

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Management of mental health symptoms such as low self-esteem, impulsivity, anxiety, and depressed mood in adolescents is crucial. Of the various mental health conditions, depression especially during the adolescent years, can continue into adulthood1; furthermore, it is closely connected to adolescent suicide,2 the third leading cause of premature death.3 According to one national study, the prevalence of depression in Korean students was 12.0%.4 The cumulative prevalence of depression before the age of 16 years was as high as 9.5%.5 Many risk factors affect depression, including relationships with friends, parental depressed mood, family economic status, smoking and inhalation uses, and exposure to trauma.6 In addition to students' social problems, body weight is also closely related to adolescents' depressed mood,7 with body weight dissatisfaction being an important risk factor for depression in students.8 Many studies that have evaluated body mass and depressed mood are focused on the body mass index (BMI) or perception of body image mainly in girls. Despite many studies, little is known about the influence of body composition on depressive mood. The underlying mechanism linking obesity and depression is not yet understood, and the physiologic link between muscle mass and mood disorders is uncertain.
Loss of skeletal muscle mass along with decreases in muscle strength or physical performance is called sarcopenia, a new geriatric syndrome. Multiple factors contribute to sarcopenia. Aging-related hormone changes such as reduced testosterone, estrogen, growth hormone, and corticosteroid levels might decrease muscle mass.9 Furthermore, increases in inflammatory cytokines, such as tumor necrosis factor (TNF)-α and interleukin (IL)-6, cause muscle breakdown.10 Along with aging-related changes, lifestyle patterns are also important in changing body composition. A less than optimal diet, especially low protein, and decreased physical function due to a sedentary lifestyle influence development of muscle loss and decreases in muscle function.11 Decreased muscle mass is well known to be related to decreased physical performance,12 impaired pulmonary function,13 increased metabolic diseases such as hypertension, type 2 diabetes, and hyperlipidemia, which are related to well-known risk factors for cardiovascular disease,14 a greater probability of falls and fractures,15 poorer quality of life, and high health care expenditures.16 Furthermore, it ultimately is associated with increased mortality.17 According to current literature, decreased skeletal muscle mass and common mental disorders share a pathophysiological pathway.18 In a cohort study involving hospitalized acutely ill older patients, individuals with low muscle mass (LMM) and decreased hand grip strength were more likely to suffer from depression.19 In a US study of middle-aged and older participants, management of sarcopenia via a home-based telemedicine exercise program was linked to a decrease in depressive symptoms.20 As in older adults, cardiorespiratory fitness has a protective effect against developing depression even after controlling for previous episodes of depression and weight in middle school students.21
Decreased muscle mass and impaired muscle functions are common in geriatric populations. Interestingly, in Korea, adolescents also have a high probability of a similar decline in muscle mass. Because of the social pressure to strive for the beauty ideal of a slimmer body, many adolescents impose severe dietary restrictions on themselves. Furthermore, Korean students also suffer from physical inactivity because of the intense college preparatory process. They spend most of the time seated, attending classes and studying. For these reasons, according to the abovementioned hypothesis, decreased skeletal muscle mass can be a contributing factor to depressive symptoms in adolescents like in adults. However, there have been no studies to explore the association of muscle mass and depressed mood in Korean students.
The aims of the present study were to evaluate the status of muscle mass and investigate the relationship between LMM status and mental health, especially depressive symptoms, among Korean adolescents and to potentially identify a new risk factor for depressed mood in adolescents.
METHODS
Study population
This study used data from the Korea National Health and Nutrition Examination Survey (KNHANES). The KNHANES has been performed periodically by Korea Centers for Disease Control and Prevention since 1998. The sample for the KNHANES was selected by stratifying household units followed by a multistage probability sampling process based on sex, age, and geographic area. Therefore, the KNHANES data is representative of the health of the entire Korean population. The KNHANES consists of a health interview, nutritional questionnaires, and physical examinations.
In KNHANES, dual-energy X-ray absorptiometry (DXA) was conducted from 2008 to 2011 in subjects over 10 years of age. In our study, we included adolescent boys and girls aged between 12 and 18 years who had undergone DXA and the health interview. Subjects were excluded if they had congenital heart disease, history of seizure, diabetes, or asthma. After exclusion, 1,233 adolescents participated in our study.
Definitions of LMM and obesity
DXA scans were conducted using a fan-beam densitometer (Hologic, Inc., Bedford, MA, USA) for measurement of whole body muscle mass and fat and bone mass. Appendicular muscle mass (ASM) was assessed by the sum of the muscle mass of upper and lower limbs, and ASM divided by weight (ASM/Wt, %) was used to analyze the absolute level of ASM.22 LMM was defined as the lower 10% of gender-specific ASM/Wt (%), like the prevalence among Korean adults.23 We think our study analyzed subjects with extremely LMM. Evaluation of the extremely reduced muscle mass group has more meaning because mild muscle mass reduction status can be easily changed with diet and exercise. Furthermore, adolescents mostly do not have comorbidities and health problems, so mild reduction of muscle was more easily compensated for than in the elderly. For the current large-scale, representative Korean study, obesity was defined as the waist circumference-to-height ratio (WHtR) being over 0.47 in both sexes.24
Mental health measures
This study used variables of self-reported questionnaires such as self-perceived stress, depressed mood, suicidal ideations, and suicide attempts to assess students' mental health. Participants who felt stressed or were experiencing uncontrollable stress were categorized as having self-perceived high stress. Depressed mood was determined by responses to the question: ‘During the past 12 months, have you ever felt sad or hopeless almost every day for 2 weeks in a row so that you stopped doing some usual activities?’ Suicide ideations were assessed by the question: ‘In the last 12 months, did you think about committing suicide?’ A positive response was considered to indicate suicidal ideation.
Statistical analysis
In order to be representative of the health status of Koreans, we used integrated weight values, which were determined by the number of participants in the research year and the research items. Continuous variables were calculated by a complex samples general linear model and presented using the mean ± standard error (SE). Categorical variables were analyzed by complex samples logistic regression analysis presented as the estimated proportion (SE). All analyses were performed by SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). P values less than 0.05 were considered statistically significant.
RESULTS
General characteristics of the participants
Our study included a total of 662 boys and 571 girls. According to the definition, the cut-off value of LMM was 28.43% and 21.94% in boys and girls, respectively. Among the boys and girls (81.3% and 62.6%, respectively) of the LMM group had a WHtR greater than 0.47. LMM groups were more obese than the normal group (P < 0.001). With regard to stress, 26.7% and 39.2% of boys and girls, respectively, in the LMM group reported they suffer from stress (P = 0.368, P = 0.105). There was no difference in depressive mood according to the muscle mass status in boys (P = 0.634). On the other hand, 9.5% of girls with normal muscle mass group and 20.7% of girls in the LMM group reported being depressed. Girls in the LMM group had a significantly higher rate of depressive mood compared with the normal muscle mass group (P = 0.023). General characteristics of subjects are shown in Table 1.
Table 1
General characteristics of participants
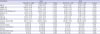
Values are expressed as mean ± standard error, estimated % (standard error). Calculated by complex sample general linear model and complex sample logistic regression analysis.
LMM = low muscle mass, WHtR = waist circumference-to-height ratio, ASM = appendicular skeletal muscle mass, Wt = weight.
![]()
Body composition and mental health
Mental health variables according to muscle mass and obesity status are summarized in Table 2. We classified the girls into four groups based on both muscle mass and obesity. There was no difference in depressive mood for all groups (P = 0.202). However, there was a significant difference in depressive mood between LMM and normal muscle mass groups, regardless of presence or absence of obesity (P = 0.017). Overall, 14.1% of girls in the LMM groups suffer from depressive mood, whereas only 9.7% of girls with normal muscle mass were depressed (P = 0.017). There was no difference in depressive mood between obese and non-obese groups, regardless of muscle mass status (P = 0.289). Furthermore, girls with LMM, regardless of obesity, thought they were obese (P < 0.001) and took more efforts to lose weight (P = 0.003).
Table 2
Comparison of mental health characteristics according to obesity and muscle mass status

Values are expressed as estimated % (standard error). Calculated by complex sample logistic regression analysis.
LMM = low muscle mass.
aP value of difference between LMM group and normal muscle mass group regardless of presence or absence of obesity; bP value of difference between obese group and non-obese group regardless of muscle mass status.
![]()
Effect of LMM on depressive mood in girls
To evaluate the independent association between LMM and depressive mood in girls, complex sample logistic regression analysis was performed. The results of analyses are shown in Table 3. After adjusting for age, the odds ratio (OR) for depressed mood was 2.37 (95% confidence interval [CI], 1.09–5.17; P = 0.030; model 1). Similarly, after further adjusting for WHtR with health habits, such as smoking status, alcohol consumption, and frequency of exercise, the LMM group was 2.79 times more at risk of depressed mood relative to the normal muscle mass group (95% CI, 1.11–7.02; P = 0.029; model 2). After further adjusting for self-reported obesity, weight loss efforts, and monthly household income, the trend increased (OR, 2.60; 95% CI, 1.05–6.49; P = 0.040; model 3). Furthermore, this trend was also observed in girls of LMM with obesity group. LMM with obese girls were 3.46 times more at risk of developing depression compared with girls with normal muscle mass after controlling age, WHtR, health habits, self-reported obesity, weight loss efforts, and monthly household income (95% CI, 1.00–11.97; P = 0.049; model 3).
Table 3
Adjusted OR for depressive mood in girls with LMM compared to normal muscle mass

Values are presented as prevalence OR (95% CI). Calculated by complex sample logistic regression analysis.
Model 1: adjust for age; Model 2: adjust for age, WHtR, smoking status, alcohol consumption, and frequency of physical activity; Model 3: adjust for age, WHtR, smoking status, alcohol consumption, frequency of physical activity, and self-reported obesity, weight-loss efforts, and monthly household income.
OR = odds ratio, LMM = low muscle mass, CI = confidence interval, WHtR = waist circumference-to-height ratio.
![]()
DISCUSSION
In our analysis, muscle mass was associated with depressed mood and LMM reveals independent associations with depressed mood in adolescent girls.
Our study results indicating that decreased skeletal muscle mass is correlated with depressive symptoms is consistent with previous studies with adults. In one study of healthy older men in a veterans' retirement community in Taiwan, participants with sarcopenia were highly associated with depressive symptoms, and sarcopenia was found to be an independent risk factor for depressive mood.25 In a cross-sectional Korean study, involving adults aged 60 or over, depressed men and women had 4.2% and 3.7% less appendicular skeletal muscle mass than mentally healthy ones, respectively.26 According to previous reports, in adolescents, perception of body image as well as BMI is important for depressed mood.27 Like the previous study, results from this study show that even after controlling for self-reported obesity status, LMM girls have a statistically significant higher probability of depressive symptoms compared to normal muscle mass girls.
Body composition is presumed to play an important role in the genesis of mental disorders like depression and anxiety, and the reverse might also be true. Physical inactivity can cause decreased muscle mass, but it is also a cause of depression. Eating disorders and disturbed eating patterns are related to both decreased muscle mass and onset of depression.28 Along with these lifestyle factors, similar biological pathways are known to affect a decline in muscle mass and brain function. Brain-derived neurotrophic factor (BDNF) drives neurogenesis in the hippocampus and is produced in skeletal muscle.29 Decreased contraction of skeletal muscle can cause a decline in secretion of BDNF as well as volume reduction of the hippocampus and thus, has been ultimately implicated in psychiatric illness.30 Furthermore, inflammation and oxidative stress are common pathophysiology of reduced muscle mass and depression.31 The activity of skeletal muscle boosts the immune system and its redox effects reduce muscle catabolism and maintain mood.32
Muscle mass can be modified by various interventions. Aerobic and anaerobic exercise is effective in the management of depression and maintaining proper muscle mass and strength.33 Exercise-based physical training programs are needed in schools. However, the most effective elements of exercise programs and the ideal frequency and intensity are still debated. Future research is needed to determine a proper exercise prescription. Moreover, for increasing muscle mass, adequate energy, especially protein intake, is essential. Education about diet pattern and portion sizes is required.
Our study has some limitations. First, in our study, for evaluating muscle mass, we used the weight-adjusted ASM, which was widely used in adults to define LMM. The definition of LMM varies,34 and there is no one prescribed way to measure it, especially in adolescents. A comparative study of various muscle mass indexes is needed. Second, when depression occurs, unlike adults, for adolescents many other variables such as parental marital status, depression of parents, problems in family communication, school status, and relationships with friends are affected.35 In our study, we could not evaluate the effect of some variables. Future studies are needed to overcome our study limitations. LMM is related to depressive symptoms, and LMM was found to be independently associated with depressed mood in adolescent girls.
 XML Download
XML Download