of BCG site reaction decreases with age.27815) In this study, the incidence of BCG site reaction peaked at 6 months to 18 months and declined with age. Similar result was found by a study in Japan, where BCG vaccination has been recommended for infants aged <1 year. In a previous study in Japan, BCG site reaction peaked between 6 and 8 months and also decreased with age.2)
We selected patients aged below 18 months for satisfactory diagnostic sensitivity of investigation into the clinical significance of the BCG site reaction. First, an incidence rate of BCG site reaction was ≥70% in patients aged below 18 months, as shown in Fig. 1. Second, BCG site reaction is more frequent than cervical lymphadenopathy in that age group in our study. Third, in a previous study by Uehara et al.,2) they selected age group 3–20 months with incidence rate ≥70% for analysis of BCG site reaction. An additional purpose of the patient selection was to reduce the strong influence of age on the incidence rate.27815)
Due to the difference between complete KD and incomplete KD, we analyzed the association of the BCG site reaction with the other variables separately for complete and incomplete KD.
The multivariate logistic regression showed that body weight was associated with the BCG site reaction in both complete and incomplete KD groups. The higher body weight was related to a diminished likelihood of the BCG site reaction. First, we interpreted this relationship as a reflection of the time course of weight gain from growth after BCG vaccination. Second, it is well known that immune system of children is still in a course of development and immune system is closely related with the child's nutrition state. For children with higher body weight, the primary immune response to BCG strains may be more complete and faster and may reduce the chance of developing BCG site reaction in infants with KD. We cannot further explain the association of pyuria and the BCG site reaction in complete KD. No association between the BCG site reaction and coronary arterial lesions in this study is compatible with other published reports.237815) Therefore, outcome of KD patients was not different between groups with or without the BCG site reaction in both complete KD and incomplete KD.
Currently, BCG site reaction is regarded as skin rash in Korea. But in this study, the BCG site reaction was not associated with any principal clinical findings of diagnostic criteria including skin rash. These findings are compatible with the results of other recent studies in which the frequency of principal clinical findings was not different between groups with or without the BCG site reaction.78) We suggest BCG site reaction as a diagnostic finding independent to skin rash.
Uehara et al.2) suggested that the BCG site reaction is a useful diagnostic sign in KD among children aged 3 to 20 months in countries with a BCG vaccination program, because the proportion of patients with the reaction was higher than 70% and the cervical lymphadenopathy, which is one of the principal clinical findings, was less than 60% in patients aged ≤24 months. The similar result was also found in our study. In our opinion, the BCG site reaction independent to the principal clinical findings of KD may not regard as a part of skin rash, instead, suggests a possible role as an additional or alternative diagnostic parameter in young children undergoing BCG vaccination.
It is well-known that infants diagnosed with KD frequently show incomplete clinical presentation and longer duration of fever.1617) A coronary artery lesion associated with prolonged fever was relatively frequent in infants.18) The BCG site reaction appears early at 1–4 days after the onset of fever.219) Therefore, we believe that the BCG site reaction represents a useful finding for early diagnosis of KD, especially in young patients undergoing BCG vaccination.
This study has a few limitations. To determine whether the BCG site reaction is diagnostically consistent and compliant with the principal clinical findings, a higher number of patients and a negative control group — children with other febrile illness are needed.
In conclusion, the BCG inoculation site reaction was independent of the principal clinical findings of KD criteria and could be a useful tool for diagnosis of KD in children aged less than 18 months and undergoing BCG vaccination. Outcome of KD patients was not different between groups with or without the BCG site reaction in both complete KD and incomplete KD.
 XML Download
XML Download