

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prenatal alcohol exposure of the developing fetus may lead to fetal alcohol spectrum disorders (FASD), associated with a wide range of adverse offspring outcomes representing the deleterious effects of ethanol.1234 Fetal alcohol syndrome (FAS), the most severe end of this continuum, is characterized phenotypically by growth retardation, microcephaly, and three specific facial dysmorphologies.124 Fatty acid ethyl esters (FAEEs), a non-oxidative ethanol metabolites, have been used as direct biomarkers of gestational ethanol consumption analyzed in the meconium of neonates, and even in very-low-birth-weight infants, with the detection time window of the second and third trimesters of pregnancy, largely in the last 3 months.5678910 The detection of FAEEs in meconium elucidates the patterns of ethanol exposure during the gestational period in contrast to women's hair, which cannot be guaranteed during pregnancy.5
Limited published data are available to support the relationship between meconium FAEEs and birth outcomes of fetal growth. There are two studies addressing the correlation of higher amounts of specific meconium FAEE analytes with greater birth weight, greater birth length, and greater gestational age at birth under low-to-moderate prenatal alcohol exposure, without adjusting for age and sex and analyzing for birth outcomes of prenatal growth restriction.1112 Furthermore, the degree to which cumulative FAEEs in meconium are related to fetal growth restriction in occipital frontal circumference (OFC), weight, and length that constitute several of the key cardinal features of FAS is unknown. Most studies investigating the effects of ethanol exposure on prenatal growth restriction assessed individual outcomes or largely focused on birth weight ≤ 10th centile (intrauterine growth restriction or small-for-gestational-age). However, based on the FAS diagnostic criteria,4 birth outcomes as a result of fetal growth restriction display combined manifestations of individual growth deficits. Accordingly, it is necessary to include the combined effects of growth deficits as well as the respective individual growth deficits in any correlation analysis. In Korea, risky alcohol consumption has been increasing among young females,1314 and the estimated prevalence of FAS was 4.2% among a sample of children receiving services in institutional settings.15 A population-based survey revealed that alcohol abuse among Korean women showed the highest prevalence between ages 20–34 years and increased among the recent generations.16 There has been an increasing interest among pediatricians, as the most likely practitioners to first encounter the neonates, for the early identification of infants with prenatal alcohol exposure who are potentially at risk for FASD, which can lead to reduced secondary disabilities, particularly in early infancy where facial dysmorphology assessment may be unavailable. We performed a prospective cohort study to examine the association between the accumulation of FAEEs in meconium and birth outcomes of growth deficits regarding OFC, weight, and length based on the FAS diagnostic growth criteria.
METHODS
Participants
This study was designed to include all infants born and receiving neonatal care in Uijeongbu St. Mary's Hospital, The Catholic University of Korea between 1st April and 31st August 2016. During the study period, 52 out of 209 infants born in the hospital were excluded: one with chromosomal disease, one with a congenital malformation, 19 due to multiple pregnancies, two with inaccurate gestational age, 11 who refused parental consent, and 18 with missed specimen collections. In total, meconium samples from 157 singleton infants were obtained and successfully analyzed. Information related to perinatal characteristics was acquired from the medical records, encompassing gestational age, infant sex, maternal age, parity, delivery method, prematurity, maternal hypertension, maternal diabetes, infant head circumference (HC), infant weight, and infant length. Each anthropometric measurement (HC, weight, and length at birth) was transformed into an age-sex-specific centile using Fenton growth charts.17 Birth outcomes of growth deficits were defined based on the key growth deficiency criteria for FAS as HC 10th percentile or less, weight 10th percentile or less, and length 10th percentile or less at birth. All possible combinations of each individual outcome were examined. Data pertaining to maternal drinking and smoking habits during pregnancy were acquired using standardized questionnaires and in-person interviews in the hospital during postpartum stay or within 1 month postpartum. All mothers were requested to provide details of the amount and frequency of their gestational alcohol consumption on an electronic form especially designed for the purpose of the study. In order to minimize the response bias and maximize the validity of self-reports,18 trained investigators recorded the information using electronic files, which were immediately stored in a password-protected system with restricted access. The number of weekly drinks was estimated based on the alcohol content of beverages (beer, wine, soju, or hard liquor) consumed. As previously described by the United States National Institute on Alcohol Abuse and Alcoholism,19 one standard drink contains 0.6 oz or 14 g of absolute ethanol. A FAEE concentration more than 2.00 nmol/g meconium has been recommended as positive for significant prenatal alcohol exposure.6720 For initial comparisons, all subjects were categorized into one of the three groups: undetectable FAEE (a group with meconium FAEE levels less than limit of quantitation (LOQ), under FAEE2 (a group with meconium FAEE levels greater than LOQ and 2.00 nmol/g or less), FAEE2 (a group with meconium FAEE levels greater than 2.00 nmol/g).
Meconium FAEE assessment
All meconium samples (> 500 mg per infant) were collected within 24 hours after birth, frozen and stored at −60°C for ≤ 6 months, and couriered to the Seoul Pharma Laboratories for the analysis of FAEEs. Quantification of FAEEs was performed by liquid chromatography/tandem mass spectrometry as described previously.21 Nine FAEEs including ethyl laurate (E12:0), ethyl myristate (E14:0), ethyl palmitate (E16:0), ethyl palmitoleate (E16:1), ethyl stearate (E18:0), ethyl oleate (E18:1), ethyl linoleate (E18:2), ethyl linolenate (E18:3), and ethyl arachidonate (E20:4) were quantified. The limits of detection varied from 0.01 to 0.08 nmol/g, whereas the LOQ ranged from 0.02 to 0.27 nmol/g. Intra- and inter-assay precisions varied from 7% to 21% and from 10% to 17%, respectively. The intra-assay and inter-assay accuracies ranged from −17% to 15% and from −4% to 14%, respectively. The individual concentrations of the nine FAEEs were summed to obtain the cumulative concentration.
Statistical analysis
The FAEE concentration groups were compared using Fisher's exact test for categorical variables and Kruskal-Wallis test for continuous variables. Spearman rank order correlation was used to assess the association of cumulative FAEE concentrations with alcohol exposure (drinks per week) during all the trimesters and during second-to-third trimesters, and anthropometric parameters at birth. Logistic regression modelling was performed for individual and combined variables of growth deficits, and the odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. All baseline characteristics were included as possible confounders in the models. Receiver operating characteristic (ROC) curve and area under the ROC curve (AUC) were used to determine the accuracy of the model in categorizing the significant outcomes in multivariate logistic regression. Fisher's exact test and conditional logistic regression were conducted to determine adequate cut-offs. Statistical analyses were performed using SPSS version 17.0 (SPSS, Chicago, IL, USA). A two-tailed P ≤ 0.05 was considered statistically significant.
RESULTS
Baseline characteristics and birth outcomes of growth deficits
Of the 157 meconium samples analyzed successfully, four (2.5%) tested positive for cumulative FAEE concentrations exceeding 2 nmol/g, 67 were detected at total FAEE concentrations ≤ 2 nmol/g, and 86 were undetected for quantifiable amounts of FAEEs (Table 1). The prevalence of gestational ethanol use was 8.9% (14/157 female) during all trimesters, and 2.5% (4/157 female) during second-to-third trimesters. Among the four mothers with infants testing positive for FAEEs, two reported ethanol use during the second-to-third trimesters (Table 1). Maternal ethanol ingestion during all the trimesters, HC and weight, both, 10th percentile or less, and HC and weight and length, all of them, 10th percentile or less were significantly associated with the cumulative FAEE concentrations (Table 1).
Table 1
Baseline characteristics and birth outcomes of growth deficits in 157 infants based on meconium FAEE concentrations

Values are presented as median (range) or number (%).
FAEE = fatty acid ethyl ester, SE = standard error, CI = confidence interval, LOQ = limit of quantitation, HC = head circumference; Undetectable FAEE = a group with meconium FAEE levels less than LOQ, Under FAEE2 = a group with meconium FAEE levels greater than LOQ and 2.00 nmol/g or less, FAEE2 = a group with meconium FAEE levels greater than 2.00 nmol/g, HC ≤ 10P = head circumference 10th percentile or less, Weight ≤ 10P = weight 10th percentile or less, Length ≤ 10P = length 10th percentile or less.
aKruskal-Wallis test; bFisher's exact test.
Relationships of meconium FAEEs with prenatal alcohol exposure, birth growth and birth outcomes of growth deficits
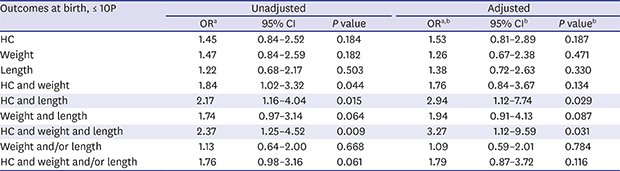
Correlation analyses revealed significant associations between cumulative meconium FAEE levels and drinks per week during all the trimesters (ρ = 0.160 and P = 0.046) and during second-to-third trimesters (ρ = 0.174 and P = 0.029). However, no correlation with birth growth parameters in the age-sex-specific centile (HC, ρ = −0.128 and P = 0.111; weight, ρ = −0.018 and P = 0.825; length, ρ = 0.068 and P = 0.398) was found. In logistic regression, for each 1 nmol/g higher FAEE concentration, the odds for HC and weight, both, 10th percentile or less increased by 1.84-fold (P = 0.044), the odds for HC and length, both, 10th percentile or less increased by 2.17-fold (P = 0.015), and the odds for HC and weight and length, all of them, 10th percentile or less increased by 2.37-fold (P = 0.009) (Table 2). After adjusting for potential confounders (gestational age, infant sex, maternal age, parity, caesarean section delivery, prematurity, maternal hypertension, maternal diabetes, and smoking during pregnancy), the odds of HC and length, both, 10th percentile or less increased by 2.94-fold (P = 0.029), and the odds of HC and weight and length, all of them, 10th percentile or less increased by 3.27-fold (P = 0.031) (Table 2).
Table 2
Association of cumulative meconium FAEE concentrations with birth outcomes of growth deficits
FAEE = fatty acid ethyl ester, OR = odds ratio, CI = confidence interval, HC = head circumference.
HC ≤ 10P = head circumference 10th percentile or less, Weight ≤ 10P = weight 10th percentile or less, Length ≤ 10P = length 10th percentile or less.
aORs are estimated per 1 nmol/g higher FAEE concentration; bValues are adjusted for gestational age, infant sex, maternal age, parity, caesarean section delivery, prematurity, maternal hypertension, maternal diabetes, and smoking during pregnancy.
Meconium FAEEs: analysis at different cut-off levels
ROC curve evaluating cumulative FAEE concentrations to identify newborns with HC and length, both, 10th percentile or less generated an AUC of 0.68 (95% CI, 0.44–0.93; P = 0.162). The sensitivity and specificity were 40.0% and 92.8%, respectively, at a cut-off of 0.5 nmol/g, and 20.0% and 98.0%, respectively, at a cut-off of 2 nmol/g. In the ROC analysis of cumulative FAEE concentrations distinguishing newborns with and without HC and weight and length, all of them, 10th percentile or less, the AUC was 0.79 (95% CI, 0.61–0.97; P = 0.05). The sensitivity and specificity were 50.0% and 92.8%, respectively, at a cut-off of 0.5 nmol/g and 25.0% and 98.0%, respectively, at a cut-off value 2 nmol/g. In conditional logistic regression, significant ORs were found at cut-offs of 0.5 and 2.0 nmol/g for HC and length, both, 10th percentile or less (Table 3) and at cut-offs of 0.3, 0.4, 0.5 and 2.0 nmol/g for HC and weight and length, all of them, 10th percentile or less (Table 4). Fisher's exact test revealed the only significant cut-off of 0.5 nmol/g for HC and weight and length, all of them, 10th percentile or less (P = 0.035) (Table 4).
Table 3
Meconium FAEE concentrations at different cut-offs and HC and length, both, 10th percentile or less (HC and length ≤ 10P) at birth

Table 4
Meconium FAEE concentrations at cut-offs and HC and weight and length, all of them, 10th percentile or less (HC and weight and length ≤ 10P) at birth

DISCUSSION
The current study demonstrated that higher cumulative concentrations of nine FAEEs in meconium were associated with birth outcomes of combined growth deficits, including HC and length, both, 10th percentile or less and HC and weight and length, all of them, 10th percentile or less (Table 2), despite lack of associations with individual birth outcomes of growth deficits and growth parameters (age-sex-specific HC, weight and length centiles) in multivariate logistic modelling. The association was even more robust with the combination of all three individual outcomes representing symmetric intrauterine growth restriction in unadjusted and adjusted models. These findings suggest that the combined growth deficits at birth were significantly correlated with ethanol exposure relative to the respective outcomes. The common denominator of HC and length, both, 10th percentile or less of the significant variables suggests that OFC and length reflecting fetal brain and bone growth were more significant than weight largely contributed to by other soft tissues in fetal growth restriction related to ethanol exposure, indicating the existence of a plausible alcohol-related pattern of intrauterine growth restriction. To date, numerous studies involving animal models have documented detrimental effects of alcohol on fetal brain and bone development. A variety of mechanisms investigated in experimental models revealed significant deficits in neural development following embryonic ethanol exposure, including rapid cerebral vasoconstriction,22 abnormal neural maturation,23 neurodegeneration by reactive oxygen species24 and neuroapoptosis25 in the developing brain. A chick embryo model demonstrated that ethanol exposure represses development of craniofacial and long bones by inhibiting the generation of cranial neural crest cells, chondrogenesis and ossification via excessive production of reactive oxygen species and altered osteogenesis-related gene expression.26 A mouse micro-computed tomography study documented growth retardation of fetal craniofacial bone following alcohol exposure, with the neurocranium (upper skull) more significantly affected than the viscerocranium (face).27 Studies involving sheep and rat fetuses revealed that fetal bone growth was more sensitive to alcohol than overall growth as measured by body weight, particularly at moderate exposure levels.2829 Taken together with our results, it is postulated that OFC and length are more significant predictors of developmental ethanol exposure than weight that has been focused on in previous studies.
The prenatal ethanol exposure levels of our infants studied considered low-to-moderate depending on the maternal self-reports. Maternal alcohol intake, especially at relatively higher levels during pregnancy, results in fetal growth restriction in weight, OFC and length.303132 However, inconsistent results have been observed in infants prenatally exposed to light-to-moderate maternal drinking, including lack of effect on fetal growth restriction and greater birth weight.333435
The prevalence of positive FAEE analyses for significant prenatal alcohol exposure in our cohort was 2.5%. This is lower than the 3.1%–4.4% (39–56 of 1,271 samples) reported in the Prince Edward Island population-based study36 with the greater observed maximum FAEE level than ours, and higher than the 2% (11 of 505 specimens) in a cohort of Southwestern Ugandan women with the maximum FAEE level similar to ours.37 The relatively low prevalence in our cohort may result from sample collection in a low-risk community hospital setting, as opposed to high-risk settings such as special institutional clinics offering structured services. The high opt-out rate of 25% and the short study period of 5 months in our study may have biased the sample towards the lower prevalence of positive FAEE analyses as well as the lower maximum FAEE concentration. This result may be attributed to the differential decline in participation rate by high-risk women, and the possible effect of seasonal variation in drinking habits.
Meconium FAEEs have been accepted as established biomarkers of prenatal alcohol exposure in the updated clinical guideline for the diagnosis of FASD.4 The clinical use of meconium FAEE analysis has been attempted to identify children at risk for future alcohol-related problems,1138 and was advocated by a meta-analysis complementing maternal self-reports increasing the risk of under-reporting of gestational ethanol intake.39 It is likely that more robust data correlate prenatal alcohol exposure with the cumulative sum of FAEEs rather than individual FAEEs in meconium.7 Our study showed a positive correlation between cumulative FAEE concentrations in meconium and maternal self-reported drinking, as reported previously.6740 The cut-offs for positive FAEE analyses in meconium indicating significant prenatal alcohol exposure vary widely from 0.17 to 33 nmol/g.672040 Our study found that a cut-off of > 0.5 nmol/g in meconium was significant for HC and weight and length, all of them, 10th percentile or less at birth in both Fisher's exact test and logistic regression analysis (Table 4). However, this finding was limited by the results from ROC analyses showing the low sensitivity of 50.0% at the 0.5 nmol/g cut-off despite an AUC of 0.79 (P = 0.05) with a cut-off specificity of 92.8%.
The study has limitations. The small size of the sample collected in one setting limits generalization of the results and warrants further investigations. Another limitation is the detection window of meconium restricted to the latter half of gestation. However, a cohort study of premature newborns proposed ethyl linolenate, a meconium FAEE analyte, as a potential biomarker for the detection of trimester one ethanol exposure.10
In conclusion, this study suggests that elevated cumulative FAEEs in meconium are associated with combined growth deficits at birth, specifically HC and length, both, 10th percentile or less, which might be related to detrimental effects of alcohol on fetal brain and bone growth, suggesting a plausible alcohol-specific pattern of intrauterine growth restriction. It additionally suggests that elevated meconium FAEEs may be an informative biomarker for the early detection of infants potentially at risk for FASD. Our results reinforce other studies recommending the complementary use of meconium FAEE assay in a multi-step approach involving maternal self-reporting and screening with a panel of other biomarkers in neonatal and maternal matrices.5610
 XML Download
XML Download