

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hip fractures in elderly patients are becoming a major social problem from various perspectives, including the progressive aging of global societies1). The elderly have a high risk of hip fracture, even with minor injuries because of osteoporosis, while early surgical treatment may be difficult due to comorbidities and medication2). Moreover, even after surgical treatment, secure fixation is hard to achieve due to osteoporosis. Additionally, impaired mobility following surgery may increase complications (e.g., pneumonia, sores, mortality). These conditions not only prolong the treatment period and result in higher medical expenditures, but also create a higher overall socioeconomic cost3). Therefore, many studies on the treatment of hip fractures in elderly patients have examined methods for increasing successful treatment outcomes and enabling early ambulation without increasing patient mortality45).
Intertrochanteric fractures-one of the most common types of fracture in elderly patients-account for roughly 45% to 50% of all hip fractures, and of these, 35% to 60% are unstable and accompanied by comminution of the posteromedial buttress, exceeding a simple lesser trochanteric fragment or those with subtrochanteric extension6789). Failure rates of unstable intertrochanteric fracture treatment have been decreasing, in part because of the development of various types of proximal nail and surgical techniques that can achieve accurate reduction. However, osteoporosis and cognitive dysfunction of patients still remain major causes of fixation failure as they may make it difficult to achieve strong fixation in the fracture site and interfere with early ambulation4,5). Consequently, although still debatable, arthroplasty may be considered a preferred approach for treating unstable intertrochanteric fractures10).
Positive outcomes have been reported from those studies using arthroplasty to treat hip fractures in elderly patients. However, in cases of unstable intertrochanteric fractures, it is difficult to achieve stable fixation and identify the anatomic structure because of comminution and displacement of the bones near the stem; this injury is also associated with risks of complications (e.g., greater trochanteric nonunion, heterotopic ossification [HO]). Additionally, cement-related fatal cardiovascular complications are also present111213). Therefore, the decisions on which surgical approach and prosthesis to use become very important, particularly which type of stem, just as is the case with femoral neck14).
Accordingly, this study aimed to compare cemented and cementless bipolar hemiarthroplasty in elderly patients with unstable intertrochanteric fractures by using a meta-analysis and systematic review of studies on these two methods.
Go to : 
MATERIALS AND METHODS
A systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines15).
1. Study Eligibility Criteria
Studies were selected based on the following inclusion criteria: 1) studies of unstable intertrochanteric fracture was reported; 2) cemented or cementless hemiarthroplasty was used for fracture treatment; and 3) studies reporting treatment outcomes. Studies were excluded if they failed to meet the above criteria, were case reports, or involved pathologic fractures.
2. Search Methods for Identification of Studies
PubMed Central, OVID Medline, Cochrane Collaboration Library, Web of Science, EMBASE, and AHRQ databases were searched to identify relevant studies published up until September 2017 with English language restriction. The following search terms were used: “unstable intertrochanteric fracture arthroplasty”, “unstable trochanteric fracture arthroplasty”, “unstable trochanteric fracture bipolar”. A manual search was also conducted to identify other potential references of relevance. Two investigators independently reviewed titles, abstracts, and full text of all potentially relevant studies as recommended by the Cochrane Collaboration.
3. Data Extraction
The following information was extracted from the included articles: authors, publication date, study design, patient number, gender, fracture classification, prosthesis type, operation time, blood loss, hospital stay period, outcome, complication, and mortality.
4. Methodological Quality Assessment
The Newcastle-Ottawa scale was used to assess methodological quality of non-randomized studies. It contains 8 items, which are categorized into 3 dimensions: the selection of the study population, the comparability of the groups, and the ascertainment of the exposure (case-control study) or outcome (cohort study). Each dimension consists of subcategorized questions: selection (a maximum of 4 stars), comparability (a maximum of 2 stars), and exposure or outcome (a maximum of 3 stars). Thus, a study can be awarded a maximum of 9 stars, indicating the highest quality. Two of the authors independently evaluated the quality of all the studies.
5. Data Analysis
The primary outcome was leg length discrepancy (LLD). Secondary outcomes were treatment outcomes (i.e., aseptic loosening, dislocation, nonunion of greater trochanter) and complications (i.e., infection, HO, periprosthetic fracture, mortality).
This meta-analysis was performed with Comprehensive Meta-Analysis statistical software (version 2.0; Biostat, Englewood, NJ, USA) and the level of significance was set at P<0.05. For dichotomous outcomes, odds ratio and 95% confidence interval (CI) were calculated. For continuous outcomes, standardized mean difference and 95% CI were calculated. The size of heterogeneity across studies was estimated with I2 statistic and the chi-squared test. A P-value of >0.10 and an I2 ≤50% were considered of no statistical heterogeneity16). To test heterogeneity, Higgins I2 statistics were used. SignifIcant heterogeneity was observed in these studies; therefore, we reported the data from a random-effects perspective. A random-effect or fixed-effect model was adopted depending on the heterogeneity of the included studies. Sensitivity analysis was conducted by omitting one study in each turn and pooling the data of the remaining studies to explore possible explanations for high heterogeneity and determine the stability of the outcomes.
Go to :
RESULTS
1. Search Results
The initial search identified 357 references from the selected databases. However, 315 were excluded after screening the abstracts and titles. The remaining 42 studies underwent full-text review; four studies were further excluded after a full review. Details on the identification of relevant studies are shown in the flow chart of the study selection process (Fig. 1). Study design, number of subjects, demographic factors, surgical approach, type of prosthesis and clinical results included in this study are summarized in Tables 1 and 2.
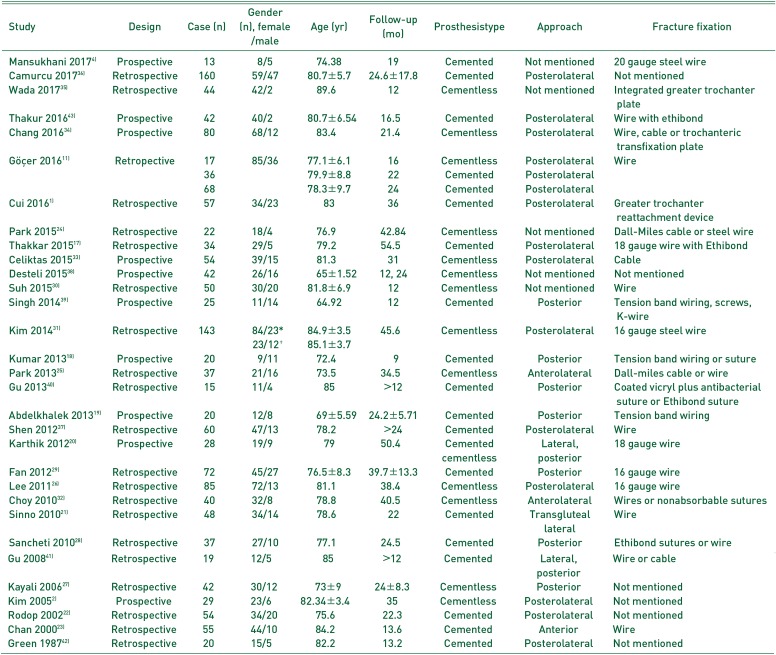
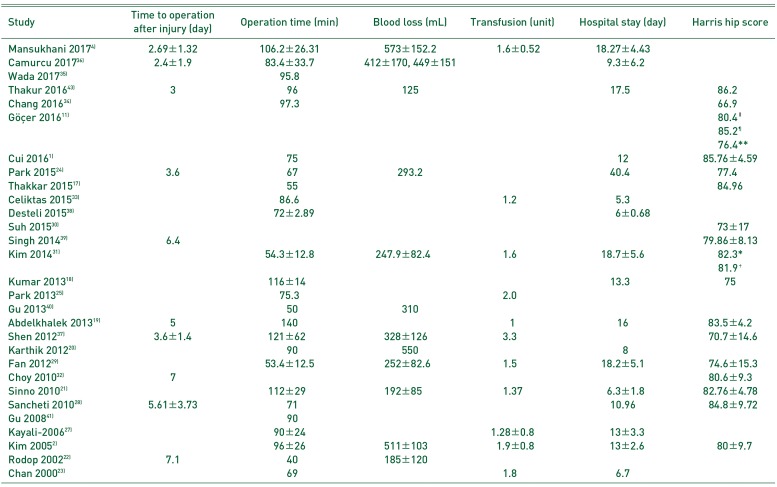
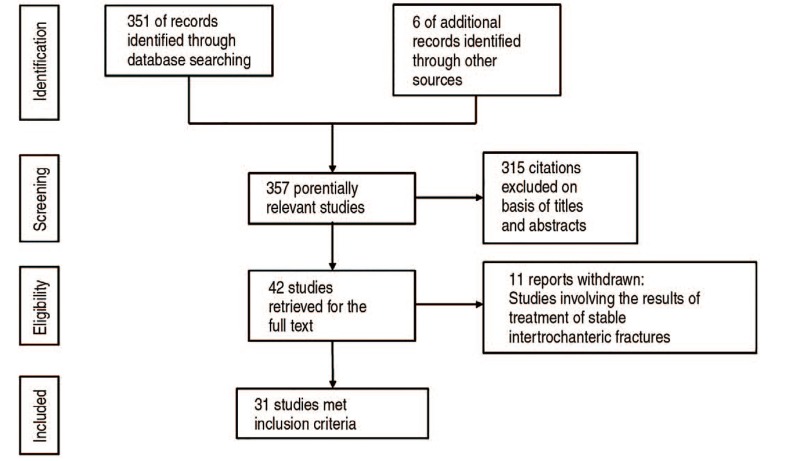
Table 1
Demographics in Included Studies
| Study | Design | Case (n) | Gender (n), female/male | Age (yr) | Follow-up (mo) | Prosthesistype | Approach | Fracture fixation |
|---|---|---|---|---|---|---|---|---|
| Mansukhani 20174) | Prospective | 13 | 8/5 | 74.38 | 19 | Cemented | Not mentioned | 20 gauge steel wire |
| Camurcu 201736) | Retrospective | 160 | 59/47 | 80.7±5.7 | 24.6±17.8 | Cemented | Posterolateral | Not mentioned |
| Wada 201735) | Retrospective | 44 | 42/2 | 89.6 | 12 | Cementless | Not mentioned | Integrated greater trochanter plate |
| Thakur 201643) | Prospective | 42 | 40/2 | 80.7±6.54 | 16.5 | Cemented | Posterolateral | Wire with ethibond |
| Chang 201634) | Prospective | 80 | 68/12 | 83.4 | 21.4 | Cementless | Posterolateral | Wire, cable or trochanteric transfixation plate |
| Göçer 201611) | Retropective | 17 | 85/36 | 77.1±6.1 | 16 | Cementless | Posterolateral | Wire |
| 36 | 79.9±8.8 | 22 | Cemented | Posterolateral | ||||
| 68 | 78.3±9.7 | 24 | Cemented | Posterolateral | ||||
| Cui 20161) | Retrospective | 57 | 34/23 | 83 | 36 | Cemented | Posterolateral | Greater trochanter reattachment device |
| Park 201524) | Retrospective | 22 | 18/4 | 76.9 | 42.84 | Cementless | Not mentioned | Dall-Miles cable or steel wire |
| Thakkar 201517) | Retrospective | 34 | 29/5 | 79.2 | 54.5 | Cemented | Posterolateral | 18 gauge wire with Ethibond |
| Celiktas 201533) | Prospective | 54 | 39/15 | 81.3 | 31 | Cementless | Posterolateral | Cable |
| Desteli 201538) | Prospective | 42 | 26/16 | 65±1.52 | 12, 24 | Cementless | Not mentioned | Not mentioned |
| Suh 201530) | Retrospective | 50 | 30/20 | 81.8±6.9 | 12 | Cementless | Not mentioned | Wire |
| Singh 201439) | Prospective | 25 | 11/14 | 64.92 | 12 | Cemented | Posterior | Tension band wiring, screws, K-wire |
| Kim 201431) | Retrospective | 143 | 84/23* | 84.9±3.5 | 45.6 | Cementless | Posterolateral | 16 gauge steel wire |
| 23/12† | 85.1±3.7 | |||||||
| Kumar 201318) | Prospective | 20 | 9/11 | 72.4 | 9 | Cemented | Posterior | Tension band wiring or suture |
| Park 201325) | Retrospective | 37 | 21/16 | 73.5 | 34.5 | Cementless | Anterolateral | Dall-miles cable or wire |
| Gu 201340) | Retrospective | 15 | 11/4 | 85 | >12 | Cemented | Posterior | Coated vicryl plus antibacterial suture or Ethibond suture |
| Abdelkhalek 201319) | Prospective | 20 | 12/8 | 69±5.59 | 24.2±5.71 | Cemented | Posterior | Tension band wiring |
| Shen 201237) | Retrospective | 60 | 47/13 | 78.2 | >24 | Cemented | Posterolateral | Wire |
| Karthik 201220) | Prospective | 28 | 19/9 | 79 | 50.4 | Cemented | Lateral, posterior | 18 gauge wire |
| cementless | ||||||||
| Fan 201229) | Retrospective | 72 | 45/27 | 76.5±8.3 | 39.7±13.3 | Cemented | Posterior | 16 gauge wire |
| Lee 201126) | Retrospective | 85 | 72/13 | 81.1 | 38.4 | Cementless | Posterolateral | 16 gauge wire |
| Choy 201032) | Retrospective | 40 | 32/8 | 78.8 | 40.5 | Cementless | Anterolateral | Wires or nonabsorbable sutures |
| Sinno 201021) | Retrospective | 48 | 34/14 | 78.6 | 22 | Cemented | Transgluteal lateral | Wire |
| Sancheti 201028) | Retrospective | 37 | 27/10 | 77.1 | 24.5 | Cemented | Posterior | Ethibond sutures or wire |
| Gu 200841) | Retrospective | 19 | 12/5 | 85 | >12 | Cemented | Lateral, posterior | Wire or cable |
| Kayali 200627) | Retrospective | 42 | 30/12 | 73±9 | 24±8.3 | Cementless | Posterior | Not mentioned |
| Kim 20052) | Prospective | 29 | 23/6 | 82.34±3.4 | 35 | Cementless | Posterolateral | Not mentioned |
| Rodop 200222) | Retrospective | 54 | 34/20 | 75.6 | 22.3 | Cemented | Posterolateral | Not mentioned |
| Chan 200023) | Retrospective | 55 | 44/10 | 84.2 | 13.6 | Cemented | Anterior | Wire |
| Green 198742) | Retrospective | 20 | 15/5 | 82.2 | 13.2 | Cemented | Posterolateral | Not mentioned |
![]()
Table 2
Clinical Results of Included Studies
| Study | Time to operation after injury (day) | Operation time (min) | Blood loss (mL) | Transfusion (unit) | Hospital stay (day) | Harris hip score |
|---|---|---|---|---|---|---|
| Mansukhani 20174) | 2.69±1.32 | 106.2±26.31 | 573±152.2 | 1.6±0.52 | 18.27±4.43 | |
| Camurcu 201736) | 2.4±1.9 | 83.4±33.7 | 412±170, 449±151 | 9.3±6.2 | ||
| Wada 201735) | 95.8 | |||||
| Thakur 201643) | 3 | 96 | 125 | 17.5 | 86.2 | |
| Chang 201634) | 97.3 | 66.9 | ||||
| Göçer 201611) | 80.4∥ | |||||
| 85.2¶ | ||||||
| 76.4** | ||||||
| Cui 20161) | 75 | 12 | 85.76±4.59 | |||
| Park 201524) | 3.6 | 67 | 293.2 | 40.4 | 77.4 | |
| Thakkar 201517) | 55 | 84.96 | ||||
| Celiktas 201533) | 86.6 | 1.2 | 5.3 | |||
| Desteli 201538) | 72±2.89 | 6±0.68 | ||||
| Suh 201530) | 73±17 | |||||
| Singh 201439) | 6.4 | 79.86±8.13 | ||||
| Kim 201431) | 54.3±12.8 | 247.9±82.4 | 1.6 | 18.7±5.6 | 82.3* | |
| 81.9† | ||||||
| Kumar 201318) | 116±14 | 13.3 | 75 | |||
| Park 201325) | 75.3 | 2.0 | ||||
| Gu 201340) | 50 | 310 | ||||
| Abdelkhalek 201319) | 5 | 140 | 1 | 16 | 83.5±4.2 | |
| Shen 201237) | 3.6±1.4 | 121±62 | 328±126 | 3.3 | 70.7±14.6 | |
| Karthik 201220) | 90 | 550 | 8 | |||
| Fan 201229) | 53.4±12.5 | 252±82.6 | 1.5 | 18.2±5.1 | 74.6±15.3 | |
| Choy 201032) | 7 | 80.6±9.3 | ||||
| Sinno 201021) | 112±29 | 192±85 | 1.37 | 6.3±1.8 | 82.76±4.78 | |
| Sancheti 201028) | 5.61±3.73 | 71 | 10.96 | 84.8±9.72 | ||
| Gu 200841) | 90 | |||||
| Kayali-200627) | 90±24 | 1.28±0.8 | 13±3.3 | |||
| Kim 20052) | 96±26 | 511±103 | 1.9±0.8 | 13±2.6 | 80±9.7 | |
| Rodop 200222) | 7.1 | 40 | 185±120 | |||
| Chan 200023) | 69 | 1.8 | 6.7 |
![]()
There were 19 studies that used cemented stem, 14 that used cementless stem, and two comparative studies that used both stems. Eleven studies were prospective studies, which used methods with wires, cables, and sutures for fixation of fracture fragments124111718192021222324252627282930313233343536373839404142).
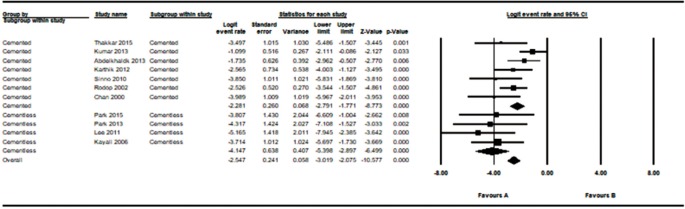
2. Over 1 cm Leg Length Discrepancy
A total of 11 comparative studies included an assessment on the frequency of LLD greater than 1 cm, of which seven used cemented stems17181920212223); the remaining four used cementless stems24252627). There was low evidence of heterogeneity across these studies (I2=52%; P=0.02) leading to the use of a random model. There were statistically significant differences in the occurrence of LLD greater than 1 cm between the cemented and cementless groups (logit event rate=−2.54; P<0.001) (Fig. 2).
3. Analysis of Treatment Results
1) Aseptic loosening
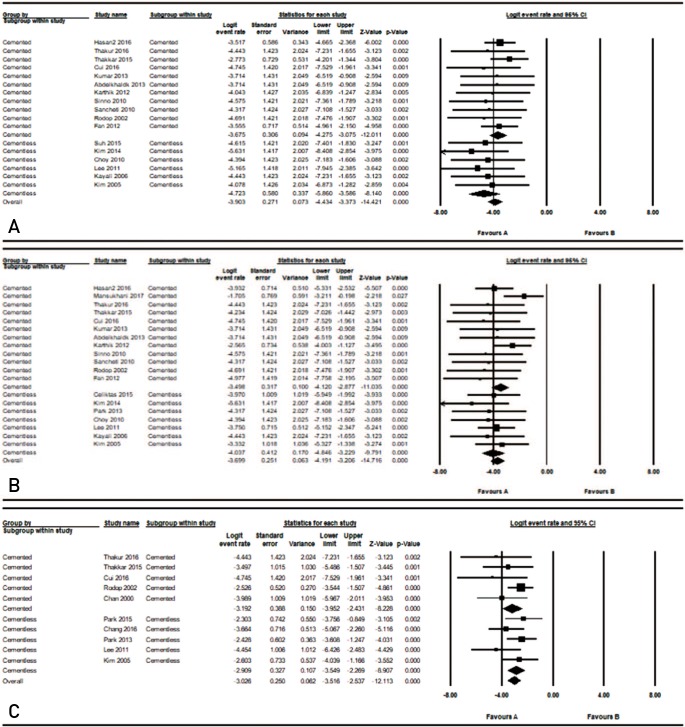
A total of 17 comparative studies included an assessment of aseptic loosening rates, of which 11 used cemented stems111171819202122282943); the remaining six used cementless stems22627303132). There was low evidence of heterogeneity across the studies (I2=0%; P=0.972) leading to the use of a fixed model. There were no statistically significant differences in the rates of aseptic loosening between the cemented and cementless groups (logit event rate=−3.90; P=0.110) (Fig. 3A).
2) Dislocation
A total of 19 comparative studies included an assessment of dislocation rates, of which 12 used this cemented stem1411171819202122282943); the remaining seven used cementless stems2252627313233). There was low evidence of heterogeneity across the studies (I2=0%; P=0.674) leading to the use of a fixed model. There were no statistically significant differences in dislocation rate between the cemented and cementless groups (logit event rate=−3.70; P=0.3) (Fig. 3B).
3) Greater trochanter nonunion
A total of 10 comparative studies included an assessment of greater trochanter nonunion rates, of which, five used cemented stems117222343); the remaining five used cementless stems224252634). There was low evidence of heterogeneity across the studies (I2=6%; P=0.385) leading to the use of a fixed model. There were no statistically significant differences in greater trochanter nonunion rate between the cemented and cementless groups (logit event rate=−3.03; P=0.577) (Fig. 3C).
4. Analysis of Complications
1) Superficial surgical site infection rate
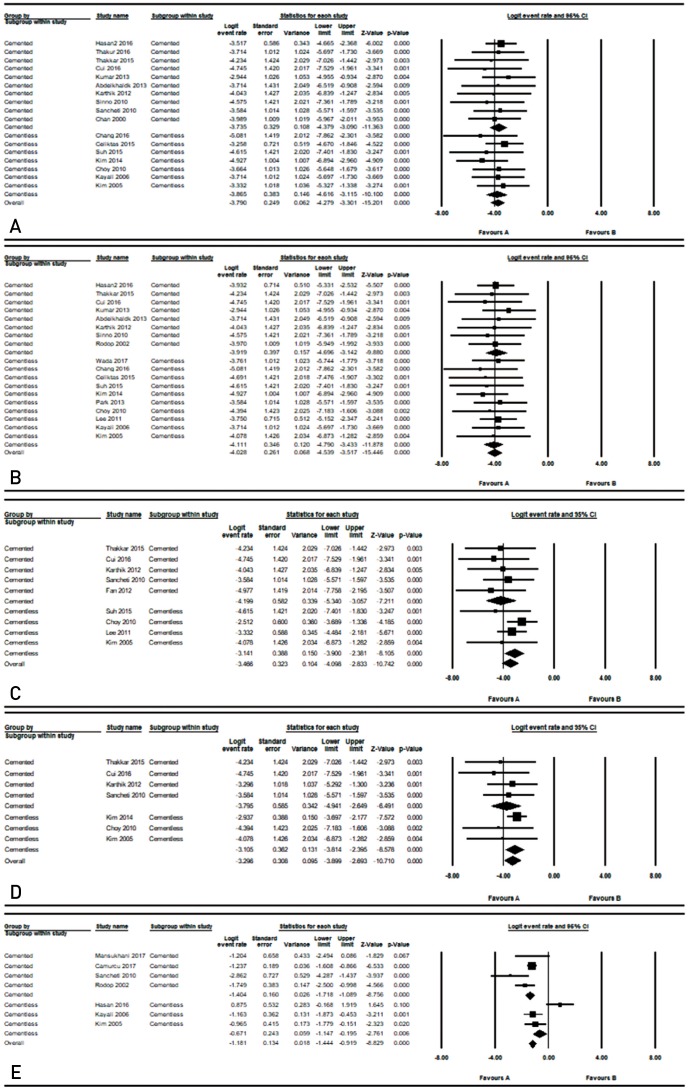
A total of 17 comparative studies included an assessment of superficial surgical site infection rates, of which 10 used cemented stems1111718192021232843); the remaining seven used cementless stems2273031323334). There was low evidence of heterogeneity across the studies (I2=0%; P=0.995) leading to the use of a fixed model. There were no statistically significant differences in superficial surgical site infection rate between the cemented and cementless groups (logit event rate=−3.79; P=0.795) (Fig. 4A).
2) Deep surgical site infection rate
A total of 18 comparative studies included an assessment of deep surgical site infection rates, of which eight used cemented stems111171819202122); the remaining 10 used cementless stems2252627303132333435). There was low evidence of heterogeneity across the studies (I2=0%; P=0.999) leading to the use of a fixed model. There were no statistically significant differences in superficial surgical site infection rate between the cemented and cementless groups (logit event rate=−4.03; P=0.715) (Fig. 4B).
3) Heterotopic ossification
A total of nine comparative studies included an assessment of heterotropic ossification rates, of which five used cemented stems120282943); the remaining four used cementless stems2263032). There was low evidence of heterogeneity across the studies (I2=0%; P=0.667) leading to the use of a fixed model. There were no statistically significant differences in HO rate between the cemented and cementless groups (logit event rate=−3.47; P=0.131) (Fig. 4C).
4) Periprosthetic fracture
A total of seven comparative studies included an assessment of periprosthetic fracture rates, of which four used cemented stems1172028); the remaining three studies used cementless stems23132). There was low evidence of heterogeneity across the studies (I2=74%; P=0.001) leading to the use of a random model. There were no statistically significant differences in periprosthetic fracture rate (logit event rate=−3.3; P=0.315) (Fig. 4D).
5) Mortality
A total of seven comparative studies included an assessment of 1-year mortality rates, of which, four used cemented stems4222836); the remaining three used cementless stems21117). There was low evidence of heterogeneity across the studies (I2=74%; P=0.012) leading to the use of a random model. There were no statistically significant differences in 1-year mortality rate between the cemented and cementless groups (logit event rate=−1.36; P=0.1) (Fig. 4E).
5. Risk Bias
The Newcastle-Ottawa scale was used to assess the quality of the selected studies. All included studies scored 6 to 8 points, indicating relatively high quality.
Go to :
DISCUSSION
With an increase in life expectancies around the globe, and osteoporosis-a progressive condition which largely affects the elderly-hip fractures are occurring more frequently and of significant concern, particularly to elderly individuals438). Compared to other types of fractures, those affecting the hip in elderly patients involves high cost, and it is expected to become a major worldwide health problem in the future4546). Among all hip fractures in elderly patients, intertrochanteric fractures are known to account for 45% to 50%; more than half of these are unstable, with comminution of the posteromedial buttress, exceeding a simple lesser trochanteric fragment or those with subtrochanteric extension847). Similar to other hip fractures in elderly patients, unstable intertrochanteric fractures are associated with high morbidity and mortality rates; while it is known that early ambulation following strong fracture fixation may help fervent morbidity and mortality, the best treatment approach for these fracture types remain a challenge.
Internal fixation is widely used as the primary treatment method for intertrochanteric fractures48). Although some studies have reported favorable treatment outcomes, others have reported high failure rates in cases of unstable intertrochanteric fractures. Studies in the literature reported cut-out rates of 8% for hip screws, 20% for mal-union and failure rate of osteosynthesis, and 36% to 54% for incidence of coxa vara, delayed healing, or nonunion495051). Consequently, some studies reported that hip arthroplasty may shorten the weight-bearing time, reduce the incidence of implant-related complications and improve hip function when compared with internal fixation by Gamma nails, dynamic hip screws, and proximal femoral nails5253).
Prosthesis fixation using cement-which enables the patients to ambulate faster-can be useful since fracture injury, operation damage and catabolic effect due to misuse can influence reduction of bone mineral quantity and the functional recovery1254). Using bone cement when conducting arthroplasty varies according to bone conditions of the patiens, surgeon techniques, and preferences. Many studies analysed outcomes with long-term follow-up and there appears to be no significant difference between cemented and cementless hemiarthroplasty in terms of morbidity, mortality or length of hospital stay for femoral neck fractures145455). Furthermore, these studies report that functional outcomes of patients treated with cementless hemiarthroplasty tends to be less favorable than those with cemented hemiarthroplasty. However, research on the choice between cemented or cementless prosthesis for treatment of unstable intertrochanteric fractures is still lacking. The routine use of cement in elderly patients has been reported to be a technically more demanding procedure and may be associated with cardiopulmonary complications5657). Using cement is even more difficult in unstable intertrochanteric fracture accompanied by comminution of the posteromedial buttress, exceeding a simple lesser trochanteric fragment or those with subtrochanteric extension; since this can result in larger amount of blood loss and longer operation times, it may lead to higher morbidity rates due to increased cardiopulmonary loading. However, in this study, there was no difference in 1-year mortality rate, and overall mortality rate between cemented and cementless groups. Previous studies have shown that cemented hemiarthroplasty with or without calcar replacement remains a good option in elderly patients with intertrochanteric femur fractures; the literature reviewed in this study revealed that more studies used cemented stems than cementless stems1958). Despite this, many orthopedic surgeons remain concerned about increased mortality from fat embolization due to increased intramedullary pressure during cementation145455596061). Moreover, according to a comparative study by Cankaya et al.13) on cemented and cementless stems in unstable intertrochanteric fractures, cement was reported to be the factor that increased mortality. There are, however, a number of other studies which report that the use of cement does not increase mortality145960). Intertrochanteric fractures have larger fracture surfaces and more bleeding, and compared to femoral neck fractures, intertrochanteric fractures generally occur in patients with poorer health status. Although the use of cement may be a potential factor leading to an increased frequency of complications, including mortality, additional studies are needed on this topic62).
There are several factors involved in HO, including hypertrophic osteoarthritis, ankylosing spondylitis, and male gender6364). Among them, surgical approach is one of the important factors that cause HO63). Compared to anterior or anterolateral approaches, the posterior approach to the hip joint involves less abductor manipulation, which may influence the occurrence of HO. Similarly, when compared to neck fractures, unstable intertrochanteric fractures require a significant amount of manipulation of fragments that are attached to the abductor and wire or plate for fixation, especially when cement is used because of longer operation time. It is believed that such differences between the two groups occurred because of these factors, but there were no statistically significant differences in the HO occurrence rates in this study. Moreover, considering that the studies included in the present study reported HO rate of up to 10%, while other studies had reported HO occurrence rate of 25% for femoral neck fractures, it is believed that performing bipolar hemiarthroplasty for unstable intertrochanteric fracture does not increase HO rate. However, additional studies are needed on this topic.
Compared to femoral neck fractures, unstable intertrochanteric fractures may require fixation of fracture; in our study, union status was not statistically different among the cement vs. cementless groups. Moreover, additional studies are deemed necessary since there were only few reports including the healing status of the fracture site.
Complication rates associated with infection, dislocation, aseptic loosening, and periprosthetic fracture were not significantly different between the cement and cementless groups. The studies reviewed did not have long-term follow-ups since the studies involved elderly patients, and as a result, there were no differences in aseptic loosening rates-a pattern similar to studies that compared cemented and cementless stems in femoral neck fracture cases1465). However, the rate of LLD greater than 1 cm was significantly higher in the cemented group compared with the cementless group. Stable femoral stem fixation in the proximal femoral medullary canal and protrusion of the femoral implant from the femoral bone by a vertical distance are essential for proper leg length. Various anatomical markers and radiological methods have been used for restoration of leg length66). It is considered difficult to obtain a proper leg length when performing cemented total hip arthroplasty in a state where anatomical markers are damaged considerably. Therefore, additional comparative studies are needed on this topic as well.
Our review has several limitations. First, although this study reviewd studies that performed bipolar hemiarthroplasty for unstable intertrochanteric fractures, most were retrospective case series studies or studies that made comparisons against an internal fixation group. Except for two studies, there were no randomized controlled trial or comparative studies on cementless and cemented groups. In such a case, studies with positive or statistically significant results would be expected to be over-represented in our review, as such studies were more likely to be published, particularly in the English language. Second, the validity of our results is limited by the low quality of the included studies; double-blinding was unattainable for most of the trials, which may decrease the strength of our conclusions. Third, there is the potential for bias because of high heterogeneity in some comparisons, which may have affected the pooled results. Studies brought together in a meta-analysis will inevitability differ, and any kind of variability among studies may be termed heterogeneity. The included studies had clinical heterogeneity caused by variability in the participants (e.g., age, gender, comorbidities, preoperative ambulatory status), interventions (e.g., instrumentation from different manufacturers, different surgeons) and outcomes (e.g., selective reporting, data deficiency), and methodological heterogeneity caused by variability in study design and risk of bias. Fourth, it is not sufficient to analyze related factors of surgical complications, such as prosthesis position and comorbidity.
Go to :
CONCLUSION
Cemented bipolar hemiarthroplasty and cementless bipolar hemiarthroplasty performed on elderly patients with unstable intertrochanteric fracture showed similar rates of mortality and complications. However, the rate of LLD greater than 1 cm was significantly higher in the cemented group than in the cementless group.
Go to :
 XML Download
XML Download