

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hip fractures are the most severe fracture type in elderly patients with osteoporosis1). Ninety percent of patients with hip fracture are over the age of sixty-five years, and most have major comorbidities that contribute to high rates of morbidity and mortality associated with their hip fractures2). It has been estimated that 250,000 hip fractures occur in the United States every year, with half of them being intertrochanteric3). Primary orthopaedic goals in patients with an intertrochanteric hip fracture are to successfully return to safe mobility-which relies on stability and strength of fracture fixation4).
Over the past fifty years, a wide variety of implants and fixation strategies have been utilized for surgical stabilization of intertrochanteric hip fractures. Antegrade intramedullary nailing of intertrochanteric fractures was introduced by Halder5) in the 1980s in the form of Gamma nail. Since then, a variety of hip fracture fixation devices have been developed for the treatment of intertrochanteric fractures. Additionally, use of a compression hip screw (CHS) is the gold standard treatment for intertrochanteric fractures of the femur67).
For the position of intertrochanteric fracture, traction tables are presently used universally as a standard tool for CHS fixation to achieve and maintain satisfactory reduction before instrumentation is performed. However, a significant amount of time is needed for preoperative set up when a traction table is used. Although there have not been many reports on traction table-associated complications during CHS fixation (e.g., pudendal, sciatic, or femoral nerve injury) due to traction or direct pressure; these complications are also common in patients undergoing femoral nailing because of the large amount of traction force involved8910). Furthermore, a traction table may not be available in hospitals with limited resources. Hence, a manual traction technique performed in the supine position using only a radiolucent table has been developed to avoid the need for a traction table. CHS fixation at our institution has been performed since 1979 using traction tables. CHS fixation with patient in lateral decubitus position without using traction table began in 2000 at our institution because of several notable advantages (e.g., easy to prepare for draping, easy to check anteroposterior (AP) and lateral radiograph, and easy to perform surgery, especially when fixing with an additional screw).
The purpose of this study was to introduce a surgical technique of CHS fixation in the decubitus position and report results of 100 consecutive cases.
Go to : 
MATERIALS AND METHODS
This retrospective study was approved by the Institutional Review Board (IRB) of Chonnam National University Hospital (CNUHH-2018-046).
1. Demographic Data
A retrospective study was designed to assess the use of a CHS (Stryker, Basel, Switzerland) with lateral approach to treat intertrochanteric fractures in elderly patients. A total of 100 patients underwent surgery using CHS with patients in the lateral decubitus position between March 2008 and May 2011. All procedures were performed by a single surgeon. Inclusion criteria were 1) patients older than 45 years of age with a femoral intertrochanteric fracture who had undergone surgery using CHS in the lateral decubitus position and 2) patients for whom ≥3 months follow-up was available. Subjects with open fractures, multiple fractures, pathologic fractures except osteoporotic fractures, previous ipsilateral hip or femur surgery, or developmental abnormality were excluded. A total of 20 patients were excluded for the following reasons; 1) failed to continue with follow-up due to expire (n=14) and 2) failed to continue with follow-up due to poor general condition (n=6). All associated injuries were managed appropriately as needed. Fractures were classified as either stable (31-A1) or unstable (31-A2 and 31-A3) on the basis of Evans11) and the AO Foundation and Orthopaedic Trauma Association (AO/OTA) classification12).
2. Surgical Technique
All patients were treated with first-generation cephalosporin (cefazolin) as a prophylactic antibiotic which was administered one hour before surgery and continued for three days postoperatively. The anesthetic method was selected by the treating anesthesiologist. Patients were operated in lateral and limbs were prepped and draped using contemporary techniques. An incision of approximately 15 cm was made over the lateral aspect of the greater trochanter extending distally 12 cm and proximally 3 cm on vastus ridge. Superficial fascia was incised along with the skin incision. Electrocautery was used to minimize blood loss. Fascia lata was cut longitudinally for the length of the incision and vastus lateralis was incised in a reverse “L” shape starting from the anterior edge of the vastus ridge while retaining a 5-mm attachment on the vastus ridge. One perforating artery was ligated and located 7 to 8 cm distal from the vastus ridge. Under the guidance of a C-arm, gentle traction of the fractured femur was performed. If the fracture was unstable and it was not reduced, the reverse “L” shape incision was extended anteriorly to the fracture site. A bone hook was applied at the fracture site and distal fragment traction was performed. Next, a straight Homann retractor was applied as a lever arm into the fracture site to ensure that the proximal fragment was placed more anteriorly to the distal fragment. Under C-arm guidance, two Steinmann pins were inserted to the proximal part of the lag screw insertion site to maintain a reduced state of fracture during the procedure (Fig. 1). A lag screw guide pin was inserted using a lag screw guide. If the lag screw was in the correct position in AP view (Fig. 2), the lateral view image was checked with 90°hip flexion and 45°abduction. After reaming and tapping, a lag screw was inserted. A 135°-side plate with at least four holes available below the fracture was used. After fixation of the side plate, a lag screw was inserted and the wound was closed over suction drain. The postoperative rehabilitation protocol included quadriceps strengthening. Hip and knee range-of-motion exercises commenced immediately after surgery. Patients were encouraged to mobilize out of bed on the second postoperative day. Partial weight bearing with a walker to the limit of pain was encouraged for all patients and continued for at least eight weeks. Subsequently, patients could be advanced to full weight bearing based on the appearance of recanalization or bridging callus on follow-up radiographs.


Postoperative evaluations were performed at one month, three months, six months, one year, and yearly thereafter. A total of 20 patients were excluded for the following reasons: 1) failed to continue with at least three month follow-up (14 patients), 2) passed away within three month follow-up (6 patients).
3. Clinical Assessment
Clinical results were evaluated based on postoperative chart records and a final follow-up evaluation. Patient clinical functions were analyzed by comparing preoperative and last follow-up Koval score13) and complications. This study also presents a summary of other assessments, including operation time, changes in postoperative hemoglobin levels, and the volume of transfusion.
4. Radiographic Assessment
All radiographic measurements (e.g., bone union time, nonunion, sliding, angulation of lag screw, and screw tip migration) were evaluated using AP and lateral radiographs with PACS (Picture Archiving and Communication Systems). Bone union was judged as callus appearance across the fracture line on AP and lateral radiographs. Radiologic failure was defined as i) screw sliding at more than 15 mm, ii) varus collapse of the proximal fragment, iii) lag screw cut-out from the femoral head, iv) varus angulation at more than 5°, or v) screw-tip migration greater than 7 mm14).
5. Statistical Analysis
Statistical analysis was performed using PASW Statistics software package (ver. 18.0; IBM Corp., Armonk, NY, USA). Univariate analysis was performed to evaluate possible influencing variables of Harris hip score (HHS) and Koval score at 1-year follow-up using the paired sample t-test. Differences were considered statistically significant at P-values ≤0.05.
Go to :
RESULTS
Of the included patients, 66 were women and 34 were men (mean age, 77.5 years; range, 45–93 years). Mean bone mineral density values for the spine and femur were −3.0 (range, −6.4–0.6) and −2.7 (range, −5.5–0.4), respectively. Thirty-nine fractures involved the right side and 61 fractures involved the left side. The mean preoperative Koval score was 1.4 (range, 0–5). A total of 70 patients required fixation with an additional screw (n=25), wire (n=12), or screw and wire (n=33). The remaining thirty cases needed no additional fixation. Based on the Evans classification, there were 23 cases of stable fractures and 77 cases of instable fractures. By AO/OTA classification, there were 7 cases of A1.1, 4 cases of A1.2, 1 case of A1.3, 11 cases of A2.1, 40 cases of A2.2, and 37 cases of A2.3 (Table 1).
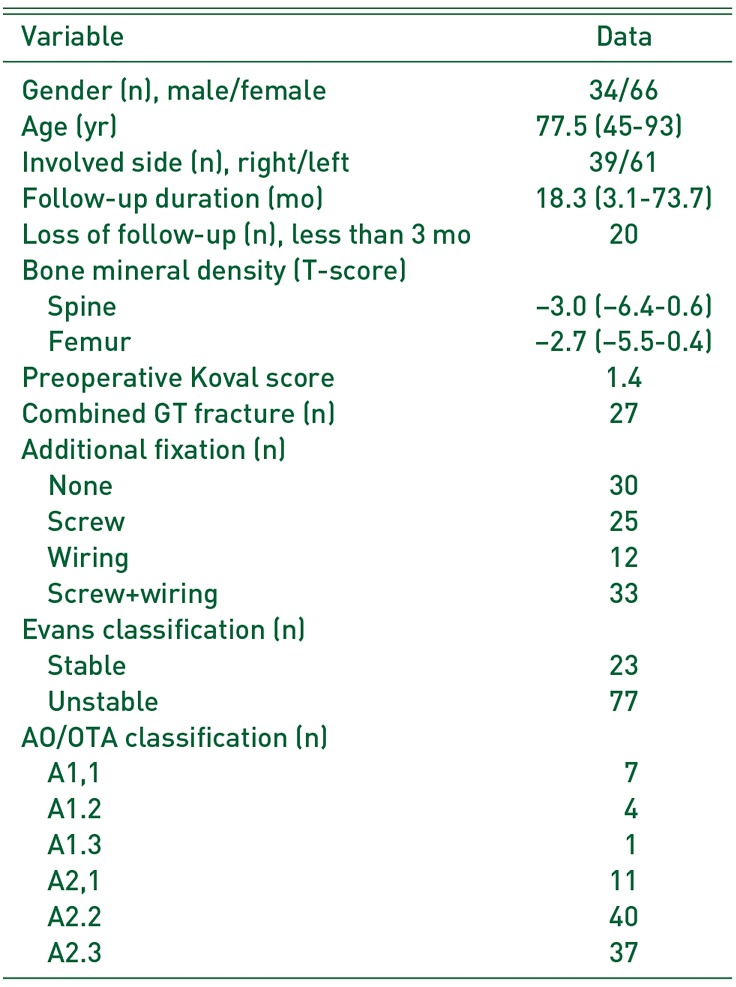
Table 1
Patients Demographics
![]()
Mean HHS and Koval scores at the last follow-up (mean 18.3 months after the operation) were 85 months (range, 72–90 months) and 2.6 months (range, 0–5 months; P<0.05) respectively. The mean operation time in the year of 2008, 2009, 2010, or 2011was 94.5, 70.0, 67.6, or 61.7 minutes, respectively. Mean hemoglobin levels were 11.4 g/dL preoperatively and 9.9 g/dL postoperatively.
All patients achieved acceptable reduction of the fracture and desired position of the lag screw. Mean bone union time was 5.0 months (range, 2.0–8.2 months). Radiographic results are as follows: i) AP average tip-apex distance (TAD) (6.95 mm; range, 1.27–14.63 mm), ii) lateral average TAD (7.26 mm; range, 1.20–18.43 mm), and iii) total average TAD (14.21 mm; range, 2.47–28.66 mm). Average angulation was varus 0.72°(range, −7.6°−12.7°). There were no cases of screw tip migration, lag screw cut-out, or nonunion; however, there were four cases of excessive screw sliding and six cases of varus angulation at more than 5°(Table 2). The number of radiologic failures decreased from 5 in 2008 to 1 in 2011 (Fig. 3).
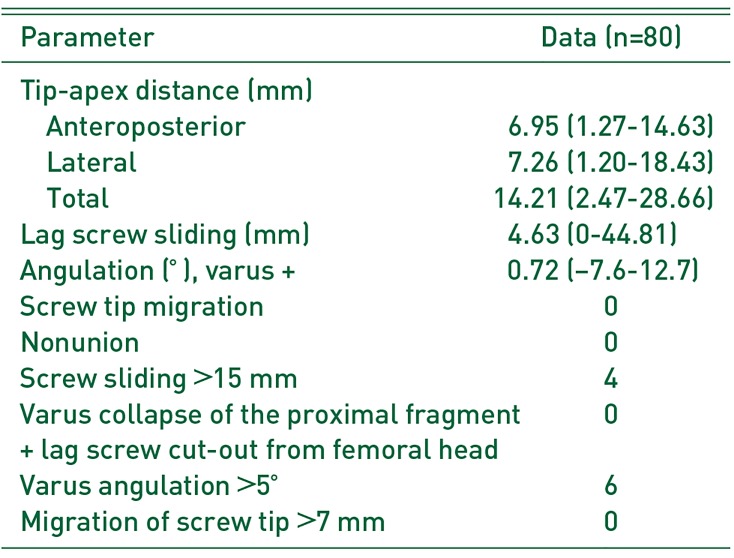
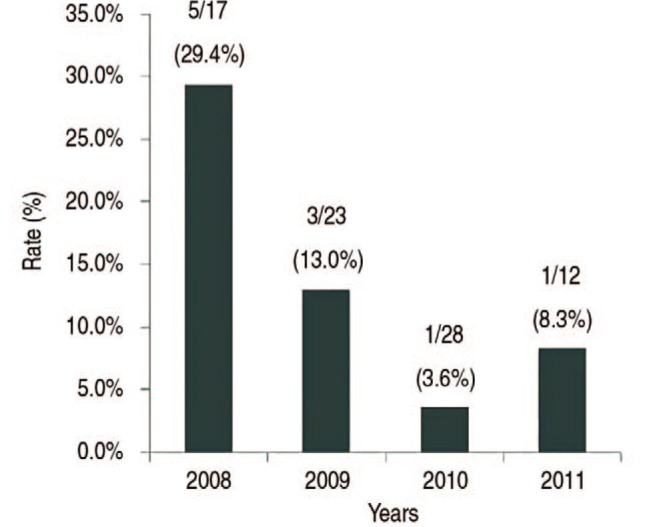
Table 2
Radiographic Results
![]()
Complications are presented in Table 3 and include delirium (n=16), pneumonia (n=2), pleural effusion (n=2), renal dysfunction (n=2) and one case each of superficial infection and revision surgery to total hip arthroplasty.
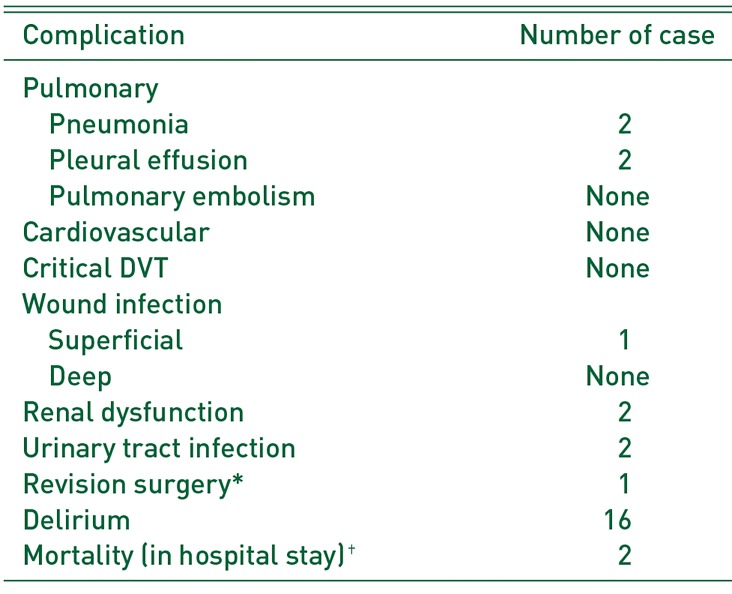
Table 3
Complications
![]()
Go to :
DISCUSSION
Intertrochanteric fractures frequently affect elderly osteoporotic patients, leading to significant morbidity and mortality. With advancing age of the general population, complications during bone healing due to inadequate fixation result in significant consumption of health care system resources15). The major advantage of CHS is that sliding of the lag screw allows impaction of fracture fragments, thereby promoting bone healing. However, its application has limitations1617). In elderly patients with osteoporotic bone, varus collapse of the proximal fragment and even cut-out of the lag screw may occur due to inadequate screw anchoring in the femoral head. In unstable fractures, excessive sliding of the lag screw caused by insufficient abutment at the fracture may shorten the femur and result in various morbidities.
In a prospective randomized study18) the outcomes of CHS (Osteo Hip Screw; Osteo, Selzach, Switzerland) compared with intramedullary hip screw (IMHS, Smith and Nephew Richards, Memphis, TN, USA.), were similar. The author did not recommend “routine” use of intramedullary hip screws for treatment of intertrochanteric fractures. Baumgaertner et al.19) have performed a prospective randomized study involving 135 patients treated either with a CHS or intramedullary hip screw and observed no differences in rates of functional recovery between the two fixation groups.
There are advantages to treating patients in the lateral position compared with use of a fracture table (e.g., reduced set up time, surgical time, and fluoroscopic exposure time)20). Also, for patients whom fracture table is unavailable, including obese, short stature, or amputated, lateral decubitus position is recommended21).
Data for TAD and cut-out complication were reported in five studies involving femoral intertrochanteric fractures treated with CHS in supine position with a traction table (Table 4). They were compared with this study2223242526) and the results were superior for patients with femoral intertrochanteric fractures treated in the lateral decubitus position. Adequate TAD means accurate screw position associated with less cut-out failure25). As it is easy to check accurate screw position in the lateral decubitus position, this study achieved favorable results in TAD and the rate of cut-out failure. However, our study used additional fixation. Further evaluation is needed to evaluate the relationship between additional fixation and cut-out failure.
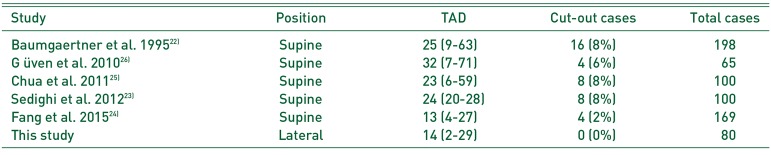
Table 4
Comparison of TAD and Screw Cut-out Complication between Lateral Position and Supine Position
| Study | Position | TAD | Cut-out cases | Total cases |
|---|---|---|---|---|
| Baumgaertner et al. 199522) | Supine | 25 (9–63) | 16 (8%) | 198 |
| G üven et al. 201026) | Supine | 32 (7–71) | 4 (6%) | 65 |
| Chua et al. 201125) | Supine | 23 (6–59) | 8 (8%) | 100 |
| Sedighi et al. 201223) | Supine | 24 (20–28) | 8 (8%) | 100 |
| Fang et al. 201524) | Supine | 13 (4–27) | 4 (2%) | 169 |
| This study | Lateral | 14 (2–29) | 0 (0%) | 80 |
![]()
Limitations of this study included its small sample size, short term follow-up, and its retrospective nature. Another limitation concerns preexisting conditions and postoperative living arrangements that made it difficult for patients to keep follow-up appointments for the twelve-month period of the study, leading to required use of telephone interviews to complete SF-36 and functional recovery score questionnaires.
Go to :
CONCLUSION
CHS fixation with patients in the lateral decubitus position provided relatively good results in TAD and cut-out ratio. This approach also significantly reduced preoperative preparation time without sacrificing reduction alignment. This technique is advisable for regular CHS fixation of intertrochanteric fractures, particularly when a traction table is unavailable or when frequent operative bed transfer should be avoided (e.g., polytrauma patients for whom multiple procedures are necessary).
Go to :
 XML Download
XML Download